All about malaria
Reading File
Finding Sources
Searching PubMed
"malaria"[MeSH Terms] AND treatment
Searching the Web
malaria 2025 2026 WHO guidelines treatment prevention
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, well-sourced content. Let me compile the complete answer.
Malaria - A Complete Overview
1. Epidemiology
Malaria remains one of the most serious infectious diseases globally. The WHO estimates over 200 million cases per year, resulting in more than 600,000 deaths annually. Approximately 90% of infections occur in sub-Saharan Africa, followed by South/Southeast Asia (6%) and the Eastern Mediterranean (2%). The majority of deaths affect children infected with P. falciparum. Cases are now seen worldwide due to international travel, even in non-endemic regions.
- Robbins & Kumar Basic Pathology, p. 392
- Murray & Nadel's Textbook of Respiratory Medicine
2. Causative Organisms
Five Plasmodium species infect humans:
| Species | Disease | Fever Periodicity | Notes |
|---|---|---|---|
| P. falciparum | Falciparum (tertian) malaria | Every 48 hours | Most dangerous; can be fatal |
| P. vivax | Benign tertian malaria | Every 48 hours | Has dormant hypnozoites |
| P. ovale | Ovale tertian malaria | Every 48 hours | Has dormant hypnozoites |
| P. malariae | Quartan malaria | Every 72 hours | Can persist >10 years |
| P. knowlesi | Zoonotic malaria (SE Asia) | Every 24 hours | Morphologically mimics P. malariae, but virulent |
The female Anopheles mosquito is the vector. Humans are the only natural reservoir. P. knowlesi is a simian malaria with zoonotic transmission in Southeast Asia, often mistaken for P. malariae but capable of causing severe fatal disease.
3. Life Cycle and Pathogenesis

Fig: Life cycle of Plasmodium falciparum showing hepatic and erythrocytic stages (Robbins & Kumar Basic Pathology)
Hepatic (Pre-erythrocytic) Phase - Clinically Silent
- Sporozoites are injected into the bloodstream during a mosquito bite
- They travel to the liver, where thrombospondin-related adhesive protein and circumsporozoite protein bind to heparan sulfate proteoglycans on hepatocytes
- Sporozoites enter hepatocytes and differentiate into merozoites (incubation: 1-4 weeks)
- Infected hepatocytes rupture, releasing thousands of merozoites into the bloodstream
In P. vivax and P. ovale, a subset of parasites remain dormant in the liver as hypnozoites, which can reactivate years later causing relapse.
Erythrocytic Phase - Clinically Apparent
- A lectin-like molecule on the merozoite surface binds to sialidated glycophorin on red blood cells
- The merozoite invaginates into the RBC inside a "digestive vacuole"
- Intraerythrocytic organisms differentiate into trophozoites:
- Some become gametocytes (restart the cycle in the mosquito)
- Most become schizonts, which express PfEMP1 (P. falciparum erythrocyte membrane protein 1) - knob-like protrusions on the RBC surface
- PfEMP1 binds endothelial adhesion molecules (ICAM-1, VCAM-1, CD36), causing sequestration of parasitized RBCs in capillary beds - the key pathogenic mechanism of severe malaria
- Schizonts mature into merozoites, lyse the RBC, and the cycle repeats
4. Clinical Features
Uncomplicated Malaria
- Classic triad: Paroxysmal fever, rigors (shaking chills), and sweating
- Fever coincides with RBC lysis and merozoite release
- Associated symptoms: headache, nausea, myalgia, fatigue, mild anemia
- Periodic fever pattern (less reliable in P. falciparum):
- P. knowlesi: every 24 hours
- P. vivax, P. ovale, P. falciparum: every 48 hours
- P. malariae: every 72 hours
Severe/Complicated Malaria (predominantly P. falciparum)
| Complication | Details |
|---|---|
| Cerebral malaria | Small cerebral vessels become engorged and occluded; convulsions, coma, death within days-weeks |
| Severe anemia | Hemolytic anemia from RBC destruction |
| Blackwater fever | Massive intravascular hemolysis → hemoglobinemia, hemoglobinuria, jaundice, renal failure |
| Acute kidney injury | Common in severe disease; can require dialysis |
| ARDS / pulmonary edema | Bilateral opacities on CXR; children and pregnant women most at risk |
| Thrombocytopenia | Consistent finding in severe disease |
| Hypoglycemia | Particularly with quinine treatment |
| Quartan malarial nephropathy | Chronic P. malariae → immune complex MPGN, proteinuria |
Chest X-ray in severe malaria:
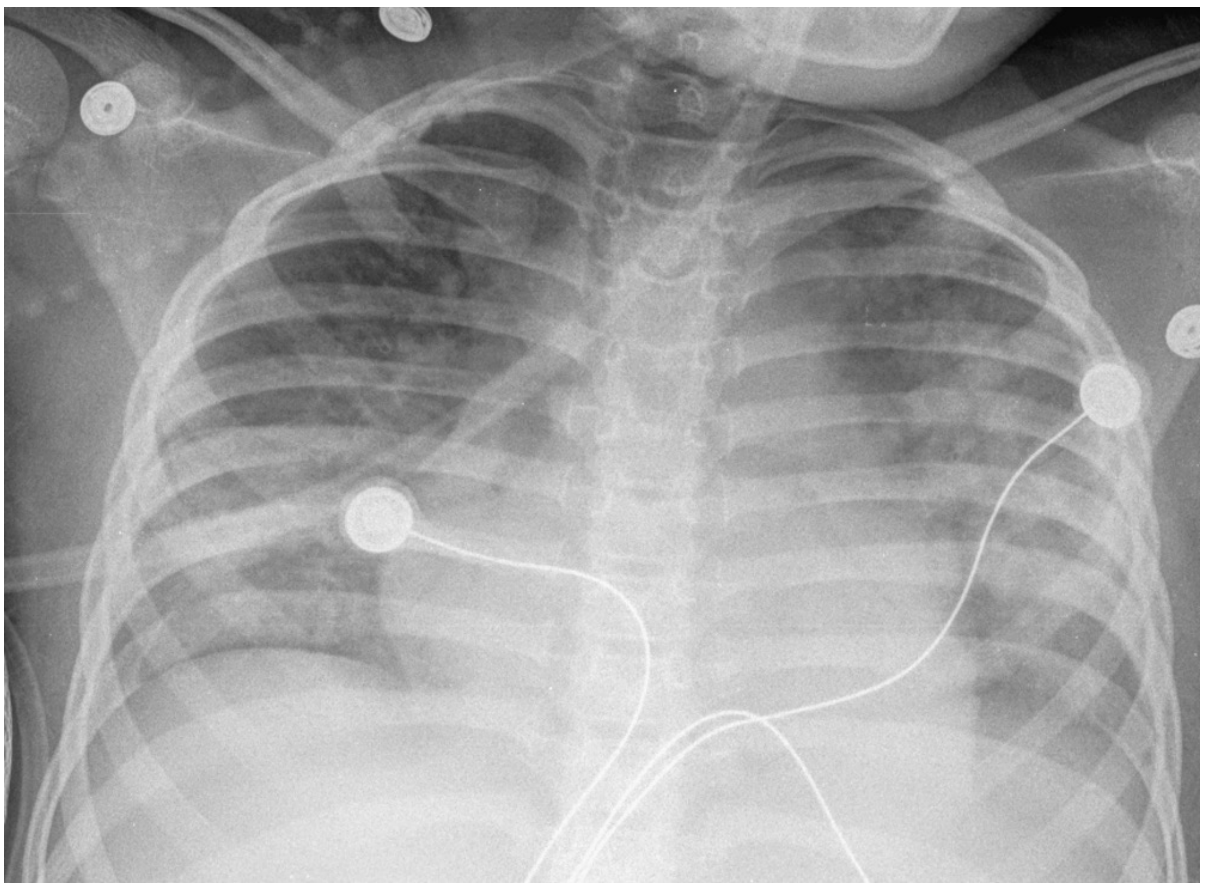
Fig: Diffuse bilateral symmetric lung opacities resembling pulmonary edema in a child with malaria (Murray & Nadel's Respiratory Medicine)
5. Pathology / Morphology
- Hemolytic anemia with characteristic lab findings
- Hematin (malarial pigment) - brown pigment derived from hemoglobin digestion; deposited in the spleen, liver, lymph nodes, and bone marrow
- Massive splenomegaly (and hepatomegaly) from hyperplasia of mononuclear phagocytes
- Cerebral vessels congested with parasitized RBCs in fatal cases
6. Diagnosis
The WHO recommends that every suspected malaria case must be confirmed by a parasite-specific laboratory test before treatment.
| Test | Notes |
|---|---|
| Thick & thin blood smears (Giemsa stain) | Gold standard; allows species ID and parasite density |
| Rapid antigen detection (RDTs) | Quick, field-deployable; detects HRP2 and other antigens |
| PCR / molecular amplification | Most sensitive; used for mixed infections, low parasitemia |
| Antibody tests | NOT recommended for acute diagnosis |
Species identification matters: P. knowlesi resembles P. malariae morphologically but is more virulent - molecular testing is needed to distinguish them.
7. Treatment
(Per WHO Guidelines for Malaria, August 2025)
Uncomplicated P. falciparum Malaria
- Artemisinin-based combination therapy (ACT) is the first-line treatment:
- Artemether/lumefantrine
- Dihydroartemisinin/piperaquine
- Artesunate/amodiaquine
- Artesunate/mefloquine
Uncomplicated P. vivax / P. ovale Malaria
- ACT or chloroquine (where chloroquine-sensitive)
- Primaquine is essential to eliminate hypnozoites (radical cure) - always check G6PD status first, as primaquine causes hemolysis in G6PD-deficient patients
- A single-dose regimen (tafenoquine) is now an alternative for patients with normal G6PD
Severe Malaria (all species)
- IV artesunate is first-line: 2.4 mg/kg by slow IV bolus at 0, 12, 24 hours, then every 24 hours
- Switch to oral ACT once patient is stable and parasitemia <1%
- If IV artesunate unavailable: IV quinine + doxycycline or clindamycin
- Careful fluid management to prevent pulmonary edema
- Treat concurrent hypoglycemia
- Artesunate resistance (slower parasite clearance) is an increasing problem in Southeast Asia
Drug Resistance
- Chloroquine resistance: widespread in P. falciparum, present in some P. vivax
- Artemisinin partial resistance: emerging in Southeast Asia (Greater Mekong Subregion) and increasingly detected in Africa, manifesting as delayed parasite clearance
- Partner drug resistance: piperaquine and mefloquine resistance complicates ACT options
8. Prevention
Personal Protection
- Insecticide-treated bed nets (ITNs/LLINs) - most effective public health intervention
- Pyrethroid-PBO nets or pyrethroid-chlorfenapyr nets in areas with pyrethroid resistance
- Indoor residual spraying (IRS)
- Repellents (DEET, picaridin)
- Protective clothing
Chemoprophylaxis for Travelers
- Atovaquone-proguanil (Malarone)
- Doxycycline
- Mefloquine
- Chloroquine (only in chloroquine-sensitive areas)
Preventive Treatment in High-Risk Groups (WHO 2025)
- Intermittent preventive treatment in pregnancy (IPTp): sulfadoxine-pyrimethamine
- Seasonal malaria chemoprevention (SMC): for children in high-transmission areas
- Perennial malaria chemoprevention (PMC): for infants in high-burden regions
- Mass drug administration (MDA): in selected low-transmission or emergency settings
Vaccines
- RTS,S/AS01 (Mosquirix) and R21/Matrix-M: approved malaria vaccines targeting the P. falciparum circumsporozoite protein. They offer partial protection and are now being deployed in high-burden African countries. Though protection is incomplete, widespread deployment is expected to prevent thousands of deaths in children annually.
9. Evolutionary and Genetic Context
Malaria has exerted profound selective pressure on human genetics. Almost all genetic RBC defects are most prevalent in malaria-endemic regions, and several protect against severe disease:
- Sickle cell trait (HbS heterozygote) - protection from severe P. falciparum
- Thalassemia - partial protection
- G6PD deficiency - some protection
- Duffy antigen negativity - near-complete protection against P. vivax (common in West African populations)
- Pyruvate kinase deficiency - partial protection
Key References
- Robbins & Kumar Basic Pathology, pp. 391-393
- Murray & Nadel's Textbook of Respiratory Medicine, Chapter 58
- Brenner & Rector's The Kidney, Chapters 20, 42-44
- WHO Guidelines for Malaria, August 2025
- Recent systematic reviews: Fadilah et al. on primaquine/hypnozoite activity (PMID: 39331646), Sultanli et al. on neonatal malaria management (PMID: 41350822)
This is a shared conversation. Sign in to Orris to start your own chat.