Prevention of diabetes mellitus
Reading File
Finding Sources
Searching PubMed
"diabetes mellitus" AND "prevention"
Searching the Web
prevention of diabetes mellitus type 2 guidelines 2025
Finding Sources
Finding Sources
Searching PubMed
"type 2 diabetes" AND "prevention" AND "lifestyle intervention"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Prevention of Diabetes Mellitus
Prevention of diabetes mellitus is approached differently depending on the type (Type 1 vs. Type 2) and the stage of risk (primary, secondary, tertiary). The evidence base is strongest for Type 2 DM (T2DM), where lifestyle modification and selected pharmacotherapy have been proven to substantially delay or prevent progression from prediabetes to overt disease.
1. Understanding the Risk Continuum
Before prevention can be applied, high-risk individuals must be identified. Prediabetes is defined as:
| Parameter | Prediabetes Range |
|---|---|
| Fasting glucose | 100-125 mg/dL (IFG) |
| 2-hour post-glucose challenge | 140-199 mg/dL (IGT) |
| HbA1c | 5.7-6.4% |
- Between 6-10% of patients with impaired glucose tolerance (IGT) progress to clinical diabetes each year; up to 65% of those with both IFG and IGT progress annually.
- A1C of 6.0-6.5% carries a 5-year progression rate of 25-50%.
- Textbook of Family Medicine 9e, p. 965-966
2. Who to Screen (Risk Factors)
Screen for prediabetes in individuals with:
- Obesity (especially abdominal obesity) or BMI >25 kg/m²
- Family history of T2DM in first-degree relative
- Sedentary lifestyle
- History of gestational diabetes mellitus (GDM) or delivery of baby >9 lb
- History of cardiovascular disease
- Hypertension (BP ≥140/90 mmHg)
- Dyslipidemia: HDL <35 mg/dL or triglycerides >250 mg/dL
- Polycystic ovary syndrome (PCOS)
- Non-white ancestry
- Schizophrenia or bipolar disorder (due to antipsychotic use)
- Age >35 years (screen every 3 years)
- HIV medications or glucocorticoid use
- History of pancreatitis
- Harrison's Principles of Internal Medicine 22E, p. 604; Textbook of Family Medicine 9e, p. 966
3. Prevention of Type 2 Diabetes
A. Lifestyle Modification (First-Line)
Lifestyle modification is the most effective single intervention for preventing T2DM. The key landmark trials and their findings:
Diabetes Prevention Program (DPP) - USA:
- Randomized subjects with IGT to placebo, metformin, or intensive lifestyle intervention.
- Lifestyle modification reduced progression to T2DM by 58% (NNT = 7 over 3 years to prevent 1 case).
- Metformin reduced progression by 31% (NNT = 14 over 3 years).
- 10-year follow-up: lifestyle arm maintained a 34% relative risk reduction.
Finnish Diabetes Prevention Study and Da Qing Study (China) similarly demonstrated that reduced-calorie diet and physical activity prevent T2DM. Long-term follow-up of Da Qing showed that CVD events and mortality were also reduced.
- Fuster and Hurst's The Heart, 15th Edition; Symptom to Diagnosis, 4th Edition
Specific Lifestyle Goals (ADA Recommendations):
- Weight loss of 7% from baseline body weight (obese/overweight individuals) - maximal T2DM prevention occurs at 7-10% weight loss, reducing risk by ~80%
- At least 150 minutes per week of moderate aerobic exercise (e.g., brisk walking)
- Dietary changes: caloric restriction with deficit of 500-1000 kcal/day, reduced saturated fat, increased dietary fiber, limited refined carbohydrates, reduced sodium
A single session of moderate exercise expending 350 kcal can improve insulin sensitivity into the following day (Newsom et al., 2013). In the Nurses' Health Study, each additional 2 hours of TV viewing per day was independently associated with increased diabetes risk.
- Textbook of Family Medicine 9e, p. 966-967; Fuster and Hurst's The Heart, 15th Edition, p. 228
B. Pharmacotherapy
No drug is currently FDA-approved specifically for diabetes prevention. However, evidence supports the following:
| Drug | Evidence | Notes |
|---|---|---|
| Metformin | 31% RRR in DPP; IDPP-1 also confirmed benefit | ADA recommends considering in: BMI >35, age <60, history of GDM, progressive hyperglycemia despite lifestyle |
| Acarbose | Reduces IGT progression (STOP-NIDDM trial) | GI side effects limit use; ADA does not recommend routinely |
| Pioglitazone | Reduces T2DM risk in IGT | ACTnow trial; risk of weight gain, heart failure, fractures |
| Orlistat | Modest T2DM prevention (XENDOS trial) | ADA does not recommend routinely |
| Liraglutide | Reduces progression from prediabetes | ADA does not currently recommend routinely |
| Phentermine/topiramate ER | 10% weight loss reduces incident diabetes by 79% at 2 years | Under obesity indication |
ADA recommendation: Consider metformin in patients under 60 years with BMI >35 kg/m² and/or with progressive hyperglycemia, or those with history of gestational diabetes. The AACE also considers initiating metformin off-label if A1C >6.0%.
- Symptom to Diagnosis, 4th Ed., p. 9787; Textbook of Family Medicine 9e, p. 1067-1068; Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 3954
C. Surgical Prevention
Bariatric surgery in severely obese individuals reduces diabetes incidence by 76-80% - comparable to pharmacotherapy despite greater weight loss, suggesting a threshold effect. The optimal threshold for metabolic benefit is 7-10% weight loss.
- Fuster and Hurst's The Heart, 15th Edition, p. 229
D. Monitoring of Prediabetic Individuals
- Monitor annually for progression to clinical diabetes (HbA1c or fasting glucose)
- Address cardiovascular risk factors:
- Smoking cessation
- Target BP <140/90 mmHg (ADA) or <130/80 mmHg (AACE)
- Target LDL <100 mg/dL with statin therapy
- In women with prior GDM: screen every 3 years
4. Prevention of Type 1 Diabetes
Prevention of T1DM is at an earlier stage and is categorized as:
| Level | Target | Approach |
|---|---|---|
| Primary | Inhibit development of islet autoimmunity | Dietary/environmental interventions (mostly investigational) |
| Secondary | Halt autoimmune processes; delay clinical onset in multi-autoantibody-positive individuals | Teplizumab (anti-CD3 monoclonal antibody): a 14-day course delays onset by ~2 years in high-risk relatives |
| Tertiary | Slow beta-cell destruction after T1DM diagnosis; prevent complications | Intensive glycemic control, teplizumab trials |
Notably, nasal insulin has been studied for secondary prevention by exploiting mucosal tolerance. Teplizumab (Tzield) received FDA approval in 2022 as the first drug to delay T1DM onset in high-risk individuals.
- Goldman-Cecil Medicine, International Edition, p. 799; Mulholland and Greenfield's Surgery, 7th Edition
5. Prevention of Gestational Diabetes and Type 3c
- Gestational diabetes: Pre-pregnancy weight management, avoiding excessive gestational weight gain, and physical activity reduce risk. Women with prior GDM should be monitored and offered intensive lifestyle intervention postpartum.
- Pancreatogenic (Type 3c) diabetes: Avoiding alcohol excess and managing chronic pancreatitis reduces risk.
6. Public Health and National Programs
India's National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) focuses on:
- Health promotion and lifestyle change through mass media
- Opportunistic screening of persons above age 30
- Integration with primary health care systems
- Capacity building at all levels
- Park's Textbook of Preventive and Social Medicine, p. 3926-3945
Summary of Prevention Strategies
PREDIABETES IDENTIFIED
│
├── Lifestyle modification (FIRST LINE)
│ ├── 7-10% weight loss
│ ├── ≥150 min/wk moderate exercise
│ └── Dietary modification
│
├── Pharmacotherapy (if lifestyle insufficient)
│ ├── Metformin (ADA-endorsed)
│ └── Others (pioglitazone, acarbose - not routinely recommended)
│
├── CV risk factor management
│ ├── BP, LDL, smoking
│
└── Annual monitoring
Recent Evidence (2025)
A 2025 meta-analysis in J Med Internet Res (PMID 39879607) confirmed that lifestyle interventions via multiple delivery modes are effective in both preventing T2DM and reverting prediabetes to normoglycemia. A 2025 RCT in Nature Medicine (PMID 41023486) demonstrated that prediabetes remission and T2DM prevention can be achieved even without significant weight loss, suggesting metabolic mechanisms beyond weight reduction. The ADA Standards of Care 2025 continue to emphasize obesity management and expanded use of GLP-1 receptor agonists in those with obesity-related diabetes risk.
Vision 2020 right to sight
Reading File
Finding Sources
Finding Sources
Searching the Web
Vision 2020 Right to Sight WHO IAPB global initiative objectives strategies
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC1706008
Reading File
Finding Sources
Searching the Web
Vision 2020 India NPCB national programme control blindness implementation results
Reading File
Loading Image
I now have comprehensive information from Park's Textbook and multiple authoritative sources. Here is the complete answer:
VISION 2020: The Right to Sight
1. Background and Launch
Vision 2020: The Right to Sight is a global initiative to eliminate avoidable (preventable and treatable) blindness. It was officially launched on 18 February 1999 by the World Health Organization (WHO), with the endorsement of Dr. Gro Harlem Brundtland (Director-General, WHO), in partnership with the International Agency for the Prevention of Blindness (IAPB).
One significant feature that distinguishes this initiative from earlier ones is that it centers around rights - recognition of sight as a fundamental human right, which serves as an important catalyst for action by member countries.
- Park's Textbook of Preventive and Social Medicine, p. 2574
2. Mission and Goal
"To eliminate the main causes of blindness in order to give all the people of the world, particularly the millions of needlessly blind, the Right to Sight by the year 2020."
The initiative also aimed to prevent the projected doubling of avoidable visual impairment between 1990 and 2020. The ultimate goal was to integrate a sustainable, comprehensive, high-quality, equitable eye-care system into national health-care systems.
3. Objectives of Vision 2020
- Raise the profile among key audiences of the causes of avoidable blindness and the solutions to the problem
- Advocate for and secure the necessary resources to increase prevention and treatment activities
- Facilitate the planning, development and implementation of national Vision 2020 programmes in all countries
- Assist member countries in developing sustainable systems to eliminate avoidable blindness from major causes by the year 2020
4. Priority Disease Areas (Target Diseases)
| Disease | Key Intervention |
|---|---|
| Cataract | Surgical removal (IOL implantation); most common cause of avoidable blindness globally (43% in LMICs) |
| Trachoma | SAFE strategy (Surgery, Antibiotics, Facial cleanliness, Environmental improvement) |
| Onchocerciasis (River Blindness) | Ivermectin distribution (community-directed treatment) |
| Childhood blindness | Vitamin A supplementation, treatment of xerophthalmia, rubella vaccination, ROP screening |
| Refractive errors and Low vision | Refraction services, provision of spectacles, low vision devices |
| Corneal blindness | Keratoplasty, trachoma control |
| Glaucoma | Early detection and treatment |
| Diabetic retinopathy | Screening, laser therapy |
- Park's Textbook of Preventive and Social Medicine, p. 2583-2586; p. 6109
5. Three Core Strategies (Pillars)
National programmes under Vision 2020 rest on three main elements:
A. Disease Control
- Cost-effective interventions targeted at the priority diseases listed above
- Emphasis on community-level disease control for trachoma and onchocerciasis
- Technical working groups established for each disease priority
B. Human Resource Development
- Training of ophthalmologists, ophthalmic medical assistants, ophthalmic nurses, and medical students
- Primary health care approach to extend coverage
- Faculty development at medical colleges
C. Infrastructure and Appropriate Technology Development
- Provision of adequate eye beds and surgical facilities
- Local production of eye medicines
- Refraction capability with spectacles and low vision devices
- Required surgical instrumentation (including low-cost IOLs)
- Sustainability built into technology use
6. Guiding Principles - ISEE
The guiding principles of Vision 2020 were summarized in the acronym ISEE:
- I - Integration of eye care into health systems
- S - Sustainability
- E - Equity (community participation, equity of treatment and standard quality services)
- E - Evidence-based practice
7. India's Plan of Action under Vision 2020
National Programme for Control of Blindness (NPCB)
India was the first country to launch a government-funded national blindness control programme (1976). Prevalence of blindness has been reduced from 1.4% (1976) → 1.1% (2001) → 0.36% (2015-19 survey) - a reduction of nearly 47%.
India's four-tier structure (proposed under Vision 2020):
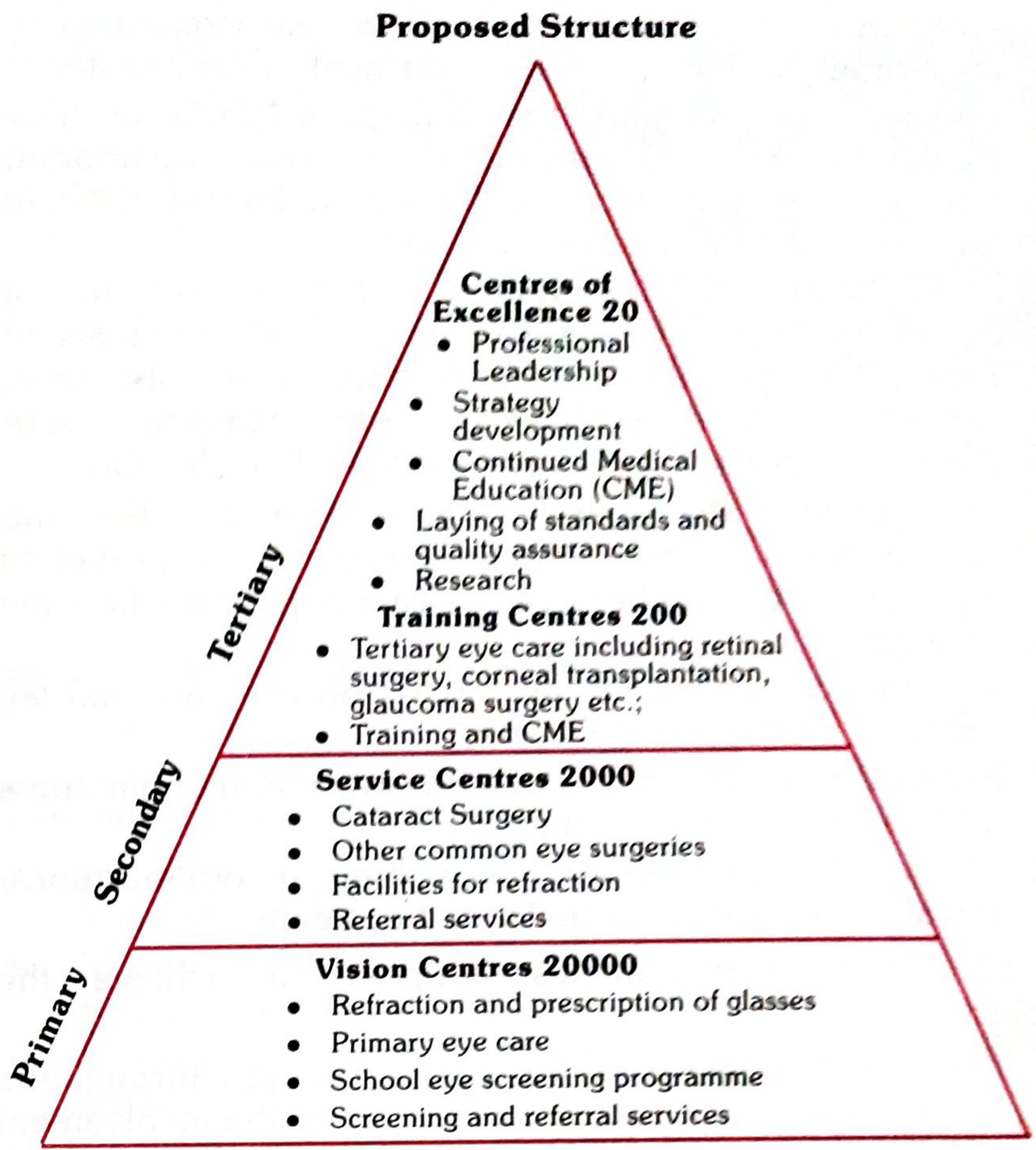
| Level | Number | Functions |
|---|---|---|
| Vision Centres (Primary) | 20,000 | Refraction and prescription of glasses, primary eye care, school eye screening, screening and referral |
| Service Centres (Secondary) | 2,000 | Cataract surgery, other common eye surgeries, refraction facilities, referral services |
| Training Centres (Tertiary) | 200 | Tertiary care (retinal surgery, corneal transplantation, glaucoma surgery), training and CME |
| Centres of Excellence (Tertiary) | 20 | Professional leadership, strategy development, CME, quality assurance, research |
- Park's Textbook of Preventive and Social Medicine, p. 6111-6113
India's target diseases under Vision 2020: Cataract, refractive errors, childhood blindness, corneal blindness, glaucoma, and diabetic retinopathy.
Key signature activities of NPCB (12th Five Year Plan):
- 66 lakh cataract operations per year
- School eye screening + 9 lakh free spectacles per year for children with refractive errors
- Collection of 50,000 donated eyes per year for keratoplasty
8. Global Eye Health Action Plan 2014-2019
Following Vision 2020, the WHO adopted the Universal Eye Health: A Global Action Plan 2014-2019, which:
- Aimed to reduce avoidable visual impairment by 25% by 2019 from the 2010 baseline
- Was built on five principles: universal access and equity, human rights, evidence-based practice, life-course approach, and empowerment of the visually impaired
- Used the health systems approach - integrating eye care at primary, secondary, and tertiary levels
- Tracked progress using 3 national-level indicators:
- Prevalence and causes of visual impairment
- Number of eye care personnel
- Cataract surgical rate
- Park's Textbook of Preventive and Social Medicine, p. 2596-2609
9. After 2020 - "2030 in Sight"
Following Vision 2020, the IAPB launched "2030 in Sight: Ending Avoidable Sight Loss", building on the success of Vision 2020 by:
- Setting the target that by 2030, no one should experience unnecessary sight loss
- Eye care and rehabilitation services should be accessible, inclusive, and affordable to everyone
- Emphasizing that national governments must own the process, with eye health as an integral part of universal health coverage
Summary Table
| Feature | Details |
|---|---|
| Launch date | 18 February 1999 |
| Launched by | WHO + IAPB |
| Goal | Eliminate avoidable blindness by 2020 |
| Key concept | Sight as a fundamental human right |
| 3 core strategies | Disease control, Human resource development, Infrastructure & technology |
| Priority diseases | Cataract, Trachoma, Onchocerciasis, Childhood blindness, Refractive errors, Low vision |
| India's prevalence target | Reduce blindness from 1.4% to 0.3% |
| India's four-tier structure | Vision Centres (20,000) → Service Centres (2,000) → Training Centres (200) → Centres of Excellence (20) |
| Successor | Universal Eye Health Global Action Plan 2014-2019; "2030 in Sight" |
This is a shared conversation. Sign in to Orris to start your own chat.