definition, signs & symptoms, causes, clinical assessment and management of DKA for EMT students according to the new guideline
Reading File
Finding Sources
Searching the Web
DKA diabetic ketoacidosis EMT prehospital management guidelines 2024 2025
Searching PubMed
"diabetic ketoacidosis" AND "prehospital" AND management
Reading File
Reading File
Reading Web Page
https://www.nj.gov/health/ems/documents/NEWJERSEYEMSCLINICAL…
Searching PubMed
"diabetic ketoacidosis" AND management AND guidelines
Reading File
Reading File
Reading Article
PMID: 40032308
Reading File
Loading Image
I now have everything needed for a thorough, guideline-aligned EMT-focused DKA guide. Let me compile the full response.
Diabetic Ketoacidosis (DKA) - Complete EMT Guide
Based on Rosen's Emergency Medicine, Goldman-Cecil Medicine, NJ EMS Clinical Practice Protocols (2025), and the 2024 ADA Consensus Report on Hyperglycemic Crises
1. DEFINITION
DKA is a life-threatening metabolic emergency defined by a triad of:
| Feature | Threshold |
|---|---|
| Hyperglycemia | Blood glucose > 250 mg/dL (may be lower in euglycemic DKA) |
| Ketonemia/Ketonuria | Urine ketones 2+ or serum β-hydroxybutyrate ≥ 3.0 mmol/L |
| Metabolic acidosis | Arterial/venous pH < 7.30; bicarbonate < 15 mmol/L |
It occurs when insulin deficiency and excess counter-regulatory hormones (glucagon, cortisol, catecholamines) combine to produce a hyperglycemic, dehydrated, acidotic patient with profound electrolyte imbalances. DKA is most common in Type 1 diabetes but occurs in Type 2 as well - approximately 25% of episodes happen in patients with previously undiagnosed diabetes.
ADA 2024 Update: The updated June 2024 ADA Consensus Report introduced revised diagnostic and resolution criteria for DKA and HHS, as well as new recommendations for assessment and management. [PMID 40032308]
2. PATHOPHYSIOLOGY (Why It Happens)
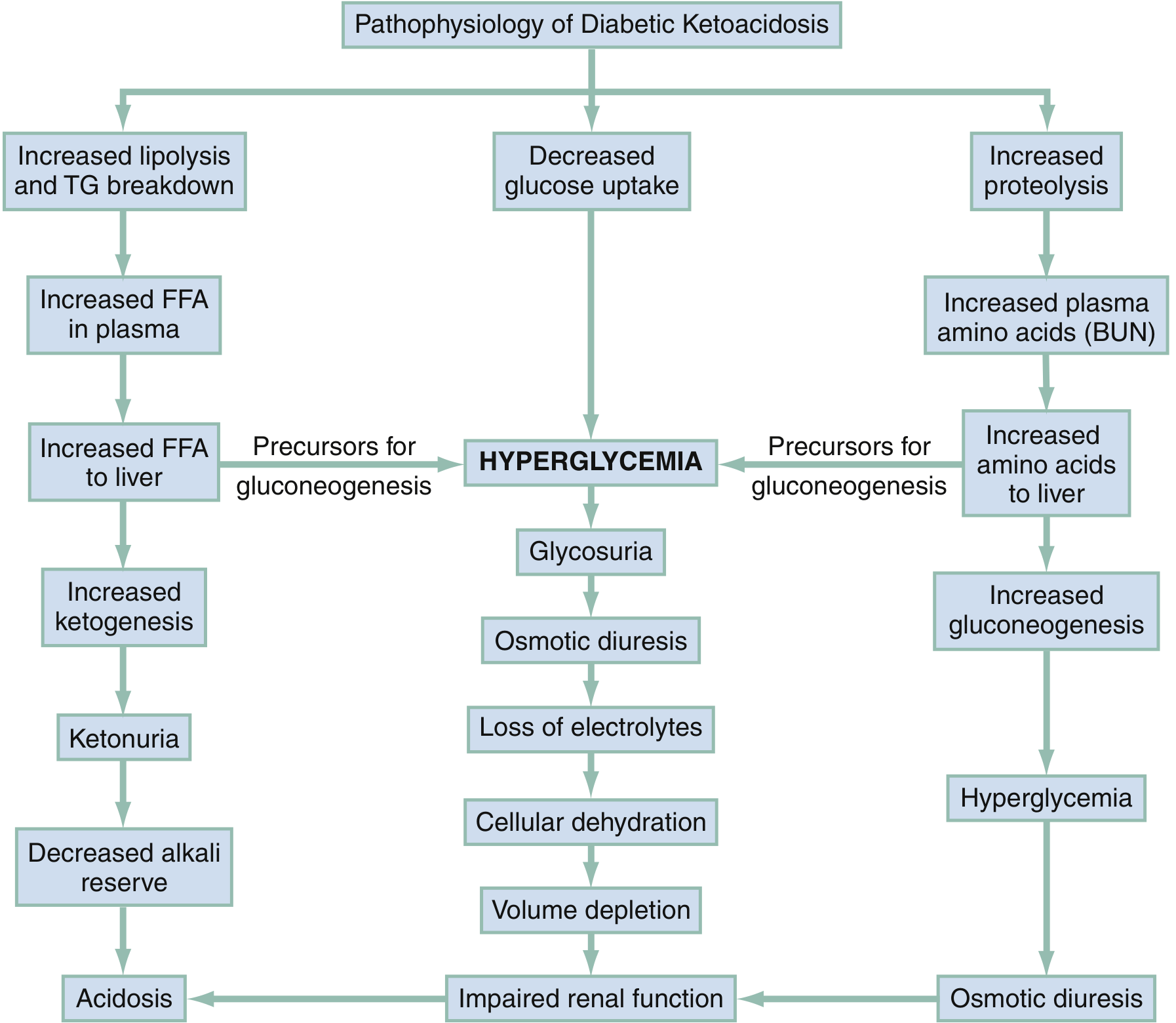
Three simultaneous processes drive DKA:
-
Lipolysis pathway: Insulin deficiency activates hormone-sensitive lipase → increased free fatty acids (FFA) → FFA enter the liver → converted to ketone bodies (β-hydroxybutyrate, acetoacetate, acetone) → ketoacidosis
-
Hyperglycemia pathway: Cells cannot uptake glucose → blood glucose rises → exceeds renal threshold → glycosuria → osmotic diuresis → loss of water, sodium, potassium, magnesium, phosphorus, chloride → profound dehydration and electrolyte depletion
-
Proteolysis pathway: Muscle breaks down amino acids → liver uses them for gluconeogenesis → worsens hyperglycemia → worsens osmotic diuresis
The acidosis triggers Kussmaul respirations (deep, rapid breathing) as the body tries to blow off CO2 to compensate. Hyperosmolarity and acidosis together directly depress mental status.
- Rosen's Emergency Medicine, 9th Ed.
3. CAUSES / PRECIPITANTS
The "6 I's" mnemonic covers most triggers:
| Category | Examples |
|---|---|
| Infection | UTI, pneumonia, sepsis (most common overall trigger) |
| Inadequate insulin | Missed doses, pump failure, non-compliance, medication cost barriers |
| Initial diagnosis | New-onset Type 1 diabetes (25% of DKA cases) |
| Ischemia/Infarction | Acute MI, stroke, PE, mesenteric ischemia |
| Intoxication | Alcohol, cocaine |
| Inflammatory/Intercurrent illness | Acute pancreatitis, burns, hyperthermia, trauma |
Drugs that can precipitate DKA:
-
Corticosteroids
-
SGLT-2 inhibitors (e.g., empagliflozin, dapagliflozin) - can cause euglycemic DKA (glucose may be < 250!)
-
Antipsychotics (clozapine, olanzapine)
-
Thiazide diuretics
-
Sympathomimetics
-
Goldman-Cecil Medicine, Table 210-11
4. SIGNS & SYMPTOMS
Onset (typically gradual over 12-24 hours)
Symptoms reported by the patient:
- Polyuria - excessive urination (from osmotic diuresis)
- Polydipsia - excessive thirst
- Polyphagia - increased hunger (early)
- Nausea and vomiting
- Abdominal pain - seen in ~50% of patients, especially children; in adults, consider this as a sign of an underlying precipitant
- Weakness and fatigue
- Visual blurring
- Weight loss
Physical examination findings (what you will observe):
| Finding | Cause |
|---|---|
| Tachypnea with Kussmaul breathing (deep, labored breathing) | Respiratory compensation for metabolic acidosis |
| Fruity/acetone odor on breath | Exhaled acetone (a ketone body) |
| Tachycardia | Dehydration, hypovolemia |
| Hypotension / orthostatic changes | Severe volume depletion (average deficit 3-5 L in adults) |
| Dry mucous membranes, poor skin turgor, sunken eyes | Dehydration |
| Altered mental status (drowsiness → stupor → coma) | Hyperosmolarity + acidosis |
| Warm, flushed skin | Peripheral vasodilation from acidosis |
| Elevated temperature | Rarely from DKA itself - suggests underlying infection |
DKA Severity Classification (ADA 2024)
| Severity | Glucose (mg/dL) | pH | Bicarbonate | Mental Status |
|---|---|---|---|---|
| Mild | > 250 | 7.25 - 7.30 | 15-18 mmol/L | Alert |
| Moderate | > 250 | 7.00 - 7.24 | 10-15 mmol/L | Alert/Drowsy |
| Severe | > 250 | < 7.00 | < 10 mmol/L | Stupor/Coma |
- Goldman-Cecil Medicine, Table 210-12
5. CLINICAL ASSESSMENT FOR EMTs
Scene Size-Up & Primary Survey
- Scene safety - ensure safe environment; note any insulin/medication bottles, glucometer
- General impression - patient may appear ill, diaphoretic, or confused
- Airway - assess; unconscious patients at risk for aspiration (especially if vomiting)
- Breathing - note rate, depth; Kussmaul breathing is a key finding
- Circulation - assess skin color/moisture/temperature; radial pulse quality; signs of shock
History (SAMPLE)
- S - Symptoms: nausea, vomiting, abdominal pain, polyuria, polydipsia, weakness
- A - Allergies to medications (especially insulin)
- M - Medications: insulin type/dose, any recent changes; SGLT-2 inhibitors; steroids
- P - Past history of diabetes (Type 1 or 2), previous DKA episodes
- L - Last oral intake; last insulin dose taken
- E - Events: recent illness, infection, stress, trauma, medication non-compliance
Physical Assessment (Focused)
Vital Signs:
- BP: look for hypotension or orthostatic drop
- HR: tachycardia is expected
- RR: Kussmaul breathing (deep and rapid)
- SpO2: usually normal unless pulmonary complication
- Temperature: fever suggests infection as precipitant
Blood Glucose (glucometer):
- The cornerstone EMT assessment tool
- DKA: typically > 250 mg/dL (but can be lower with SGLT-2 inhibitors or partial treatment)
- Document the exact reading
Mental Status (AVPU or GCS):
- Alert? Responsive to voice? Pain? Unresponsive?
- Altered mental status = higher severity, faster transport
Skin: Warm, dry, flushed; poor turgor = significant dehydration
Breath odor: Fruity/ketone smell is a strong clinical clue
6. MANAGEMENT - EMT Scope of Practice
EMT-Basic (BLS) Actions
- Ensure scene safety and BSI (Standard Precautions - wear gloves)
- Primary survey and stabilize ABCs
- Administer oxygen to maintain SpO2 ≥ 94%
- Do NOT suppress Kussmaul breathing with high-flow oxygen unless hypoxic - this breathing is compensatory
- Obtain blood glucose level via glucometer (if approved by agency Medical Director)
- If BG < 60 mg/dL with AMS → treat as hypoglycemia instead
- Position the patient: semi-Fowler's if alert; recovery position if unconscious/vomiting
- Do NOT delay transport - DKA requires hospital-level treatment (IV fluids, insulin, electrolyte monitoring)
- Call for ALS intercept if the patient has:
- Unstable vital signs
- Altered mental status
- Positive sepsis screen (lactate ≥ 2, suspected infection)
- Provide oral hydration (water only) IF: patient is alert, can swallow, and is not vomiting
- Monitor closely during transport - mental status, breathing, vitals
ALS / Paramedic Actions (scope for reference)
Fluid Resuscitation (highest priority):
- Adults: 1,000 mL isotonic crystalloid (Normal Saline or Lactated Ringer's) IV/IO bolus; reassess and repeat if indicated
- Pediatrics: 20 mL/kg NS bolus during first hour
- If in hypovolemic shock: administer as rapidly as possible until SBP > 80 mmHg
- Average fluid deficit is 3-5 liters in adults
- ⚠️ Use 10 mL/kg bolus in pediatric patients to reduce risk of cerebral edema (NJ EMS Protocol 2025)
- Recent meta-analysis (2024) supports balanced electrolyte solutions (e.g., LR) over 0.9% saline for faster DKA resolution [PMID 38925619]
Electrolyte Considerations:
- Potassium is likely total-body depleted (even if serum K appears normal/high due to acidosis)
- Do NOT give insulin until potassium ≥ 3.3 mEq/L - insulin drives K into cells and can cause life-threatening hypokalemia
- Add 20-40 mEq KCl per liter of fluid once K < 5.5 mEq/L and renal function is adequate
Insulin (hospital/ALS):
- 0.1 units/kg/hour regular insulin IV infusion
- Switch IV fluid to D5W/0.45% NS when glucose ≤ 300 mg/dL (to prevent hypoglycemia while continuing insulin)
- Reduce to 0.05 units/kg/hour when glucose ≤ 250 mg/dL AND ketones < 1.0 mmol/L
Airway:
- Avoid intubation if at all possible - patients have tremendous respiratory drive; matching minute ventilation with a ventilator is extremely difficult
- Intubate only if patient is comatose or vomiting with inability to protect airway
- If intubated: maintain hyperventilation to prevent worsening acidosis
Treat the precipitant: Search for and treat underlying infection or other cause
7. KEY EMT PEARLS & RED FLAGS
- Fruity breath + high BG + Kussmaul breathing = DKA until proven otherwise
- Do NOT give insulin in the field - dangerous without potassium monitoring
- Hyperglycemia worsens brain ischemia - be extra cautious in patients with concurrent stroke, cardiac arrest, or head trauma
- SGLT-2 inhibitor patients may have euglycemic DKA (BG < 250) - don't rule out DKA on BG alone if clinical picture fits
- Fever is NOT caused by DKA itself - always suspect infection as the trigger if temperature is elevated
- Abdominal pain in adults = consider real abdominal pathology triggering DKA (not just a DKA symptom)
- Bicarbonate is NOT routinely given - only considered if pH < 7.0 and not responding to fluids/insulin
- DKA patients on hemodialysis may not have osmotic diuresis and can present atypically
8. DIFFERENTIAL DIAGNOSIS
Other conditions that can mimic DKA or co-exist with it:
| Condition | Key Differentiator |
|---|---|
| Hyperosmolar Hyperglycemic State (HHS) | BG > 600 mg/dL, minimal/no ketosis, profound neurologic deficits |
| Alcoholic ketoacidosis | Euglycemic or hypoglycemic; recent alcohol use/cessation |
| Starvation ketosis | Mild, BG normal/low; no acidosis |
| Lactic acidosis | Shock state; elevated lactate; BG may be normal |
| Sepsis | May co-exist; fever, leukocytosis, source of infection |
| Acute abdomen | Can trigger DKA AND be an actual surgical emergency |
9. DOCUMENTATION CHECKLIST FOR EMTs
- Blood glucose reading (with time)
- Mental status on arrival and at handoff
- Respiratory rate and pattern (note Kussmaul breathing if present)
- Breath odor (fruity/acetone)
- Vital signs (BP, HR, RR, SpO2, Temp if available)
- Skin assessment (turgor, moisture, color)
- Last insulin dose and time
- Last oral intake
- Medications (especially SGLT-2 inhibitors or steroids)
- Oral fluids given en route (if applicable)
- ALS intercept requested/obtained (Y/N)
- Oxygen administered (rate/delivery device)
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 9th Ed. (Chapter 115, DKA section)
- Goldman-Cecil Medicine International Edition (Chapter 210, Table 210-11/12)
- NJ EMS Clinical Practice Protocols & Guidelines v1.0, August 2025 (Protocol 2.7A - Diabetic Emergencies: Hyperglycemia)
- 2024 ADA Consensus Report on Hyperglycemic Crises - Rodriguez Alvarez et al., Cleveland Clinic Journal of Medicine, 2025 [PMID 40032308]
- Szabó et al. (2024) - Balanced electrolyte solutions vs. 0.9% saline in DKA (Meta-Analysis) [PMID 38925619]
This is a shared conversation. Sign in to Orris to start your own chat.