Sibsons fascia
Reading File
Finding Sources
Searching the Web
Sibson's fascia anatomy suprapleural membrane clinical significance
Reading File
Reading File
Reading File
Loading Image
Loading Image
Sibson's Fascia (Suprapleural Membrane)
Definition
Sibson's fascia is the suprapleural membrane - a dome-shaped thickening of the endothoracic fascia that covers the pleural cupola (apex of the lung) as it projects above the thoracic inlet into the neck.
Anatomy
Structure:
- A condensation of the endothoracic fascia, which is the fibrous connective tissue lining the inner surface of the thoracic wall (analogous to the transversalis fascia of the abdomen)
- Dome-shaped, covering the apex of the cervical pleura
- Some authors describe it as being formed partly by the alar fascia (a layer of the prevertebral fascia) rather than purely the endothoracic fascia
Attachments:
- Medially: transverse process of C7 vertebra
- Anterolaterally: inner border (medial margin) of the 1st rib
- It arches superiorly over the pleural apex like a tent
Relations:
- Inferiorly: cervical pleura and apex of the lung
- Superiorly: subclavian artery (which grooves the first rib posterior to the anterior scalene insertion)
- The scalene muscles (anterior, middle, posterior) form a muscular dome surrounding the apex, and their fascia (scalene fascia, a continuation of the prevertebral fascia) contributes to and blends with Sibson's fascia at this region
- The C8 and T1 nerve roots unite behind Sibson's fascia (and beneath the subclavian artery) to form the lower trunk of the brachial plexus
Here is the anatomy diagram from the THIEME Atlas of Anatomy showing Sibson's fascia in context:
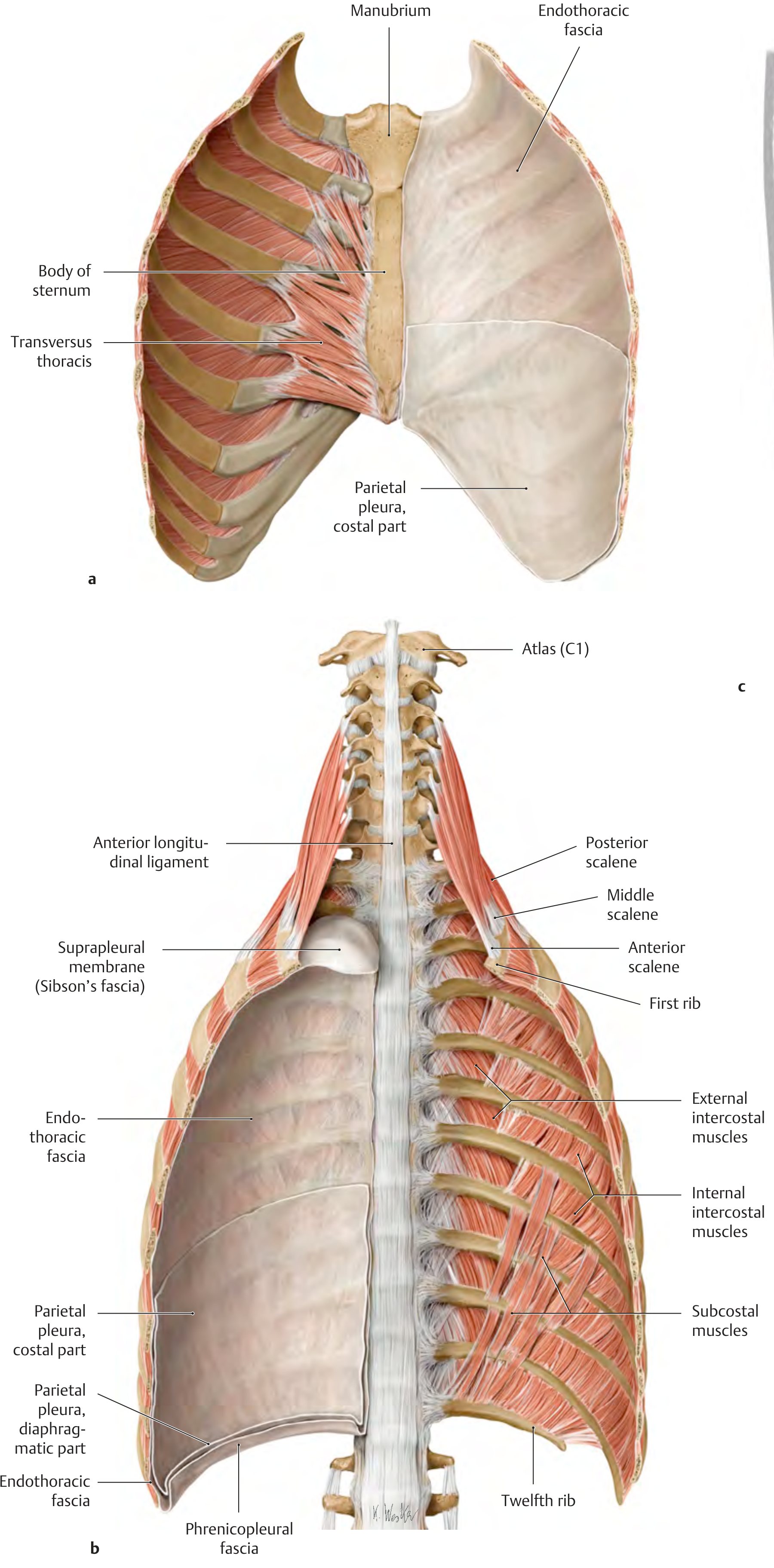
THIEME Atlas of General Anatomy, p. 194 - showing the suprapleural membrane (Sibson's fascia) at the apex of the thorax, with the endothoracic fascia and phrenicopleural fascia below
Related Fasciae of the Thorax (for context)
| Fascial layer | Location | Notes |
|---|---|---|
| Endothoracic fascia | Lines entire thoracic wall | Between deep thoracic muscles and parietal pleura |
| Sibson's fascia | Over pleural apex | Thickened part of endothoracic fascia |
| Phrenicopleural fascia | Inferior thorax | Connects diaphragmatic pleura to upper diaphragm |
Functions
- Supports the pleural dome: Holds the apex of the lung in position above the 1st rib, preventing it from prolapsing superiorly
- Resists intrathoracic pressure changes: Mechanically buffers the negative pressure transmitted to the apex during inspiration
- Protects the cervical pleura: Acts as a barrier protecting the pleural apex from above
Clinical Relevance
1. Thoracic outlet syndrome (TOS)
Sibson's fascia is in close relation to the subclavian vessels and lower trunk of the brachial plexus (C8-T1). Fibrous bands in this region (sometimes called "Sibson's bands") can compress the lower trunk, causing:
- Numbness/weakness in ulnar nerve territory (C8-T1 distribution)
- Weak or absent radial pulse (subclavian artery compression)
- Venous obstruction (subclavian vein)
2. Brachial plexus anatomy landmark
The C8/T1 roots unite behind Sibson's fascia to form the lower trunk, making it a surgical landmark for procedures at the thoracic outlet. - Localization in Clinical Neurology, 8e, p. 188
3. Cervical rib effects
A cervical rib or fibrous band elevates and tenses Sibson's fascia, angulating and compressing the lower trunk of the brachial plexus against it.
4. Surgical access (first rib resection / scalenectomy)
During thoracic outlet decompression surgery, the scalene fascia and Sibson's fascia must be carefully dissected to protect the phrenic nerve (which lies on the anterior scalene deep to this fascia) and the pleural dome. - Fischer's Mastery of Surgery, 8e, p. 7024
5. Pneumothorax risk
Because the pleural apex sits directly below Sibson's fascia, any penetrating injury or needle procedure at the root of the neck (e.g., subclavian line, scalene block, supraclavicular brachial plexus block) risks traversing this membrane and causing an apical pneumothorax.
Sources:
- THIEME Atlas of General Anatomy & Musculoskeletal System, p. 193-194
- Fischer's Mastery of Surgery, 8th ed., p. 7024
- Localization in Clinical Neurology, 8th ed., p. 188
Pleural resses
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Pleural Recesses (Pleural Sinuses)
Pleural recesses are potential spaces within the pleural cavity where two layers of parietal pleura are reflected against each other, forming pocket-like spaces that the lung does not occupy during quiet respiration. They expand to accommodate the lung during deep/forced inspiration and serve as sites where fluid can collect pathologically.
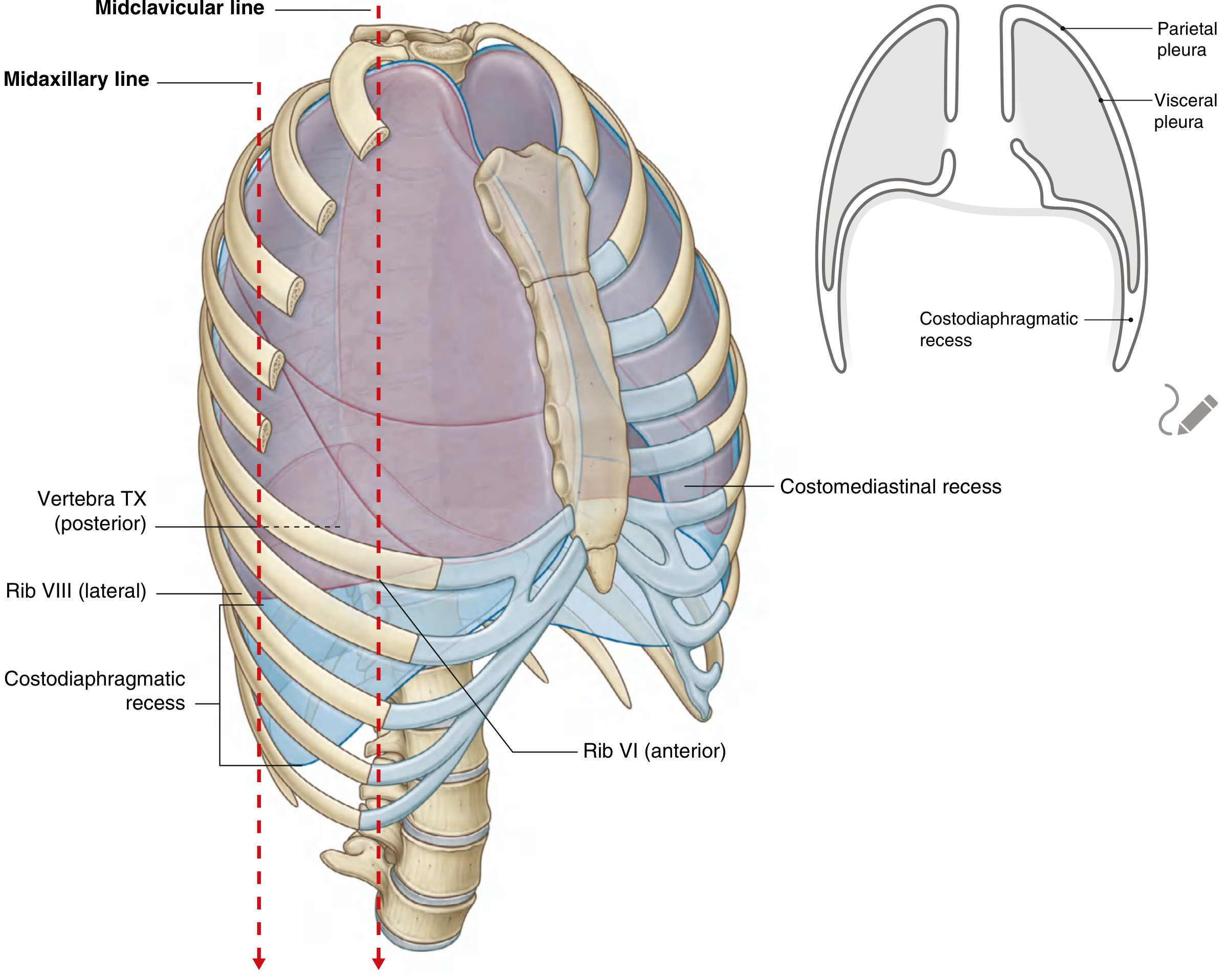
Gray's Anatomy for Students - showing costodiaphragmatic and costomediastinal recesses, p. 202-203
Types of Pleural Recesses
There are two main recesses:
1. Costodiaphragmatic Recess
- Formed by: Costal pleura reflected onto diaphragmatic pleura (at their junction inferiorly)
- Location: Inferolateral portion of the pleural cavity, bilaterally
- Size: The largest and clinically most important recess
- Shape: Deepest posteriorly (like a gutter running around the lower thorax)
- Deepest during forced expiration; shallowest (smallest) during forced inspiration when the lung descends to fill it
Surface projection (quiet respiration):
| Reference line | Inferior lung margin | Inferior pleural margin |
|---|---|---|
| Midclavicular line | Rib VI | Rib VIII |
| Midaxillary line | Rib VIII | Rib X |
| Paravertebral/scapular line | T10 vertebra | T11-T12 vertebra |
So the costodiaphragmatic recess spans approximately 2 rib spaces between the lung border and pleural border at any given vertical line. - Color Atlas of Human Anatomy Vol. 2, p. 224
2. Costomediastinal Recess
- Formed by: Costal pleura reflected onto mediastinal pleura (anteriorly, behind the sternum)
- Location: Anterior chest, posterior to the sternum and costal cartilages
- Asymmetry: The left costomediastinal recess is significantly larger than the right, because the left lung has a cardiac notch (the heart occupies that space, so the lung is indented and the pleural recess is wider)
- The right costomediastinal recess is narrow
Summary Table
| Feature | Costodiaphragmatic | Costomediastinal |
|---|---|---|
| Pleurae forming it | Costal + diaphragmatic | Costal + mediastinal |
| Location | Inferior, lateral | Anterior, behind sternum |
| Size | Largest recess | Smaller; left > right |
| Asymmetry | Both sides roughly equal | Left larger (cardiac notch) |
| Deepest when | Forced expiration | - |
| Filled by lung when | Deep/forced inspiration | Deep/forced inspiration |
Functions
- Respiratory reserve space: Allows lung expansion during deep inspiration
- Fluid reservoir: Pathological fluid (pleural effusion) first collects here before compressing the lung - the costodiaphragmatic recess is the most dependent, so fluid gravitates here first
- Percussion sign: Dullness to percussion in the lower chest (rib VIII-X laterally) when fluid fills the costodiaphragmatic recess
Clinical Relevance
1. Pleural effusion
Fluid from any cause (infection, malignancy, heart failure, hepatic disease, pulmonary embolism) accumulates first in the costodiaphragmatic recess. As volume increases, the lung is progressively compressed. Fluid is aspirated (thoracocentesis) from this region. - Gray's Anatomy for Students, p. 203
2. Thoracocentesis / Chest drain insertion
- Safe site: 4th-5th intercostal space, anterior to midaxillary line
- Inserting below the 5th intercostal space risks entering the costodiaphragmatic recess at its lower limit, and going too low risks passing through the recess entirely into the liver (right) or spleen (left)
- The needle must pass just above the upper border of the lower rib to avoid the intercostal neurovascular bundle (VAN) which runs in the costal groove
3. Surgical entry into the chest (thoracotomy)
- The sharp angle of the costodiaphragmatic recess means entry too low (or an incision continuing inferiorly) can breach the diaphragm and enter the abdomen - a major complication. - Fischer's Mastery of Surgery, 8e
4. Kidney relations
- The costodiaphragmatic recess sits between the 12th rib and the posterior surface of the kidney - this is why a renal biopsy or nephrectomy from behind risks entering the pleural cavity if the approach is too high. - Color Atlas of Human Anatomy Vol. 2
5. Pleurisy
Inflammation of the costal or diaphragmatic pleura (which are pain-sensitive, supplied by intercostal and phrenic nerves respectively) produces sharp, localised pain that worsens on breathing - referred to the shoulder tip if the diaphragmatic pleura is involved (via the phrenic nerve, C3-C5).
Sources:
- Gray's Anatomy for Students, pp. 202-203
- Color Atlas of Human Anatomy, Vol. 2 (Internal Organs), p. 224
- Fischer's Mastery of Surgery, 8th ed.
- Mulholland & Greenfield's Surgery, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.