Cholecystitis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cholecystitis"[MeSH Terms] AND ("management" OR "treatment")
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Cholecystitis
Cholecystitis is inflammation of the gallbladder. It is one of the most common indications for abdominal surgery in the United States, and its epidemiologic distribution closely parallels that of gallstone disease.
Classification
| Type | Key feature |
|---|---|
| Acute calculous | Obstruction by gallstone (~90% of acute cases) |
| Acute acalculous | No stone; stasis/ischemia in critically ill (5-12%) |
| Chronic | Repeated bouts; fibrosis; almost always with stones |
| Emphysematous | Gas-forming organisms; diabetics/elderly men |
| Gangrenous | Necrosis of gallbladder wall; most severe |
Acute Calculous Cholecystitis
Pathogenesis
Acute cholecystitis begins when a stone becomes persistently embedded in the cystic duct (rather than causing transient obstruction as in biliary colic). Three parallel mechanisms drive the inflammatory response:
- Mechanical - increased intraluminal pressure and distension cause mucosal ischemia
- Chemical - phospholipase A released from the mucosa converts lecithin to lysolecithin, which is toxic to the epithelium; the glycoprotein mucous layer is disrupted, exposing mucosa to bile salt detergent action; prostaglandins E and F2α amplify mucosal inflammation
- Bacterial - enteric organisms (E. coli, Klebsiella, Streptococcus, Clostridium) are cultured from gallbladder bile in 50-85% of patients, but are considered a secondary event, not the initiator
The role of prostaglandins is supported by evidence that diclofenac (a prostaglandin synthetase inhibitor) given early resolves biliary pain and prevents acute cholecystitis from developing - Sleisenger and Fordtran's, p. 1242.
Clinical Features
- Pain: RUQ or epigastric pain that is steady and severe, lasting >6 hours (contrast with biliary colic, which resolves within 5 hours). Radiates to the right scapula or interscapular area.
- Fever: low-grade fever typical; temperature >102°F (>39°C) suggests gangrene or perforation
- Nausea/vomiting: common; may cause volume depletion
- Murphy's sign: during deep palpation of the RUQ, the patient arrests inspiration when the inflamed gallbladder descends to meet the examiner's hand. Positive predictive value >90% for acute cholecystitis when gallstones are also present.
- Palpable gallbladder: in ~25-50% of patients, especially on first attack. Repeat attacks cause scarring that prevents distension.
- Jaundice: mild (bilirubin <4 mg/dL) in ~20% overall, up to 40% in elderly. Bilirubin >4 mg/dL raises concern for choledocholithiasis or Mirizzi syndrome.
- Approximately 75% of patients report prior attacks of biliary pain before their first episode of acute cholecystitis. - Sleisenger and Fordtran's, p. 1242
Laboratory Findings
| Test | Finding |
|---|---|
| WBC | 10,000-15,000/mm³ with left shift |
| WBC >15,000 | Suggests empyema or perforation |
| Serum bilirubin | Mildly elevated (<4 mg/dL) in <50% |
| Bilirubin >4 mg/dL | Suggests bile duct stones or Mirizzi syndrome |
| ALT/AST, ALP | Mildly elevated; up to 5-fold |
| Amylase/lipase | Mildly elevated nonspecifically; >1000 U/L suggests pancreatitis |
- Harrison's Principles of Internal Medicine, 22E (2025), p. 2775
Imaging
Ultrasound (US) is the first-line and most useful study:
- Identifies gallstones in 90-95% of cases
- Gallbladder wall thickening >4 mm (loses specificity in ascites/hypoalbuminemia)
- Pericholecystic fluid
- Sonographic Murphy sign: focal gallbladder tenderness under the US probe
HIDA scan (hepatobiliary scintigraphy): highly sensitive and specific (~95%). Non-visualization of the gallbladder (isotope appears in bile duct and small bowel but not the gallbladder within 60 minutes) confirms cystic duct obstruction. A normal scan effectively excludes acute cholecystitis.
CT: shows gallbladder wall thickening, pericholecystic inflammation; useful when US is inconclusive and for detecting complications (gangrene, perforation, emphysematous cholecystitis).
Morphology (Pathology)
Acute cholecystitis:
- Enlarged, tense gallbladder; bright red or violaceous (from subserosal hemorrhage)
- Serosal fibrinous or fibrinopurulent exudate
- In 90% of cases, stones obstruct the neck or cystic duct
- Lumen contains cloudy/turbid bile, fibrin, blood, pus
- Empyema: lumen filled predominantly with pus
- Gangrenous cholecystitis: green-black necrotic wall
- Histology: edema, leukocytic infiltration, vascular congestion, abscess formation, gangrenous necrosis
Chronic cholecystitis:
- Marked subepithelial and subserosal fibrosis
- Lymphocytic infiltrate in the wall (when not superimposed acute)
- Rokitansky-Aschoff sinuses: outpouchings of mucosal epithelium through the gallbladder wall - a hallmark finding
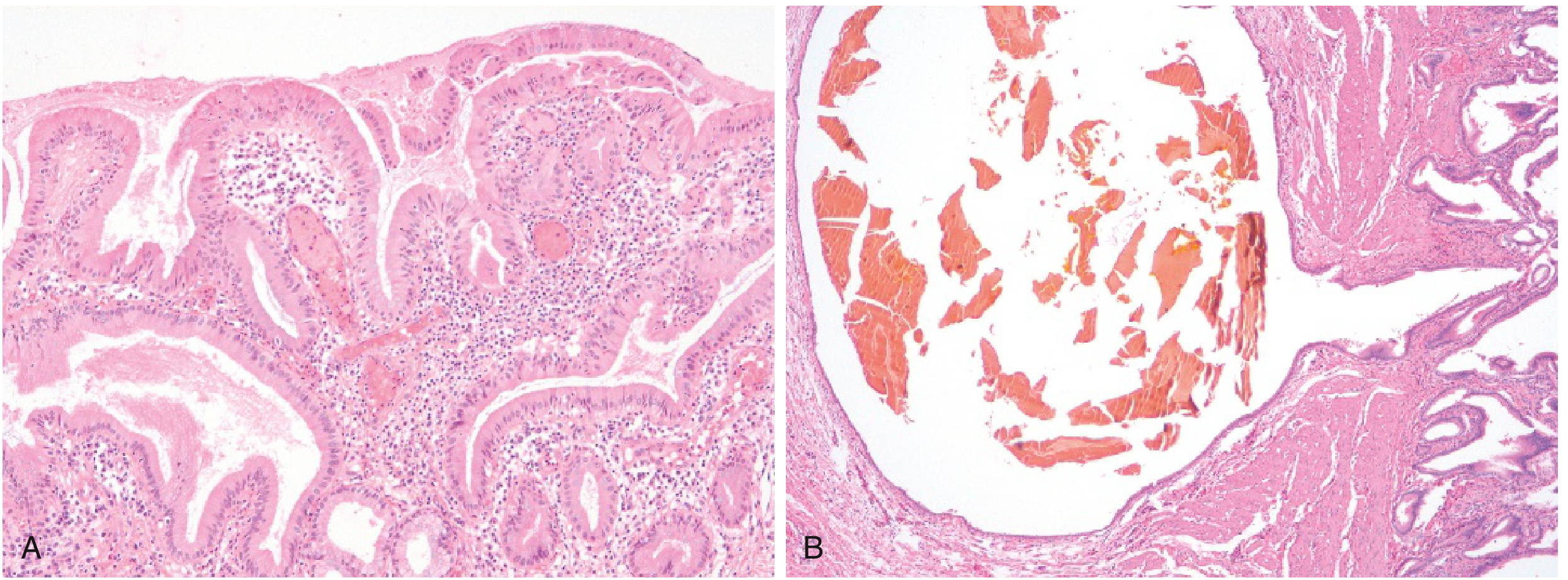
FIG. 14.43 Chronic cholecystitis. (A) Gallbladder mucosa infiltrated by chronic inflammatory cells. (B) Rokitansky-Aschoff sinus containing a fragmented bile pigment stone. - Robbins & Kumar Basic Pathology, p. 633
Acute Acalculous Cholecystitis
Accounts for 5-12% of acute cholecystitis cases. Thought to result from gallbladder stasis and ischemia rather than stone obstruction.
Predisposing conditions:
- Major surgery or severe trauma (motor vehicle crashes)
- Severe burns
- Sepsis
- Prolonged fasting / parenteral nutrition
- Postpartum after prolonged labor
- Vasculitis, cholesterol emboli
- DM, adenocarcinoma, gallbladder torsion
Important organisms in unusual cases: Leptospira, Salmonella, Vibrio cholerae, parasitic infestations.
The complication rate exceeds that of calculous cholecystitis. Management depends on early diagnosis and prompt surgical or percutaneous drainage. - Harrison's 22E, p. 2775
Emphysematous Cholecystitis
- Acute cholecystitis complicated by ischemia/gangrene + gas-producing organisms
- Common organisms: Clostridium perfringens/welchii (anaerobes), E. coli (aerobes)
- Most common in elderly men and diabetics
- Diagnosis: plain film or CT showing gas in the gallbladder lumen, gas dissecting the wall (ring sign), or pericholecystic gas
- Carries high morbidity and mortality; urgent surgery + antibiotics mandatory
Natural History
- Untreated acute cholecystitis pain resolves in 7-10 days; often remits within 48 hours of hospitalization
- ~83% resolve without complication medically
- Complications occur in ~17%: gangrenous cholecystitis (7%), empyema (6%), perforation (3%), emphysematous (<1%)
- Of those who remit medically: ~25% recur within 1 year, ~60% within 6 years
- Therefore acute cholecystitis is best treated by early surgery when possible
Complications
- Empyema of the gallbladder (pus-filled lumen)
- Gangrenous cholecystitis with risk of perforation
- Perforation - local abscess or diffuse peritonitis
- Cholangitis/sepsis from bacterial superinfection
- Biliary-enteric (cholecystoenteric) fistula - drainage into adjacent bowel, entry of air/bacteria into biliary tree, risk of gallstone ileus
- Mirizzi syndrome - impacted stone in cystic duct compresses the common hepatic duct, causing jaundice
Treatment
Acute Cholecystitis
- IV fluids, NPO, analgesia (NSAIDs - ketorolac, diclofenac are preferred; also reduce prostaglandin-driven inflammation)
- Antibiotics covering enteric gram-negatives and anaerobes
- Early laparoscopic cholecystectomy is the treatment of choice - ideally within 72 hours to 1 week of symptom onset
- Conversion to open surgery in ~5%; death rate <0.1%; bile duct injury rate 0.2-0.6%
High-risk/non-surgical candidates: Percutaneous cholecystostomy (gallbladder drainage) followed by interval cholecystectomy once the patient is stabilized.
A recent 2025 systematic review and meta-analysis (PMID 40483437) comparing percutaneous treatment vs. cholecystectomy found that both approaches are viable, with percutaneous drainage being preferred for high-risk surgical patients.
A 2024 meta-analysis (PMID 39607476) challenged the traditional "7-day barrier," showing that early laparoscopic cholecystectomy remains safe even beyond 7 days of symptom onset.
Chronic Cholecystitis
- Elective laparoscopic cholecystectomy is definitive
- Medical dissolution with UDCA (10-15 mg/kg/d) is an option only for radiolucent stones <5 mm in a functioning gallbladder; complete dissolution in ~50% within 6-24 months; high recurrence rate (30-50% over 3-5 years)
Chronic Cholecystitis
Develops with or without a prior history of acute attacks. Almost always associated with gallstones, though the stones appear to create a milieu of bile supersaturation rather than directly causing inflammation. Microorganisms (E. coli, enterococci) cultured in ~one-third of cases.
Chronic symptoms: recurrent RUQ pain, fatty food intolerance, bloating. Gallbladder may be contracted (fibrotic) and non-functioning on imaging.
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, pp. 1241-1244
- Harrison's Principles of Internal Medicine, 22E (2025), pp. 2774-2776
- Robbins & Kumar Basic Pathology (Robbins Pathology), pp. 632-633
- Tintinalli's Emergency Medicine: A Comprehensive Study
- Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.