Physiology of pain
Reading File
Finding Sources
Finding Sources
Searching the Web
physiology of pain nociception pathways 2024 overview
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed answer.
Physiology of Pain
Pain is defined by the International Association for the Study of Pain (IASP) as "an unpleasant sensory and emotional experience associated, or resembling that associated, with actual or potential tissue damage." It is both a protective physiological mechanism and a complex subjective experience shaped by biological, psychological, and sociological factors.
1. The Pain Experience - Three Components
The pain experience has three interdependent components (Firestein & Kelley's Textbook of Rheumatology):
| Component | Nature | Neural Substrate |
|---|---|---|
| Sensory/Discriminative | Intensity, location, quality | Peripheral receptors → ascending tracts → somatosensory cortex |
| Affective/Emotional | Suffering, distress | Ascending fibers → brainstem & limbic structures |
| Evaluative/Cognitive | Meaning, cultural response | Ascending fibers → forebrain (PFC, insula) |
2. Classification of Pain
Pain is mechanistically divided into four types (Firestein & Kelley's):
- Nociceptive pain - transient response to a noxious stimulus; activates high-threshold afferents; protective function.
- Inflammatory pain - spontaneous hypersensitivity following tissue damage/inflammation (e.g., postoperative pain, arthritis).
- Functional pain - hypersensitivity from abnormal central processing of normal input (e.g., fibromyalgia, irritable bowel syndrome).
- Neuropathic pain - spontaneous pain from damage to or lesions of the nervous system (e.g., postherpetic neuralgia, diabetic neuropathy).
3. Nociceptors - The Peripheral Detectors
Nociceptor receptors are found in skin, connective tissue, blood vessels, periosteum, and most visceral organs. They are free nerve endings formed by peripheral endings of primary sensory neurons (Bradley & Daroff's Neurology).
Types of Cutaneous Nociceptors
| Type | Fiber | Properties |
|---|---|---|
| High-threshold mechanical (HTM) | Aδ (myelinated) | Mechanical stimuli |
| Mechanothermal (MT) | Aδ (myelinated) | Mechanical + thermal |
| Polymodal | C (unmyelinated) | Mechanical, chemical, AND thermal |
Adequate Stimuli Vary by Tissue
- Skin: pricking, cutting, crushing, burning, freezing
- Skeletal muscle: ischemia, necrosis, hemorrhage, prolonged contraction
- Stomach/intestine: distention, smooth muscle spasm, inflamed mucosa (NOT cutting or crushing)
- Cardiac muscle: ischemia (most important)
- Joints: synovial inflammation, ligament tearing
- Blood vessels: puncture, inflammation, distention (Adams & Victor's Neurology)
4. Peripheral Transduction & Chemical Mediators
Noxious stimuli are transduced into depolarizing currents by specialized receptors in nociceptor terminals. A key transducer is TRPV1 (transient receptor potential vanilloid 1), a ligand-gated ion channel in nociceptors that:
- Is activated by temperatures >43°C (painful heat)
- Is activated by capsaicin, ethanol, and low pH (<5.9, as in inflamed tissue)
- Is sensitized by inflammatory mediators: bradykinin, PGE2, ATP, glutamate, NGF, and cytokines (Rheumatology, 2022)
With tissue damage, proteolytic enzymes release pain-producing substances including histamine, prostaglandins, serotonin, kinins, and potassium ions. These excite peripheral nociceptors and increase local vascular permeability.
Substance P is released from C fiber endings during peripheral nerve stimulation. It:
- Dilates cutaneous vessels (erythema)
- Releases histamine from mast cells (edema)
- Acts as a chemoattractant for leukocytes
This is called neurogenic inflammation, mediated by antidromic action potentials - the basis of the axon reflex of Lewis (Adams & Victor's).
5. Primary Afferent Fibers
| Fiber | Myelination | Conduction Velocity | Pain Quality |
|---|---|---|---|
| Aδ | Thinly myelinated | ~15 m/s | Sharp, well-localized, "first pain" |
| C | Unmyelinated | 0.5-2 m/s | Dull, burning, poorly localized, "second pain" |
Cell bodies of primary afferents below the head are located in the dorsal root ganglion (DRG). Visceral nociceptive afferents (Aδ, C) travel with sympathetic and parasympathetic nerves, with cell bodies also in the DRG (Bradley & Daroff's).
6. Spinal Cord Dorsal Horn Processing
Axons from DRG neurons enter the spinal cord via dorsal roots and terminate in the Rexed laminae:
- Aδ fibers (HTM, MT) → primarily laminae I and V
- C fibers → primarily lamina II (substantia gelatinosa)
Dorsal Horn Neurons
- Nociceptive-specific (NS) neurons - respond only to noxious stimuli
- Wide dynamic range (WDR) neurons - respond to both nociceptive and non-nociceptive stimuli
Key Neurotransmitters at the Dorsal Horn
- Glutamate (main neurotransmitter) - acts on AMPA receptors postsynaptically, causing rapid depolarization and action potential discharge
- Substance P - neuropeptide cotransmitter
- Activation of NMDA receptors by glutamate during intense stimulation underlies central sensitization (Firestein & Kelley's)
7. Ascending Pain Pathways
Most second-order neurons cross the midline via the anterior white commissure and ascend as the spinothalamic tract (STT) in the contralateral anterolateral quadrant. The STT is somatotopically organized (sacral elements posterolaterally, cervical elements anteromedially).
Two Major Subdivisions
Neospinothalamic tract (fast pain):
- Projects to ventral posterolateral (VPL) nucleus of the thalamus
- Third-order neurons project to primary somatosensory cortex (SI)
- Mediates: sharp, well-localized, fast pain
Paleospinothalamic tract (slow pain):
- Fibers synapse in periaqueductal gray (PAG) and brainstem reticular nuclei (spinoreticular pathway)
- Projects to central/intralaminar nuclei of the thalamus
- Mediates: slow, burning, aching, poorly localized pain and the emotional response to pain
Cortical Processing (the "Pain Matrix")
fMRI and PET studies show activation of multiple areas during painful stimulation:
- Primary and secondary somatosensory cortex (SI, SII)
- Thalamus
- Anterior cingulate cortex (ACC) - emotional component
- Insular cortex - autonomic and affective integration
- Prefrontal cortex - cognitive evaluation
- Supplemental motor cortex (Bradley & Daroff's)
8. Gate Control Theory (Melzack & Wall, 1965)
Proposed by Ronald Melzack and Patrick Wall at MIT, this theory explains how non-painful stimuli can inhibit pain.
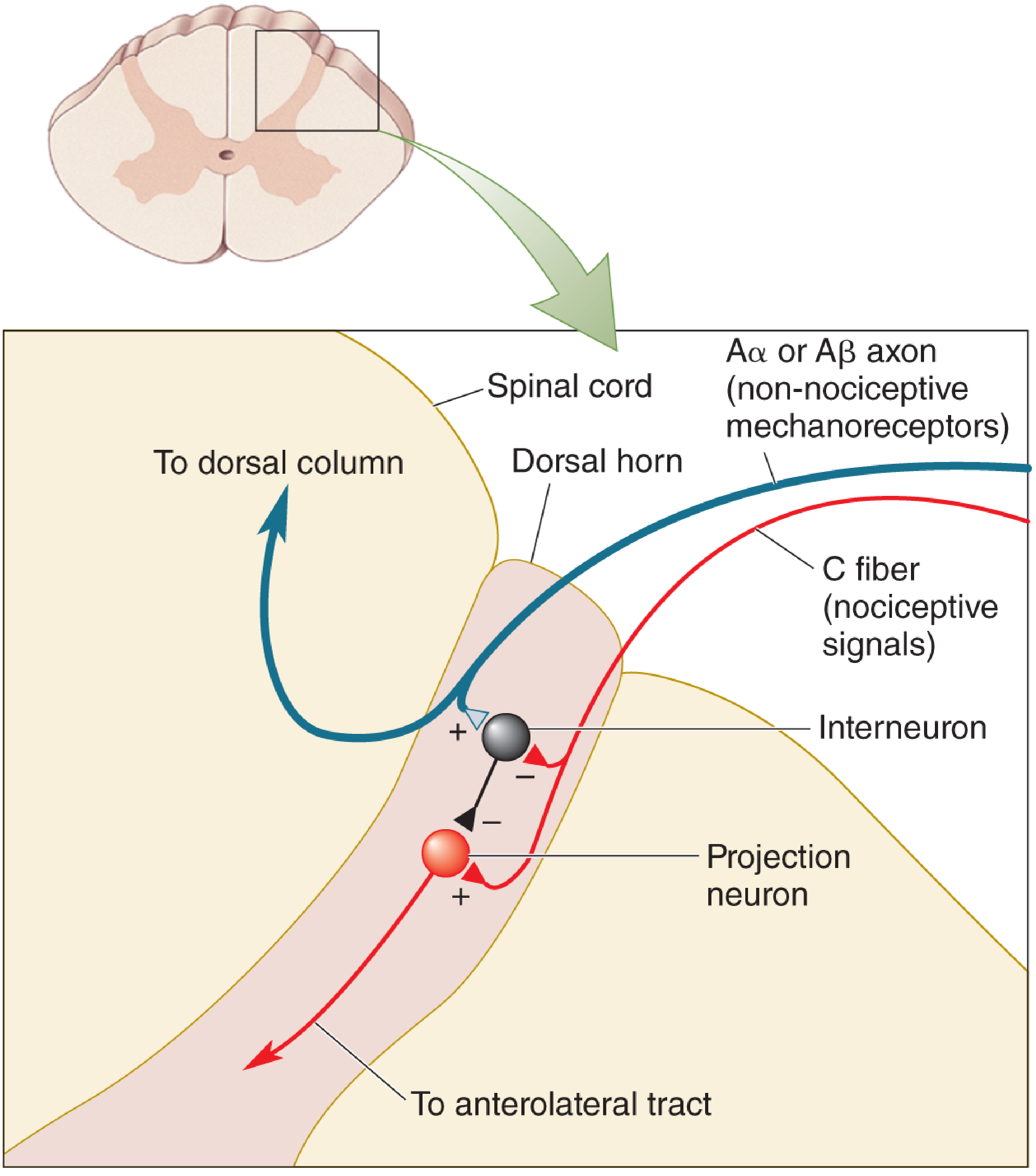
Figure: Melzack & Wall's Gate Control Theory. Non-nociceptive Aβ mechanoreceptors excite an inhibitory interneuron ("close the gate"), which inhibits the projection neuron carrying pain signals up the anterolateral tract. Nociceptive C fibers inhibit the interneuron ("open the gate"), permitting pain transmission. - Neuroscience: Exploring the Brain, 5th Ed.
Key principle: Pain signals from thin C fibers can be suppressed when large-diameter Aβ touch-sensitive axons fire at high rates, activating inhibitory interneurons. This is the mechanism behind:
- Rubbing an injured area to reduce pain
- TENS (transcutaneous electrical nerve stimulation) for chronic pain
9. Descending Pain Modulation
Several brain regions inhibit nociceptive signals at the spinal cord level. The key player is the periaqueductal gray matter (PAG) of the midbrain (Neuroscience: Exploring the Brain, 5th Ed.).
Three Descending Inhibitory Neurotransmitter Systems (Bradley & Daroff's):
- Opioid system: Endogenous opioids (β-endorphin, enkephalins, dynorphin) in the amygdala, hypothalamus, PAG, raphe magnus, and dorsal horn
- Noradrenergic system: Neurons from the locus coeruleus project via the dorsolateral funiculus; α₂-receptor agonists (e.g., clonidine) produce analgesia
- Serotonergic system: Neurons from the raphe magnus project to the dorsal horn via the dorsolateral funiculus; serotonin at the spinal cord produces analgesia
Clinical relevance: The analgesic effects of tricyclic antidepressants and SNRIs (duloxetine, milnacipran) work by increasing serotonin and norepinephrine in these descending inhibitory pathways.
Strong emotion, stress, or injury can trigger powerful pain suppression via the PAG - explaining why soldiers with severe battlefield wounds sometimes feel no pain initially.
10. Peripheral and Central Sensitization
Peripheral Sensitization
With repetitive or strong noxious stimulation or inflammation:
- The excitation threshold of polymodal nociceptors decreases - light, normally innocuous stimuli now activate them
- Silent nociceptors become excitable
- This produces enhanced afferent input to the spinal cord
Peripheral sensitization is a hallmark mechanism in rheumatoid arthritis, osteoarthritis, and myositis (Rheumatology, 2022).
Central Sensitization
Enhanced input from the periphery induces changes in dorsal horn neurons:
- Primary hyperalgesia - increased pain sensitivity at the site of injury
- Allodynia - non-painful stimuli produce pain
- Secondary hyperalgesia - enhanced pain sensitivity in healthy tissue surrounding the inflamed area
- In chronic pain, Aβ fibers (normally non-nociceptive) also participate in pain transmission
Clinical significance: Once peripheral and central sensitization become established, patients may experience pain with minor stimulation - or even spontaneous pain without any peripheral stimulus (Bradley & Daroff's).
11. Pain Perception - Threshold and Modulation
- The pain threshold (lowest intensity recognized as pain) is approximately the same in all persons under normal conditions
- Inflammation lowers the threshold through sensitization
- Raised by: local anesthetics, analgesic drugs, certain CNS lesions
- Placebos reduce pain in ~one-third of patients
- Distraction and suggestion reduce awareness of pain but not the threshold itself
- Strong emotion (fear, rage) suppresses pain via descending noradrenergic activation (Adams & Victor's)
12. Opioid Receptors
Opioids act via G-protein coupled receptors. The five classes are μ, δ, κ, σ, and ε:
- μ (mu) receptors - primary targets of morphine; found in the PAG and substantia gelatinosa
- μ₁ (supraspinal): analgesia, euphoria
- μ₂ (spinal): constipation, respiratory depression
- Presynaptically: opioid receptor activation inhibits release of substance P and glutamate
- Postsynaptically: opens K⁺ channels → hyperpolarization → neuronal inhibition (Bradley & Daroff's)
Summary Flowchart
Noxious stimulus
↓
Peripheral nociceptor activation (Aδ, C fibers)
↓
Chemical mediators released (histamine, PGs, substance P, kinins)
↓
DRG → Dorsal horn (laminae I, II, V)
↓
Dorsal horn neurons (NS and WDR) ← [Gate control modulation by Aβ fibers]
↓
Anterior commissure crossing
↓
Spinothalamic tract (neospinothalamic + paleospinothalamic)
↓
Thalamus (VPL → cortex) + PAG + Reticular formation
↓
Cortical processing (SI, SII, ACC, insula, PFC)
↓
Pain perception (sensory + emotional + cognitive)
↑
Descending modulation (PAG → raphe magnus / locus coeruleus → dorsal horn)
Sources:
- Adams & Victor's Principles of Neurology, 12th Ed., Ch. on Pain
- Bradley & Daroff's Neurology in Clinical Practice, Ch. 52 on Pain Pathways
- Firestein & Kelley's Textbook of Rheumatology, Ch. on Pain Physiology
- Rheumatology, 2-Volume Set (Elsevier, 2022), Ch. 6 on Peripheral Sensitization
- Neuroscience: Exploring the Brain, 5th Ed., Ch. 12 on Pain and Gate Control
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Ed., Pain Processing Chapter
This is a shared conversation. Sign in to Orris to start your own chat.