Osteoporosis therapeutic notes
Reading File
Finding Sources
Finding Sources
Searching PubMed
"osteoporosis"[MeSH Terms] AND "drug therapy"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive content from all major textbooks. Let me compile the complete therapeutic notes.
Osteoporosis - Therapeutic Notes
Treatment Thresholds & Indications
Pharmacologic therapy is warranted in:
- Postmenopausal women and men ≥50 years with a prior osteoporotic fracture
- BMD T-score ≤ -2.5 (diagnostic threshold for osteoporosis)
- Osteopenia + high fracture probability: >20% 10-year major fracture risk or >3% 10-year hip fracture risk (FRAX, US thresholds)
- Minimal-trauma fracture with BMD in osteopenia range, or multiple risk factors even if BMD is not in osteoporotic range
(Harrison's Principles of Internal Medicine 22E, p. 3345)
Drug Classification Overview
All pharmacologic agents are either antiresorptive or anabolic:
| Category | Drugs |
|---|---|
| Antiresorptive | Bisphosphonates, Denosumab, Estrogen/HRT, SERMs (Raloxifene), Calcitonin |
| Anabolic | Teriparatide, Abaloparatide, Romosozumab |
Because bone remodeling is a coupled process, antiresorptive drugs ultimately also reduce bone formation - they do not promote substantial BMD gains. BMD increases seen in the first years of antiresorptive therapy represent a contraction of the remodeling space to a new steady-state plateau. (Goodman & Gilman's, p. 575)
Relative Efficacy on Lumbar Spine BMD
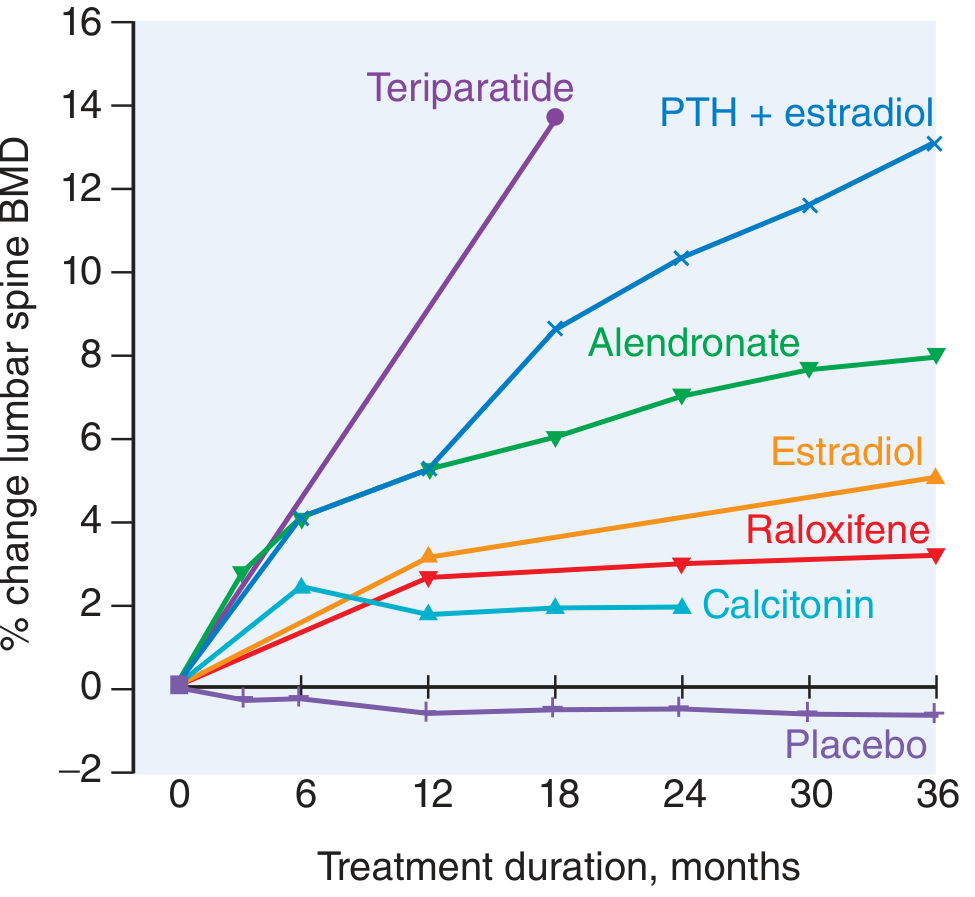
Figure: % change in lumbar spine BMD over 36 months for major osteoporosis therapies vs. placebo. Teriparatide dramatically outperforms all antiresorptive agents. - Goodman & Gilman's
1. Bisphosphonates (First-Line)
Agents: Alendronate, Risedronate, Zoledronic acid (preferred); also Ibandronate, Pamidronate, Etidronate
Mechanism of Action
- Bind to hydroxyapatite crystals in bone at sites of active remodeling
- Inhibit osteoclast function and reduce osteoclast number by inducing apoptosis
- Nitrogen-containing bisphosphonates additionally inhibit farnesyl pyrophosphate synthase (mevalonic acid pathway), disrupting intracellular protein trafficking
- Zoledronic acid has very high affinity for mineralized bone; a single IV infusion suppresses resorption for up to 1 year
(Lippincott Illustrated Reviews Pharmacology, p. 891; Harrison's 22E, p. 3348)
Relative Antiresorptive Potency
| Bisphosphonate | Relative Antiresorptive Activity |
|---|---|
| Etidronate | 1 |
| Tiludronate | 10 |
| Pamidronate | 100 |
| Alendronate | 1,000 |
| Risedronate | 5,000 |
| Ibandronate | 10,000 |
| Zoledronic acid | 10,000 |
(Lippincott Illustrated Reviews Pharmacology, p. 893)
Effect on Lumbar Spine BMD (Alendronate)
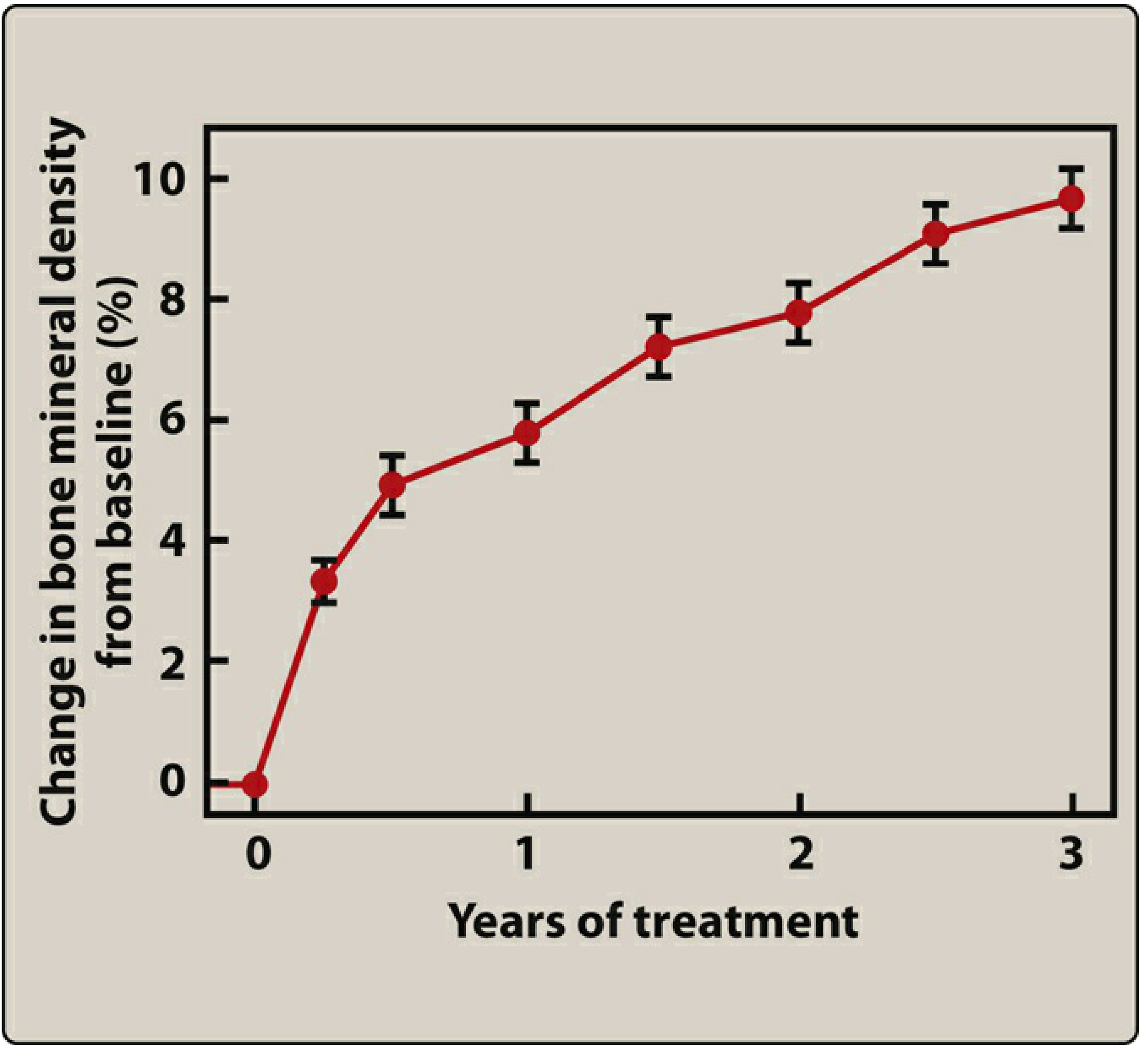
Figure: Effect of alendronate therapy on lumbar spine bone mineral density over 3 years. - Lippincott
Dosing & Administration
| Drug | Formulation | Dosing Frequency |
|---|---|---|
| Alendronate | Oral tablet / Effervescent tablet | Daily or weekly / Weekly |
| Ibandronate | Oral tablet / IV | Monthly / Every 3 months |
| Risedronate | Oral tablet / Delayed-release tablet | Daily, weekly, or monthly / Weekly |
| Zoledronic acid | IV infusion | Yearly |
Critical administration instructions for oral bisphosphonates:
- Take with 6-8 oz of plain water only (risedronate delayed-release: at least 4 oz)
- Take ≥30 min before any food, drink, or medications (≥60 min for ibandronate)
- Remain upright and do not lie down for ≥30 min after (≥60 min for ibandronate)
- Risedronate delayed-release: take immediately after breakfast
(Lippincott, p. 894)
Adverse Effects
- GI: Diarrhea, abdominal pain; esophagitis and esophageal ulcers (oral agents) - minimized by upright posture
- Musculoskeletal pain
- Osteonecrosis of the jaw (ONJ): Risk factors include longer/higher-dose therapy, IV route, dental procedures, glucocorticoids, diabetes, smoking
- Atypical femur fractures: Risk increases with long-term use
- Drug holiday: Recommended after 5 years of oral bisphosphonate or 3 years of zoledronic acid in patients whose fracture risk has decreased; do NOT discontinue in high-risk patients
- Avoid in severe renal impairment (eliminated renally)
Fracture Efficacy
- Alendronate: reduces hip and vertebral fractures; the beneficial effect persists for several years
- Bisphosphonates are preferred first-line agents for postmenopausal, male, and glucocorticoid-induced osteoporosis
2. Denosumab (RANKL Inhibitor)
Mechanism of Action
Denosumab is a fully human monoclonal antibody that binds with high affinity to RANKL (receptor activator of NF-kB ligand), mimicking the physiologic action of osteoprotegerin (OPG). By blocking RANKL from binding to RANK on osteoclast precursors and mature osteoclasts, it:
- Inhibits osteoclast formation, activity, and survival
- Produces a potent and rapid antiresorptive effect
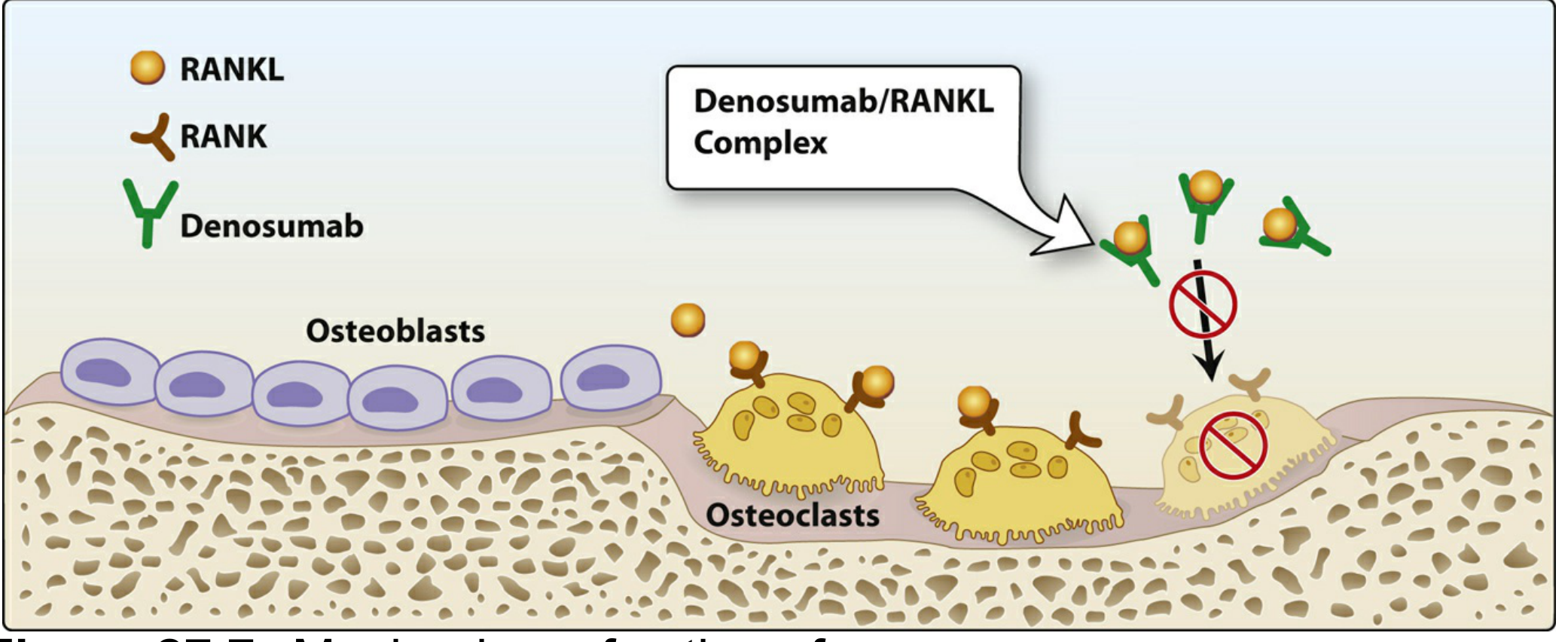
Figure: Mechanism of action of denosumab. - Lippincott
Key Pharmacology
- Route/Frequency: Subcutaneous injection every 6 months
- Unlike bisphosphonates (where BMD plateaus at 4-5 years), BMD continues to increase as long as denosumab is continued
- 10-year extension data: +21.7% spine BMD, +9.2% hip BMD
- Fracture reduction (FREEDOM trial, 3 years): Vertebral fractures -68%, Hip fractures -40%, Nonvertebral fractures -20%
Indications
- Postmenopausal osteoporosis at high fracture risk
- Male osteoporosis
- Glucocorticoid-induced osteoporosis
- Women on aromatase inhibitors (breast cancer)
- Men on androgen deprivation therapy (prostate cancer)
- Considered an alternative first-line agent, particularly for higher-risk patients
Adverse Effects
- Hypocalcemia (especially in CKD with eGFR <30 mL/min / hemodialysis - monitor serum Ca²⁺)
- Hypersensitivity reactions, dermatitis, rash, eczema
- Increased risk of infections
- ONJ (~5/10,000 patient-years), atypical femur fractures (~1/10,000 patient-years)
Critical Warning: Rebound Effect on Discontinuation
When denosumab is stopped, there is a rebound increase in bone turnover with rapid bone loss and a marked increase in multiple vertebral fracture risk. This reflects maturation of accumulated osteoclast precursors. Transition to a bisphosphonate is mandatory when discontinuing:
- Single IV infusion of zoledronic acid at time of missed dose maintains BMD for 1-2 years
- Oral bisphosphonates for 12-24 months are an alternative
- Monitor bone turnover markers and BMD after transition
(Harrison's 22E, p. 3349-3350)
3. Estrogen / Hormone Replacement Therapy (HRT)
Efficacy
- Prevents bone loss and induces small increases in BMD at spine, hip, and total body
- Epidemiologic data: ~50% reduction in osteoporosis-related fractures (including hip) in women who start early and continue treatment
- Benefit declines after discontinuation; no residual fracture protection by 10 years post-cessation
- Effective via oral, transdermal, or subcutaneous implant routes
Standard Doses
- Conjugated equine estrogens: 0.625 mg/day (lower doses of 0.3-0.45 mg also effective)
- Esterified estrogens: 0.3 mg/day
- Ethinyl estradiol: 5 μg/day
- Transdermal estradiol: 50 μg/day patch
Mode of Action
- Two estrogen receptor subtypes (ERα, ERβ) are expressed on osteoblasts and cells of monocyte lineage
- ERα is the dominant subtype in bone (ERα knockout → reduced bone mass)
- Estrogen mainly acts indirectly by reducing pro-osteoclastic cytokines (IL-1, IL-6, TNF) from osteoblasts and T-cells, rather than by direct inhibition of osteoclasts
WHI Findings - Risk-Benefit Profile
The Women's Health Initiative (>16,000 postmenopausal women) showed for combined estrogen + progestin (CEE + MPA):
| Effect | Relative Risk Change |
|---|---|
| Coronary heart disease | +29% (8 excess/10,000 women-years) |
| Stroke | +40% |
| Venous thromboembolism | +100% (18 excess/10,000 women-years) |
| Breast cancer | +26% (8 excess/10,000 women-years) |
| Hip fractures | -34% (5 fewer/10,000 women-years) |
| All clinical fractures | -24% (44 fewer/10,000 women-years) |
| Colorectal cancer | -37% (6 fewer/10,000 women-years) |
- Estrogen-only arm (women post-hysterectomy): no increased MI risk, and decreased breast cancer risk - suggesting some detrimental effects are progestin-related
- Benefit/risk ratio improved if commenced before age 60 or within 10 years of menopause
- Current guidelines: not recommended for osteoporosis prevention as primary strategy (USPSTF)
(Harrison's 22E, p. 3346-3347)
4. SERMs - Selective Estrogen Receptor Modulators
Key agent: Raloxifene
- Acts as an estrogen agonist in bone (antiresorptive) and a partial antagonist in breast and uterus
- Increases BMD by ~2-3% at lumbar spine (less than estrogen or bisphosphonates - see efficacy graph above)
- Fracture reduction: Reduces vertebral fracture risk; no proven effect on non-vertebral or hip fractures
- Additional benefit: reduces invasive breast cancer risk by ~76% in high-risk postmenopausal women
- Adverse effects: Hot flashes, leg cramps, increased venous thromboembolism risk (similar to estrogen)
- Does not cause endometrial hyperplasia
(Goodman & Gilman's; Lippincott)
5. Calcitonin
- Polypeptide hormone produced in the thyroid; suppresses osteoclast activity by direct action on the osteoclast calcitonin receptor (osteoclasts cannot maintain their active ruffled border)
- Preparations: nasal spray (200 IU/day) or injectable
- Small increments in spinal BMD; small reduction in new vertebral fractures
- No proven effect on non-vertebral or hip fractures
- Not indicated for prevention; not potent enough to prevent bone loss in early postmenopausal women
- Possible analgesic effect on bone pain
- Safety concerns: possible increased cancer risk (European Medicines Agency removed osteoporosis indication; FDA Advisory Committee voted similarly)
- Injectable form: frequent reactions including nausea and facial flushing
(Harrison's 22E, p. 3348)
6. Anabolic Agents
A. Teriparatide [PTH(1-34)]
- Recombinant human PTH fragment (hPTH 1-34)
- Acts as a PTH receptor agonist: once-daily SC administration leads to stimulation of osteoblastic activity and net bone formation (intermittent PTH is anabolic; continuous PTH is catabolic)
- Most potent BMD gain of all agents (see efficacy graph - ~14% spine BMD increase at 18 months)
- Indications: High fracture risk, failure or intolerance of antiresorptive therapy
- Dose: 20 μg SC daily (approved); max 2 years cumulative lifetime use
- Adverse effects: Injection site reactions, hypercalcemia, orthostatic hypotension
- Contraindication: Patients at risk for osteosarcoma (Paget disease, prior radiation to bone, unexplained elevated ALP, open epiphyses); increased osteosarcoma risk in rats
- After completion: Must transition to an antiresorptive agent to maintain gains
B. Abaloparatide [PTHrP(1-34)]
- Analog of parathyroid hormone-related peptide (hPTHrP 1-34)
- Similar mechanism and indications to teriparatide
- Additional adverse effect: Hyperuricemia (vs. teriparatide)
- Same 2-year lifetime limit and same post-treatment antiresorptive transition requirement
(Lippincott, p. 896)
C. Romosozumab (Sclerostin Inhibitor)
- Monoclonal antibody against sclerostin (a Wnt pathway inhibitor secreted by osteocytes that normally inhibits bone formation)
- Blocking sclerostin → promotes osteoblast activity (anabolic) + decreases bone resorption (antiresorptive) = dual mechanism (unique among osteoporosis drugs)
- Indication: Postmenopausal women with osteoporosis at high fracture risk
- Administration: Monthly SC injection for 12 months (then transition to antiresorptive)
- Key safety concern: Increased risk of cardiovascular events (MI, stroke) - contraindicated in patients with prior MI or stroke within the last year
- Must follow with antiresorptive therapy after 12-month course
(Lippincott, p. 896)
Sequential Therapy Strategy
| Clinical Scenario | Preferred Approach |
|---|---|
| Most postmenopausal women | Bisphosphonate first-line |
| High fracture risk / very low BMD | Start with anabolic (teriparatide/romosozumab), then antiresorptive |
| Patients on denosumab stopping therapy | Transition to bisphosphonate (prevent rebound) |
| After teriparatide/abaloparatide course | Transition to antiresorptive (bisphosphonate or denosumab) |
| After romosozumab (12 months) | Transition to antiresorptive |
| Glucocorticoid-induced osteoporosis | Bisphosphonate (alendronate, risedronate, zoledronic acid) |
| CKD / renal impairment | Avoid bisphosphonates (severe); denosumab with Ca²⁺ monitoring |
A 2026 systematic review (Nayak & Greenspan, Osteoporos Int) confirms that sequential treatment strategies - particularly anabolic first followed by antiresorptive - produce the greatest long-term fracture risk reduction and sustained BMD gains. A 2024 meta-analysis (Yang et al., Front Endocrinol) found denosumab superior to oral bisphosphonates for BMD increase at lumbar spine and femoral neck in postmenopausal osteoporosis.
Non-Pharmacologic Foundations
These underpin all pharmacologic therapy:
- Calcium: Dietary increase or supplementation (adequate intake essential for all drug therapies)
- Vitamin D: Supplementation; a 2025 meta-analysis (Cong & Zhang, BMC Musculoskel Disord) confirms combined Ca²⁺ + Vit D significantly improves BMD and reduces fracture risk in postmenopausal women
- Exercise: Muscle-strengthening and weight-bearing
- Lifestyle: Avoid smoking; limit alcohol
Drug Comparison Summary
| Drug | Class | Route | Frequency | Key Fracture Data | Key Risk |
|---|---|---|---|---|---|
| Alendronate | Bisphosphonate | Oral | Weekly | Vertebral + hip + non-vertebral | Esophagitis, ONJ, atypical fracture |
| Risedronate | Bisphosphonate | Oral | Weekly/monthly | Vertebral + hip + non-vertebral | Esophagitis |
| Zoledronic acid | Bisphosphonate | IV | Yearly | Vertebral + hip + non-vertebral | Renal toxicity, flu-like reaction |
| Ibandronate | Bisphosphonate | Oral/IV | Monthly/3-monthly | Vertebral only | Esophagitis |
| Denosumab | RANKL mAb | SC | Every 6 months | Vertebral -68%, Hip -40% | Rebound on cessation, hypocalcemia |
| Teriparatide | PTH analogue | SC | Daily | Vertebral + non-vertebral | Osteosarcoma risk; 2-year limit |
| Abaloparatide | PTHrP analogue | SC | Daily | Vertebral + non-vertebral | Hyperuricemia; 2-year limit |
| Romosozumab | Sclerostin mAb | SC | Monthly x12 | Vertebral + hip | Cardiovascular events |
| Raloxifene | SERM | Oral | Daily | Vertebral only | VTE, hot flashes |
| Calcitonin | Hormone | Nasal/SC | Daily | Vertebral only (modest) | Possible cancer risk |
| Estrogen/HRT | Hormone | Oral/transdermal | Daily | All fractures | VTE, stroke, breast cancer |
Sources: Harrison's Principles of Internal Medicine 22E (2025), Lippincott Illustrated Reviews Pharmacology, Goodman & Gilman's The Pharmacological Basis of Therapeutics | Recent evidence: PMIDs 41105226, 39286276, 41063100
This is a shared conversation. Sign in to Orris to start your own chat.