What is cholesterolosis
Reading File
Finding Sources
Finding Sources
Searching the Web
cholesterolosis gallbladder pathology definition
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information. Let me compile the full answer.
Cholesterolosis
Cholesterolosis (also called "strawberry gallbladder") is an acquired histological abnormality of the gallbladder characterized by excessive accumulation of cholesterol esters and triglycerides within epithelial macrophages (foam cells) in the lamina propria of the gallbladder mucosa. It is classified as one of the "hyperplastic cholecystoses", alongside adenomyomatosis.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1280
- Bailey and Love's Short Practice of Surgery, p. 5608
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, p. 2149
Schematic: Normal gallbladder vs. cholesterolosis vs. cholesterol polyp
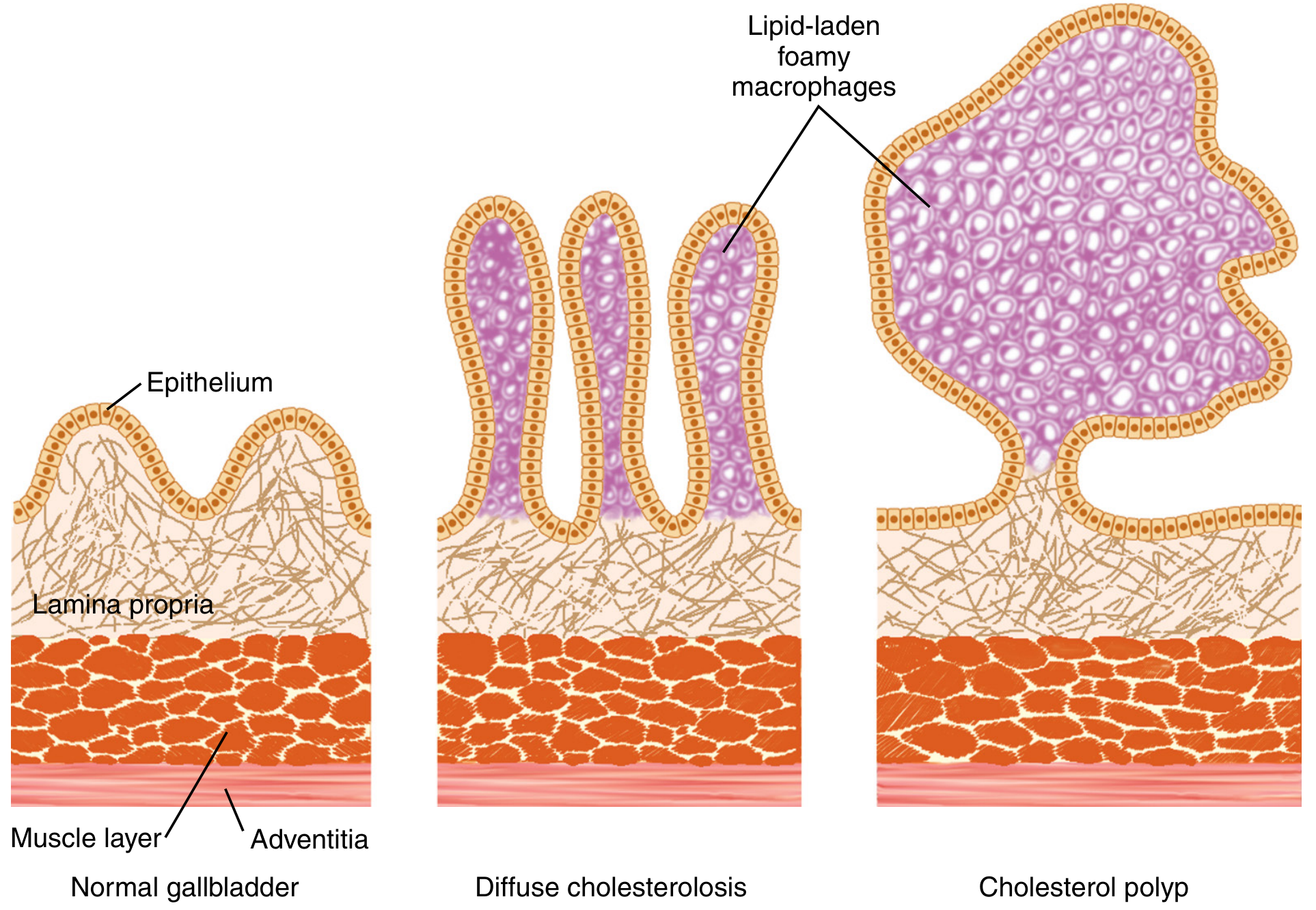
Patterns of Lipid Deposition
There are four recognized patterns:
| Pattern | Description | Frequency |
|---|---|---|
| Diffuse | Lipid distributed throughout the entire epithelial lining, ending abruptly at the cystic duct | ~80% |
| Cholesterol polyps | Excess lipid confined to one or more polypoid excrescences projecting into the lumen | ~10% |
| Combined | Cholesterol polyps on a background of diffuse cholesterolosis | ~10% |
| Focal | Lipid deposition limited to a small mucosal area | Rare |
Gross Appearance
- The opened gallbladder shows pale yellow linear streaks running longitudinally over a hyperaemic mucosa, giving rise to the classic term "strawberry gallbladder."
- In about two-thirds of cases, the lipid nodules are <1 mm; the remainder form larger polypoid lesions.
- Gallstones co-exist in ~50% of surgically resected cases, but only ~10% of autopsy cases - showing the two processes are largely independent.
Histology (Microscopic Appearance)
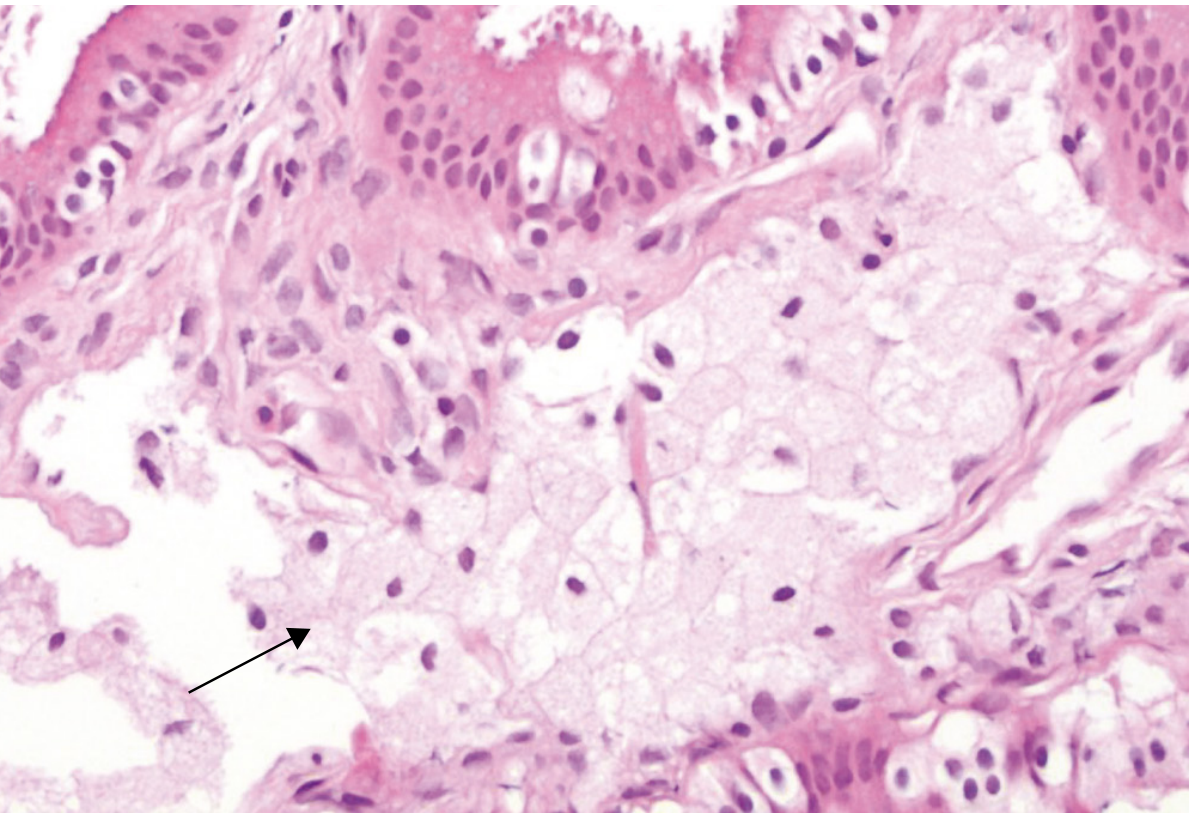
- Mucosal hyperplasia (villous type) is invariably present, marked in ~50% of cases.
- The hallmark is an abundance of foam cells (macrophages stuffed with lipid droplets) within elongated villi.
- In mild cases, foam cells are limited to villous tips (producing linear streaks on gross exam); in severe cases, they fill entire villi and spill into the submucosa.
- Small yellow particles called lipoidic corpuscles (detached foam cell masses) may float in the bile.
Pathogenesis
The exact cause remains unclear. The leading hypothesis is that the bile becomes supersaturated with cholesterol (similar to cholesterol gallstone disease), and cholesterol is absorbed by mucosal epithelial cells, then transferred to subepithelial macrophages which become foam cells. Increased acyl-CoA cholesterol ester acyltransferase (ACAT) activity in the gallbladder mucosa has been implicated. Importantly, cholesterolosis is not associated with elevated serum cholesterol levels.
Epidemiology
- Found in 5-40% of autopsy gallbladders (depending on gross vs. microscopic criteria); ~12% in large autopsy series.
- Frequency rises to ~18% in surgically resected gallbladders; up to 38% in gallbladders from bariatric surgery patients (obesity is a risk factor).
- Like cholesterol gallstone disease: uncommon in children, marked female predilection until age 60, after which gender differences lessen.
- No clear racial or geographic differences reported.
Clinical Features
- Most cases are asymptomatic and discovered incidentally on pathologic examination after cholecystectomy.
- Occasionally: dull, vague right upper quadrant or epigastric pain resembling biliary colic.
- Polypoid forms have been associated with biliary pain and rarely acute pancreatitis (from detachment of cholesterol fragments into the bile duct).
- Not associated with jaundice, fever, or signs of cholecystitis unless coexisting gallstones or inflammation are present.
Diagnosis
- Most commonly an incidental pathologic finding after cholecystectomy.
- Ultrasound (USG): may show a non-mobile, non-shadowing echogenic lesion (polyp) in the gallbladder lumen. Differential is adenomatous polyp; interval follow-up is recommended to confirm stability.
- Diagnosis can sometimes be made at laparoscopy by observing the characteristic mucosal appearance through the serosal surface (~20% of cases).
Treatment
Because cholesterolosis is almost always diagnosed only after gallbladder resection, treatment is rarely a separate consideration. In the rare case where polypoid cholesterolosis is diagnosed pre-operatively on ultrasound, cholecystectomy is advised if there is diagnostic dilemma (to rule out adenomatous or malignant polyp), but observation with follow-up imaging is appropriate for small, stable, asymptomatic lesions.
This is a shared conversation. Sign in to Orris to start your own chat.