Total thyroidectomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have comprehensive information. Let me compile a complete, well-structured answer.
Total Thyroidectomy
Total thyroidectomy is the excision of all (or nearly all) visible thyroid tissue from both lobes. It is one of the most common surgical procedures in the United States, with over 130,000 thyroidectomies performed annually.
Definition and Nomenclature
| Extent of Resection | Description |
|---|---|
| Total thyroidectomy | All or nearly all visible thyroid gland excised bilaterally |
| Near-total thyroidectomy | Less than 1 g of remnant left at the ligament of Berry |
| Subtotal thyroidectomy | 3-5 g remnant left (less common today) |
| Lobectomy / Hemithyroidectomy | Entire lobe on one side + isthmus + pyramidal lobe |
| Isthmusectomy | Resection of isthmus and pyramidal lobe only |
- Sabiston Textbook of Surgery, p. 1522
Indications
- Thyroid cancer - differentiated, medullary, or anaplastic thyroid carcinoma
- Hyperthyroidism - Graves disease, toxic multinodular goiter, when nonsurgical management has failed or is not preferred
- Goiter - with or without local compressive symptoms (tracheal compression, dysphagia, dyspnea)
- Thyroid nodules - indeterminate or suspicious on FNA biopsy
- Current Surgical Therapy 14e, p. 898; Sabiston Textbook of Surgery, p. 1522
Surgical Anatomy
A thorough knowledge of anatomy is foundational to safe thyroidectomy.
Vascular supply:
- Each lobe is fed by two arteries: the superior thyroid artery (branch of external carotid) and the inferior thyroid artery (from thyrocervical trunk)
- Venous drainage via three named veins: superior, middle, and inferior thyroid veins
Critical nerves:
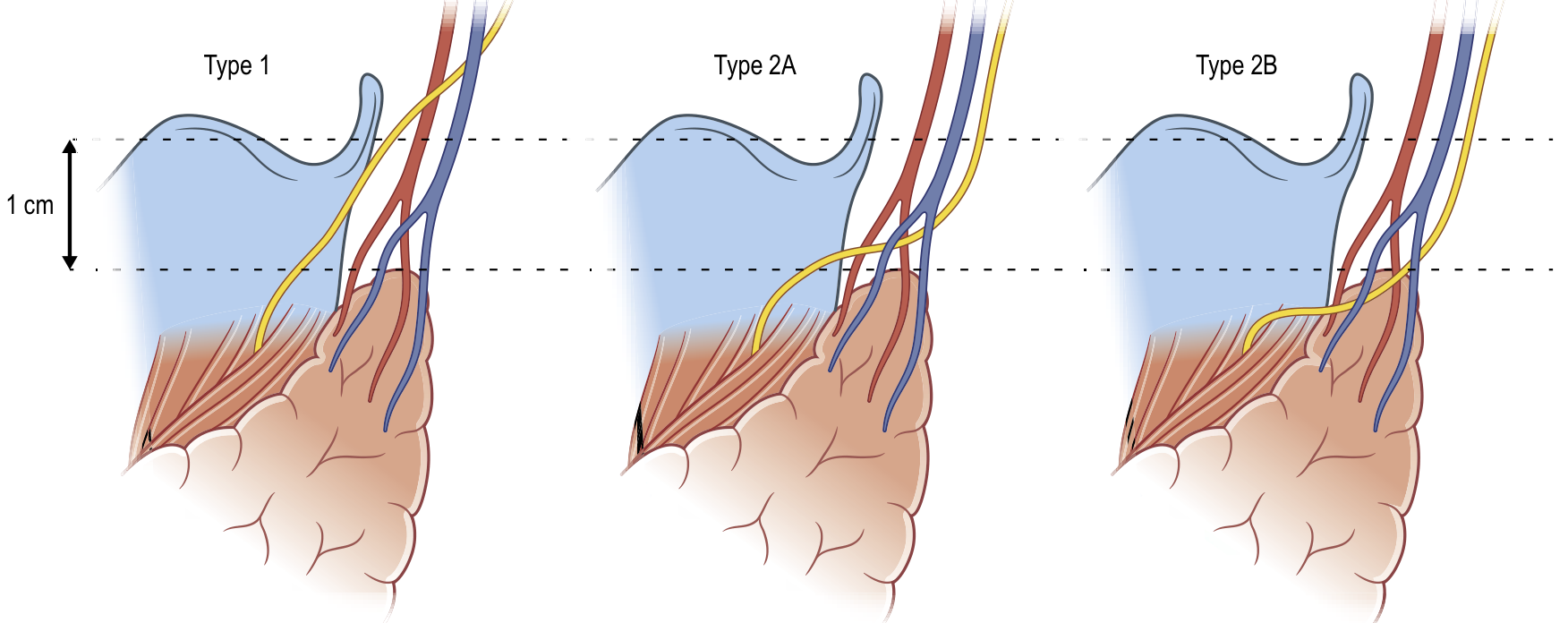
- External branch of the superior laryngeal nerve (EBSLN): innervates the cricothyroid muscle, controlling high-pitch voice projection. It travels close to the superior thyroid artery. The Cernea classification describes its relationship to the superior pole:
-
Type 1: crosses > 1 cm above the superior pole (safest)
-
Type 2A: crosses within 1 cm above the superior pole
-
Type 2B: crosses below the superior border of the superior pole (highest risk)
-
Recurrent laryngeal nerve (RLN):
- Left RLN: loops around the aortic arch, ascends in the tracheoesophageal groove
- Right RLN: loops around the subclavian artery, ascends more laterally
- A non-recurrent inferior laryngeal nerve (prevalence ~0.5%) occurs with an aberrant retro-esophageal right subclavian artery - it lies in a near-transverse trajectory and must be identified preoperatively
Parathyroid glands:
-
Two glands per side (superior and inferior), classically posterior to the thyroid
-
Superior glands are more predictable, lying within 2-5 mm of the RLN
-
Inferior glands are more variable, on average 7-10 mm from the RLN
-
Ectopic glands occur in ~15% of patients (retroesophageal, intrathyroidal, or in the thyro-thymic ligament/mediastinum)
-
Current Surgical Therapy 14e, p. 898-899
Preoperative Preparation
-
Biochemical assessment: TFTs (TSH, free T4), serum calcium (especially in MEN2A)
-
Imaging: Neck ultrasound; CT for substernal extension or airway assessment
-
FNA biopsy: for nodular or malignant disease
-
For hyperthyroidism: render the patient euthyroid preoperatively with antithyroid drugs ± beta-blockers; Lugol's iodine solution or SSKI may be added within 10 days of surgery for Graves disease to reduce gland vascularity
-
Voice and laryngeal assessment:
- All patients: noninvasive voice history and assessment
- Selective laryngoscopy for: prior voice changes, prior cervical surgery, posterior extrathyroidal extension, or bulky nodal metastases
- Preoperative vocal cord dysfunction found in up to 3.5% with benign disease and up to 8% with cancer; notably up to 20% of paralyzed cords are associated with a normal voice
- Transcutaneous laryngeal ultrasound is emerging as a noninvasive alternative (sensitivity/specificity 93-100%/97-100%)
-
Sabiston Textbook of Surgery, p. 1523-1524
Anesthesia and Positioning
-
General endotracheal anesthesia (most cases)
-
If intraoperative nerve monitoring (IONM) planned: specialized neuromonitoring ETT with vocal cord contact electrodes; muscle relaxants are contraindicated
-
Position: supine, both arms tucked, back raised ~20-30 degrees (reverse Trendelenburg), neck extended with a shoulder roll
-
Excessive extension is uncomfortable postoperatively; inadequate extension crowds the field
-
Total IV anesthesia (TIVA) may reduce coughing and improve recovery quality
-
Local anesthesia with cervical plexus blocks is described but uncommon
-
Scott-Brown's Otorhinolaryngology, p. 1060-1067; Sabiston Textbook of Surgery, p. 1524
Operative Technique
Incision and Exposure
- Transverse collar incision along Langer's lines, typically 2-3 cm above the clavicular heads
- Carried through the platysma; subplatysmal flaps raised inferiorly to the clavicles and superiorly to the thyroid cartilage
- Strap muscles (sternohyoid, sternothyroid) lifted off the thyroid capsule in the midline along avascular planes
- Middle thyroid vein exposed and ligated between thyroid and IJV
- For large/firm glands: sternothyroid muscle may be divided high (near thyroid cartilage insertion) to improve lateral exposure; preserve the ansa cervicalis
Superior Pole Dissection
- Develop the avascular cricothyroid space (space of Reeve) between the superior pole and cricothyroid muscle
- Isolate the superior thyroid artery with closed-tip blunt dissection
- Identify the EBSLN (visually or with nerve monitor) before ligation
- Divide the superior pedicle as close to the gland as possible to protect the EBSLN
Inferior Pole Dissection
- Retract inferior pole superiorly; ligate inferior thyroid vein branches close to the gland
- Avoid straying deep and lateral (risks injury to the parathyroids and RLN)
RLN Identification and Parathyroid Preservation
- The RLN is at greatest risk at: (1) the ligament of Berry, (2) during ligation of branches of the inferior thyroid artery, and (3) at the thoracic inlet
- The nerve should be identified and traced along its entire course
- IONM allows direct or vagal stimulation-based monitoring of RLN integrity
- Superior parathyroid glands: posterior to the RLN plane; inferior glands: anterior
- Any devascularized or inadvertently removed parathyroid tissue confirmed by frozen section or intraoperative PTH aspiration should be minced and autotransplanted into the sternocleidomastoid muscle
Isthmus Division
-
Dissection extended under the isthmus; divided so that the isthmus (and pyramidal lobe if present) is included with the specimen
-
Current Surgical Therapy 14e, p. 899-900; Sabiston Textbook of Surgery, p. 1525-1527
Minimally Invasive Approaches
- Transaxillary thyroidectomy: remote access; avoids a neck scar
- Transoral thyroidectomy: vestibular approach; no visible scar
- Robotic thyroidectomy: extends the reach and dexterity of minimally invasive approaches
- These offer cosmetic advantages; fundamental surgical steps remain the same
Postoperative Care
- Outpatient thyroidectomy is appropriate for selected patients who: (1) live within driving distance of the hospital, (2) have reliable adult support at home for 24 hours, (3) have no significant perioperative comorbidities or anticoagulant use
- The majority of neck hematomas occur within the first 6 hours; standard observation was historically overnight but outpatient management is now evidence-supported for low-risk cases
- Thyroid hormone replacement (levothyroxine) is required after total thyroidectomy; started postoperatively
- Calcium/calcitriol supplementation: many high-volume centers use prophylactic calcium ± calcitriol after total thyroidectomy, especially in high-risk groups (Graves disease, pediatric patients)
Complications
1. Recurrent Laryngeal Nerve Injury
- Temporary injury: 4-10% of cases
- Permanent injury: 0.5-2% (up to fourfold higher in children)
- Unilateral: hoarse/breathy voice, vocal fatigue, dysphagia, aspiration
- Bilateral: midline vocal cord positioning → airway compromise → may need tracheostomy
- Risk factors: low surgeon volume, reoperative surgery, extensive malignancy, Graves disease, large substernal goiter
2. Hypoparathyroidism
- Most common complication of thyroid surgery
- Temporary: up to 5-15% (resolves within 6 months in most)
- Permanent: 1-3%
- Manifests as symptomatic hypocalcemia (tetany, perioral tingling, Chvostek's/Trousseau's signs)
- Risk factors: bilateral neck exploration, central neck dissection, reoperative surgery, Graves disease, pediatric age
- Near-infrared parathyroid autofluorescence shows promise for intraoperative identification but current data show mixed results
3. Postoperative Neck Hematoma
- Incidence: 0.1-1.1%
- The primary danger is tracheal compression causing rapid airway compromise (not blood loss)
- Presents with: pain, incision oozing, ecchymosis, firm neck swelling, and potentially stridor
- Requires immediate return to the operating room for hematoma evacuation
- Risk factors: male sex, advanced age, bilateral operation, Graves disease, anticoagulant use
4. EBSLN Injury
-
Causes: vocal fatigue, decreased high-pitch ability, reduced voice projection
-
Rates estimated at 2.5-28% (wide range due to diagnostic difficulty; laryngoscopy often normal; confirmed by EMG)
-
Sabiston Textbook of Surgery, p. 1527-1529
Surgeon Volume and Outcomes
-
Surgeon experience is a well-established, modifiable determinant of outcomes
-
Higher-volume surgeons have fewer complications, shorter stays, and lower costs
-
A study of 16,954 patients showed outcomes improved with increasing volume up to a threshold of 26 total thyroidectomies per year on restricted cubic spline analysis
-
Sabiston Textbook of Surgery, p. 1522
Sources: Current Surgical Therapy 14e | Sabiston Textbook of Surgery (21e) | Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1
This is a shared conversation. Sign in to Orris to start your own chat.