Jouberd syndrome
Joubert syndrome ciliopathy
Joubert syndrome molar tooth sign clinical features genetics 2025
Joubert Syndrome (JBTS)
Definition and Overview
- Bradley and Daroff's Neurology in Clinical Practice
- Brenner and Rector's The Kidney, 2-Volume Set
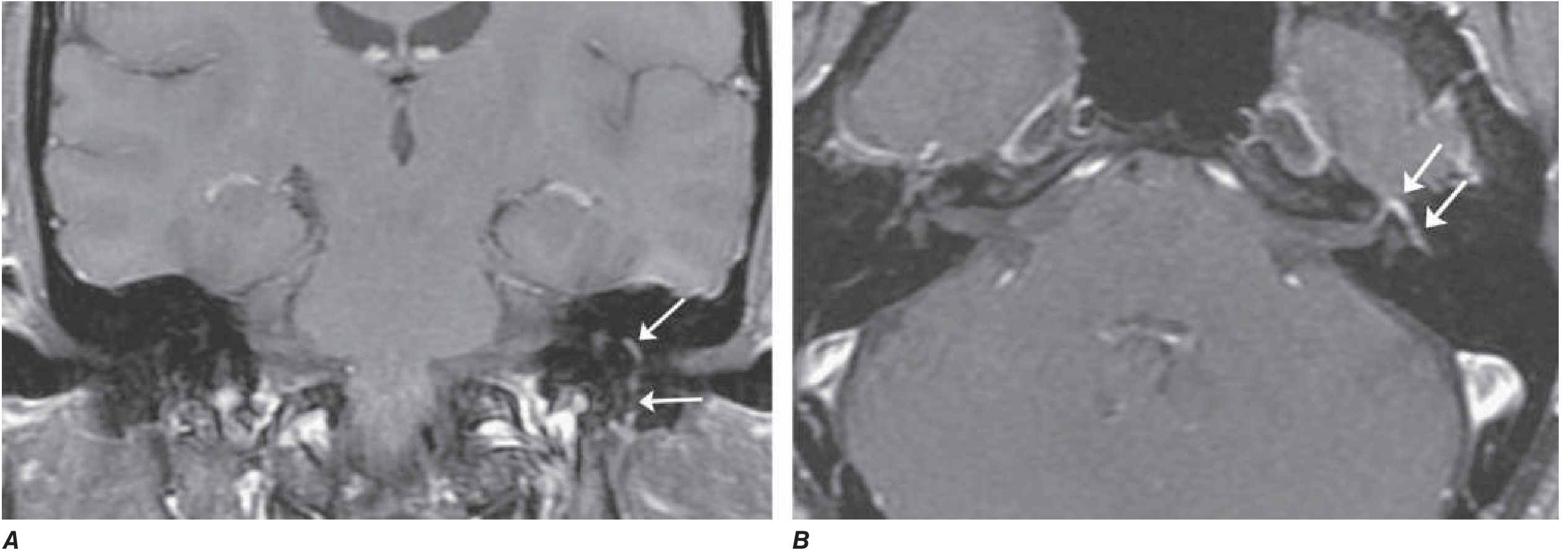
Pathognomonic Imaging: The Molar Tooth Sign
- Midbrain hypoplasia with an abnormally deep interpeduncular fossa
- Failure of the superior cerebellar peduncles to decussate across the midline (thick horizontal "roots")
- Cerebellar vermis hypoplasia/aplasia with a midline vermian cleft
- Grainger & Allison's Diagnostic Radiology
Clinical Features
Core (Obligate) Features
| Feature | Description |
|---|---|
| Cerebellar vermis aplasia/hypoplasia | Structural brain malformation |
| Hypotonia | Neonatal/infantile decreased muscle tone |
| Episodic hyperpnea | Irregular breathing pattern; neonatal tachypnea/apnea alternating |
| Oculomotor apraxia | Jerky, abnormal eye movements |
| Ataxia | Cerebellar gait and limb ataxia |
| Intellectual disability | Variable degree of cognitive impairment |
Additional/Variable Features
- Retinal dystrophy (ranging from Leber congenital amaurosis to slowly progressive retinopathy)
- Chorioretinal or optic nerve colobomas
- Ptosis, epicanthal folds
- Nephronophthisis (NPHP) - a common cause of early ESKD in JS
- Cystic dysplastic kidneys
- Glomerulocystic kidney disease
- Congenital hepatic fibrosis (CHF)
- The COACH syndrome (Cerebellar vermis hypoplasia/aplasia, Oligophrenia, Congenital Ataxia, Coloboma, Hepatic fibrosis) is a distinct JBTS subgroup, usually with TMEM67, CC2D2A, or RPGRIP1L mutations
- Postaxial polydactyly
- Severe scoliosis, skeletal dysplasia
- Situs inversus
- Congenital heart malformations
- Hirschsprung disease
- Cleft lip/palate, notched upper lip
- Lobulated tongue with multiple frenula
- Oral soft tissue tumors (hamartomas)
-
Macrocephaly, prominent forehead
-
High rounded eyebrows, upturned nose with prominent nostrils
-
Open mouth, tongue protrusion, low-set ears
-
Brenner and Rector's The Kidney; Grainger & Allison's Diagnostic Radiology
Pathophysiology: A Ciliopathy
- Brain (neurons, ependyma)
- Retinal photoreceptors
- Bile duct epithelium
- Renal tubular microtubules
Genetics
-
Inheritance: Autosomal recessive (most), rare X-linked recessive
-
Genetic heterogeneity: Extreme - over 34 causative genes have been identified (NGS-era discovery)
-
All causative gene products localize to the primary cilium, transition zone, or centrosome
-
Key genes/protein complexes include: TMEM67, CC2D2A, RPGRIP1L, CEP290 (NPHP6 - often initially presenting as Joubert), and many others
-
Gene-phenotype correlations guide surveillance:
- Highest renal risk: specific gene mutations guide avoidance of nephrotoxic medications
- CEP290 mutations: high risk for retinal dystrophy
- TMEM67 mutations: high risk for liver disease (COACH)
-
Brenner and Rector's The Kidney; Comprehensive Clinical Nephrology 7th Edition
Related Ciliopathies (Overlap Spectrum)
- Nephronophthisis (NPHP) - shares many causative genes
- Meckel-Gruber syndrome (MKS) - lethal, more severe allelic disorder
- Bardet-Biedl syndrome (BBS)
- Alstrom syndrome
Course and Prognosis
- Variable, often progressive course, though improvement occurs in some patients
- Neonatal respiratory irregularities often improve with age
- Renal disease (NPHP) is a major cause of long-term morbidity; leads to ESKD if untreated
- Hepatic fibrosis can lead to portal hypertension
- Retinal dystrophy is progressive
Management Principles
- Genetic testing - molecular diagnosis guides organ-specific surveillance intensity
- Renal monitoring - serial urinalysis, GFR, blood pressure; avoid nephrotoxic drugs in high-risk genotypes
- Ophthalmology - regular surveillance for retinal dystrophy
- Liver - serial abdominal ultrasound/Doppler, platelet count as surrogate for portal hypertension; variceal management
- Neurological/developmental - physiotherapy, occupational therapy, speech therapy
- Respiratory - supportive; neonatal respiratory monitoring
- Genetic counseling - 25% recurrence risk per pregnancy; prenatal diagnosis available
Recent literature note: A 2024 systematic review on CEP290-associated ciliopathy (PMID 39213781) describes the spectrum of extraocular features in this important JS-related gene subgroup, confirming the broad multisystem involvement pattern described above.
Bells palsy
"Bell palsy" treatment corticosteroids
Bell's palsy diagnosis treatment guidelines 2025
Bell's Palsy
Definition
- Cummings Otolaryngology Head and Neck Surgery; Harrison's Principles of Internal Medicine 22E
Epidemiology
- Annual incidence: 23-37 per 100,000 population (~1 in 60 persons over a lifetime)
- Affects men and women roughly equally
- Higher incidence in those >65 years (59/100,000); lower in children <13 years (13/100,000)
- Risk factors: Pregnancy (especially 3rd trimester and early postpartum - up to 3x risk), diabetes mellitus, hypertension
- Left and right sides equally involved
- ~30% present with incomplete paralysis; 70% with complete paralysis
- Bilateral palsy occurs in only 0.3% of cases
- Family history in 8%; recurrence rate ~7-9%
Pathophysiology
- HSV-1 DNA found in endoneurial fluid of the facial nerve in 11/14 Bell's palsy patients at surgery (Murakami et al., PCR)
- Varicella-zoster virus (VZV) accounts for up to one-third of cases and is the likely second most common cause - including zoster sine herpete (VZV without vesicles)
- Other proposed mechanisms: microcirculatory failure of the vasa nervorum, ischemic neuropathy, autoimmune reaction
- Adams and Victor's Principles of Neurology 12th Ed.; Cummings Otolaryngology
Clinical Features
| Symptom | Approximate Incidence |
|---|---|
| Facial/retroauricular pain | 60% |
| Dysgeusia (taste impairment) | 57% |
| Hyperacusis (stapedius muscle paralysis) | 30% |
| Hypesthesia/dysesthesia (glossopharyngeal/trigeminal) | 80% |
| Decreased tearing | 17% |
| Hypesthesia of C2 | 20% |
- Onset is abrupt - 50% reach maximum weakness within 48 hours; nearly all within 3-4 days
- Pain behind the ear may precede facial weakness by 1-2 days
- Taste impairment (chorda tympani involvement) usually resolves within 2 weeks
MRI Findings
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Ramsay Hunt syndrome (Herpes zoster oticus) | Severe palsy + vesicular rash in external ear canal, auricle, palate/tongue; CN VIII often involved |
| Lyme disease | Endemic area exposure; can be bilateral; serology |
| Sarcoidosis | Often bilateral; systemic features; raised ACE |
| Guillain-Barré syndrome | Bilateral facial palsy; ascending weakness |
| Parotid/CPA tumors | Progressive (not abrupt) onset - a key red flag |
| Melkersson-Rosenthal syndrome | Recurrent facial palsy + facial edema (labial) + fissured tongue |
| HIV seroconversion | Risk factor history |
| Diabetes, amyloidosis, Sjögren's | Systemic context |
| Central (UMN) lesion (stroke, MS) | Forehead spared; other CNS signs |
Red flag: Progressive facial paralysis is NOT Bell's palsy - must prompt imaging to exclude neoplasm.
Investigations
- Diagnosis is clinical - no specific diagnostic test
- EMG/nerve conduction: Useful for prognosis after 10 days - evidence of denervation indicates axonal degeneration, predicting a 3+ month delay before recovery and possible incomplete recovery
- MRI with gadolinium: May show nerve enhancement; indicated if atypical features or to exclude mass lesions
- Lyme serology in endemic areas
- CSF may show mild lymphocytosis in some cases
Prognosis
- ~70-80% recover completely within a few weeks to months
- 85% achieve near-normal function overall
- ~10% have little recovery
- Best prognostic sign: Incomplete paralysis (or some motor recovery) in the first 5-7 days
- Recovery of taste before motor function is also a good sign
- EMG denervation at 10 days = poor prognosis (axonal injury)
- Synkinesis - aberrant reinnervation causing co-contraction (e.g., "jaw winking" - eye closes when mouth opens)
- Crocodile tears - unilateral lacrimation during eating (parasympathetic fibers rerouting to lacrimal gland)
- Hemifacial spasm
Treatment
1. Corticosteroids (First-line - Strong evidence, Grade A)
- Prednisolone 25 mg twice daily for 10 days (or prednisone 60 mg/day for 5 days then tapered over 5 days)
- Increases recovery of facial function from 63% to 83% at 3 months
- Recommended by the American Academy of Neurology, AAO-HNS, and American Academy of Family Physicians
2. Antiviral Agents (Adjunct - Uncertain independent benefit)
- Acyclovir/valacyclovir alone: no independent benefit over steroids
- Combined with corticosteroids: may improve outcomes in severe cases (particularly where VZV/Ramsay Hunt is suspected)
- Typical regimen: acyclovir 400 mg 5x daily for 7 days (or valacyclovir 1000 mg TID)
- A 2025 systematic review (PMID 40741786) notes statistical fragility of the steroid-antiviral RCT evidence, and the 2024 Japanese clinical practice guidelines (PMID 39079445) provide updated evidence-based recommendations
3. Eye Care (Essential)
- Artificial tear drops during the day, lubricating eye ointment at night
- Protective eye patch, especially at night and outdoors
- Regular ophthalmology review in severe/prolonged cases
- Risk of exposure keratopathy and corneal ulceration if neglected
4. Physiotherapy
- Facial exercises, massage, and electrical stimulation may help rehabilitation
5. Surgical Decompression
- Rarely indicated; reserved for severe/prolonged cases with electrodiagnostic evidence of complete axonal degeneration
- Decompression of the meatal foramen (narrowest segment of the fallopian canal) is the surgical target
Special Populations
- Pregnancy: Managed the same way as non-pregnant patients, in collaboration with the obstetrician; corticosteroids are generally considered safe
- Children: Generally favorable prognosis; corticosteroid use follows the same principles
Generate a patient handout on Bell's palsy recovery timeline and eye care
ls -la /tmp/workspace/ 2>/dev/null || mkdir -p /tmp/workspace && ls -la /tmp/workspace/
mkdir -p /tmp/workspace/bells-palsy-handout && cat > /tmp/workspace/bells-palsy-handout/create_handout.py << 'PYEOF' from docx import Document from docx.shared import Pt, Inches, RGBColor from docx.enum.text import WD_ALIGN_PARAGRAPH from docx.oxml.ns import qn from docx.oxml import OxmlElement import copy doc = Document() # ── Page margins (narrow for handout feel) ────────────────────────────────── section = doc.sections[0] section.top_margin = Inches(0.75) section.bottom_margin = Inches(0.75) section.left_margin = Inches(0.9) section.right_margin = Inches(0.9) # ── Default body style ─────────────────────────────────────────────────────── normal = doc.styles["Normal"] normal.font.name = "Arial" normal.font.size = Pt(11) # ── Helper: add a horizontal rule ─────────────────────────────────────────── def add_hr(document): p = document.add_paragraph() p.paragraph_format.space_before = Pt(2) p.paragraph_format.space_after = Pt(2) pPr = p._p.get_or_add_pPr() pBdr = OxmlElement("w:pBdr") bottom = OxmlElement("w:bottom") bottom.set(qn("w:val"), "single") bottom.set(qn("w:sz"), "6") bottom.set(qn("w:space"), "1") bottom.set(qn("w:color"), "2E86AB") pBdr.append(bottom) pPr.append(pBdr) # ── Helper: coloured heading ───────────────────────────────────────────────── TEAL = RGBColor(0x2E, 0x86, 0xAB) # section headings ORANGE = RGBColor(0xE6, 0x77, 0x22) # warnings / call-outs DARK = RGBColor(0x1A, 0x1A, 0x2E) # dark body text def add_section_heading(document, text, color=TEAL): p = document.add_paragraph() p.paragraph_format.space_before = Pt(10) p.paragraph_format.space_after = Pt(2) run = p.add_run(text.upper()) run.bold = True run.font.size = Pt(12) run.font.color.rgb = color run.font.name = "Arial" return p def add_body(document, text, bold=False, italic=False, color=None, size=11, space_after=4): p = document.add_paragraph() p.paragraph_format.space_before = Pt(1) p.paragraph_format.space_after = Pt(space_after) run = p.add_run(text) run.bold = bold run.italic = italic run.font.size = Pt(size) run.font.name = "Arial" if color: run.font.color.rgb = color return p def add_bullet(document, text, level=0, bold_prefix=None): p = document.add_paragraph(style="List Bullet") p.paragraph_format.left_indent = Inches(0.3 + level * 0.2) p.paragraph_format.space_before = Pt(1) p.paragraph_format.space_after = Pt(2) if bold_prefix: r1 = p.add_run(bold_prefix) r1.bold = True r1.font.name = "Arial" r1.font.size = Pt(11) r2 = p.add_run(text) r2.font.name = "Arial" r2.font.size = Pt(11) else: run = p.add_run(text) run.font.name = "Arial" run.font.size = Pt(11) def add_callout(document, title, body_text, bg_color=RGBColor(0xE8, 0xF4, 0xFD), border_color="2E86AB"): """Add a shaded callout box using a table with one cell.""" tbl = document.add_table(rows=1, cols=1) tbl.style = "Table Grid" cell = tbl.cell(0, 0) # shade tcPr = cell._tc.get_or_add_tcPr() shd = OxmlElement("w:shd") shd.set(qn("w:val"), "clear") shd.set(qn("w:color"), "auto") r, g, b = bg_color shd.set(qn("w:fill"), f"{r:02X}{g:02X}{b:02X}") tcPr.append(shd) p1 = cell.paragraphs[0] p1.paragraph_format.space_before = Pt(2) p1.paragraph_format.space_after = Pt(2) r1 = p1.add_run(title + " ") r1.bold = True r1.font.color.rgb = ORANGE r1.font.name = "Arial" r1.font.size = Pt(11) r2 = p1.add_run(body_text) r2.font.name = "Arial" r2.font.size = Pt(11) document.add_paragraph().paragraph_format.space_after = Pt(2) # ═══════════════════════════════════════════════════════════════════════════ # HEADER BLOCK # ═══════════════════════════════════════════════════════════════════════════ title_p = doc.add_paragraph() title_p.alignment = WD_ALIGN_PARAGRAPH.CENTER title_p.paragraph_format.space_before = Pt(0) title_p.paragraph_format.space_after = Pt(4) tr = title_p.add_run("BELL'S PALSY") tr.bold = True tr.font.size = Pt(22) tr.font.color.rgb = TEAL tr.font.name = "Arial" sub_p = doc.add_paragraph() sub_p.alignment = WD_ALIGN_PARAGRAPH.CENTER sub_p.paragraph_format.space_after = Pt(2) sr = sub_p.add_run("Patient Information Guide: Recovery & Eye Care") sr.font.size = Pt(13) sr.font.color.rgb = DARK sr.font.name = "Arial" sr.italic = True add_hr(doc) intro = doc.add_paragraph() intro.paragraph_format.space_before = Pt(4) intro.paragraph_format.space_after = Pt(6) ri = intro.add_run( "You have been diagnosed with Bell's palsy, a temporary weakness or paralysis of the muscles on one side " "of your face. This handout explains what to expect during your recovery and how to protect your eye." ) ri.font.name = "Arial" ri.font.size = Pt(11) # ═══════════════════════════════════════════════════════════════════════════ # SECTION 1 – What Is Bell's Palsy? # ═══════════════════════════════════════════════════════════════════════════ add_section_heading(doc, "1. What Is Bell's Palsy?") add_hr(doc) add_body(doc, "Bell's palsy is caused by inflammation of the facial nerve (cranial nerve 7), most often triggered by " "reactivation of the herpes simplex virus (the same virus that causes cold sores). The nerve runs through " "a narrow bony canal in your skull; when it swells, it becomes compressed, causing weakness or complete " "paralysis of one side of your face." ) add_body(doc, "It is NOT a stroke. A stroke usually only affects the lower face; Bell's palsy affects the entire side " "including your forehead and eyelid.", bold=False, color=RGBColor(0x33, 0x33, 0x33) ) # ═══════════════════════════════════════════════════════════════════════════ # SECTION 2 – Recovery Timeline # ═══════════════════════════════════════════════════════════════════════════ add_section_heading(doc, "2. Recovery Timeline") add_hr(doc) add_body(doc, "Recovery varies from person to person, but most people recover well. Here is what is typical:", space_after=4) # Timeline table tbl = doc.add_table(rows=6, cols=2) tbl.style = "Table Grid" headers = ["Timeframe", "What to Expect"] header_row = tbl.rows[0] for i, h in enumerate(headers): cell = header_row.cells[i] p = cell.paragraphs[0] run = p.add_run(h) run.bold = True run.font.name = "Arial" run.font.size = Pt(11) run.font.color.rgb = RGBColor(0xFF, 0xFF, 0xFF) # shade header tcPr = cell._tc.get_or_add_tcPr() shd = OxmlElement("w:shd") shd.set(qn("w:val"), "clear") shd.set(qn("w:color"), "auto") shd.set(qn("w:fill"), "2E86AB") tcPr.append(shd) rows_data = [ ("Days 1-3", "Weakness reaches its worst. Pain behind the ear may be present. This is normal."), ("Days 3-10", "Inflammation peaks. Eye closure may be most difficult at this stage. Follow eye care steps carefully."), ("Weeks 2-4", "Most patients begin to notice small improvements - taste may return first, then some flicker of movement."), ("Weeks 4-8", "About 70-80% of patients recover completely by this point. Facial movements gradually strengthen."), ("3-6 Months", "Nearly 85% achieve near-normal function. A small number (about 10%) have partial or slow recovery."), ] alt_fill = RGBColor(0xEA, 0xF4, 0xFB) for i, (timeframe, detail) in enumerate(rows_data): row = tbl.rows[i + 1] # Timeframe cell c0 = row.cells[0] p0 = c0.paragraphs[0] r0 = p0.add_run(timeframe) r0.bold = True r0.font.name = "Arial" r0.font.size = Pt(11) r0.font.color.rgb = TEAL if i % 2 == 0: tcPr = c0._tc.get_or_add_tcPr() shd = OxmlElement("w:shd") shd.set(qn("w:val"), "clear") shd.set(qn("w:color"), "auto") shd.set(qn("w:fill"), "EAF4FB") tcPr.append(shd) # Detail cell c1 = row.cells[1] p1 = c1.paragraphs[0] r1 = p1.add_run(detail) r1.font.name = "Arial" r1.font.size = Pt(11) if i % 2 == 0: tcPr = c1._tc.get_or_add_tcPr() shd = OxmlElement("w:shd") shd.set(qn("w:val"), "clear") shd.set(qn("w:color"), "auto") shd.set(qn("w:fill"), "EAF4FB") tcPr.append(shd) doc.add_paragraph().paragraph_format.space_after = Pt(4) add_body(doc, "Good signs of recovery:", bold=True, color=TEAL, space_after=2) add_bullet(doc, "Some movement returning in the first 5-7 days") add_bullet(doc, "Taste sensation returning in the first 1-2 weeks") add_bullet(doc, "Incomplete (partial) paralysis at the start is a very good sign") # ═══════════════════════════════════════════════════════════════════════════ # SECTION 3 – Eye Care (CRITICAL) # ═══════════════════════════════════════════════════════════════════════════ add_section_heading(doc, "3. Eye Care - This Is the Most Important Part", color=ORANGE) add_hr(doc) add_body(doc, "Because your eyelid may not close fully, your eye cannot protect itself. Tears evaporate faster, " "and the cornea (clear front surface of your eye) can become dry, scratched, or infected. This can " "cause permanent vision damage if not managed carefully.", space_after=6 ) add_callout(doc, "WARNING:", " Never go to sleep without protecting your eye. A dry or scratched cornea can cause permanent scarring.", bg_color=RGBColor(0xFF, 0xF3, 0xE0) ) add_body(doc, "Your daily eye care routine:", bold=True, color=TEAL, space_after=2) add_bullet(doc, " Artificial tear eye drops (preservative-free preferred) - use every 1-2 hours while awake, or whenever your eye feels dry or gritty.", bold_prefix="During the day:") add_bullet(doc, " Apply a thick lubricating eye ointment (e.g., Lacri-Lube or equivalent) before sleeping. This stays in longer than drops.", bold_prefix="At bedtime:") add_bullet(doc, " Use a moisture chamber goggle or firmly tape your eyelid shut with micropore tape to keep it closed overnight.", bold_prefix="Eye protection at night:") add_bullet(doc, " Wear sunglasses or protective glasses when outdoors or in windy conditions.", bold_prefix="When outdoors:") add_bullet(doc, " Tilt your head slightly upward and manually close the eye using a clean finger when eating, laughing, or coughing, if your eye tends to water or open.", bold_prefix="During meals/activity:") doc.add_paragraph().paragraph_format.space_after = Pt(2) add_body(doc, "How to tape your eyelid shut at night:", bold=True, space_after=2) add_bullet(doc, "Apply lubricating ointment first.") add_bullet(doc, "Gently close your eye.") add_bullet(doc, "Place a strip of micropore (paper) tape horizontally across the eyelid.") add_bullet(doc, "Do not pull the skin tight - just enough to keep the lid closed.") add_bullet(doc, "Remove gently in the morning using warm water or a damp cloth.") # ═══════════════════════════════════════════════════════════════════════════ # SECTION 4 – Seek Help Immediately If... # ═══════════════════════════════════════════════════════════════════════════ add_section_heading(doc, "4. Seek Medical Help Immediately If...", color=ORANGE) add_hr(doc) warning_items = [ "Your eye becomes red, painful, or your vision changes - this may mean a corneal injury", "You develop a rash or blisters around your ear, mouth, or scalp (may indicate Ramsay Hunt syndrome requiring stronger antiviral treatment)", "Both sides of your face are affected", "Your weakness is getting worse after 3 weeks, or you see no improvement at all by 3 months", "You develop new symptoms such as difficulty swallowing, hearing loss, or limb weakness", ] for item in warning_items: add_bullet(doc, item) # ═══════════════════════════════════════════════════════════════════════════ # SECTION 5 – Your Medications # ═══════════════════════════════════════════════════════════════════════════ add_section_heading(doc, "5. Your Medications") add_hr(doc) add_body(doc, "Your doctor may have prescribed one or both of the following. Take them exactly as directed - they work " "best when started within 72 hours of your symptoms beginning.", space_after=4 ) add_bullet(doc, " Reduces inflammation of the facial nerve. Take with food. Do not stop suddenly - finish the full course.", bold_prefix="Corticosteroids (e.g., prednisolone): ") add_bullet(doc, " Targets the herpes virus that may be triggering the inflammation. Take all doses as prescribed.", bold_prefix="Antiviral medication (e.g., acyclovir/valacyclovir): ") # ═══════════════════════════════════════════════════════════════════════════ # SECTION 6 – Facial Exercises # ═══════════════════════════════════════════════════════════════════════════ add_section_heading(doc, "6. Facial Exercises") add_hr(doc) add_body(doc, "Once movement begins to return (usually after week 2-3), gentle facial exercises can help stimulate " "nerve recovery. Do each exercise slowly, 5-10 times, 2-3 times per day:", space_after=4 ) exercises = [ ("Eyebrow raise", "Raise both eyebrows as high as you can, hold 2 seconds, relax."), ("Eyelid squeeze", "Gently try to close both eyes tightly, hold 2 seconds. Do NOT strain."), ("Smile", "Try to smile broadly showing teeth, hold 2 seconds, relax."), ("Puff cheeks", "Puff out both cheeks with air, hold 2 seconds, release."), ("Nose wrinkle", "Wrinkle your nose as if smelling something bad, hold 2 seconds."), ("Lower lip pull", "Pull down the lower lip on the affected side, hold 2 seconds."), ] for name, desc in exercises: add_bullet(doc, f" {desc}", bold_prefix=f"{name}: ") add_callout(doc, "Note:", " Do not force movements that are not yet returning. Gentle stimulation only - overexertion will not speed recovery.", bg_color=RGBColor(0xE8, 0xF8, 0xE8) ) # ═══════════════════════════════════════════════════════════════════════════ # SECTION 7 – Long-Term: What to Watch For # ═══════════════════════════════════════════════════════════════════════════ add_section_heading(doc, "7. Long-Term Recovery: What to Watch For") add_hr(doc) add_body(doc, "Most people recover fully. However, in a small number of cases, the nerve may not regenerate perfectly, leading to:" ) add_bullet(doc, " When you move your mouth (smile, chew), your eye involuntarily blinks on the same side. This is normal nerve regrowth and can improve with physiotherapy.", bold_prefix="Synkinesis (co-contraction): ") add_bullet(doc, " Tearing on one side when you eat or smell food. This happens when nerve fibres regrow along the wrong path.", bold_prefix="'Crocodile tears': ") add_bullet(doc, " Tightness or pulling sensation in the face.", bold_prefix="Hemifacial spasm: ") add_body(doc, "If any of these develop, discuss them with your doctor. Physiotherapy and in some cases Botulinum toxin (Botox) injections can help.", italic=True, color=RGBColor(0x55, 0x55, 0x55) ) # ═══════════════════════════════════════════════════════════════════════════ # SECTION 8 – Follow-Up # ═══════════════════════════════════════════════════════════════════════════ add_section_heading(doc, "8. Your Follow-Up Appointments") add_hr(doc) add_bullet(doc, "See your GP or neurologist at 4 weeks to assess progress.") add_bullet(doc, "If no improvement by 3 months, a nerve conduction study (EMG) or MRI may be arranged.") add_bullet(doc, "See an ophthalmologist (eye doctor) early if you have any eye pain, redness, or vision changes.") # ═══════════════════════════════════════════════════════════════════════════ # FOOTER # ═══════════════════════════════════════════════════════════════════════════ add_hr(doc) footer_p = doc.add_paragraph() footer_p.alignment = WD_ALIGN_PARAGRAPH.CENTER footer_p.paragraph_format.space_before = Pt(4) fr = footer_p.add_run( "This handout is for general information only and does not replace your doctor's advice. " "Always follow the specific instructions given to you by your healthcare team." ) fr.font.size = Pt(9) fr.font.color.rgb = RGBColor(0x88, 0x88, 0x88) fr.font.name = "Arial" fr.italic = True out = "/tmp/workspace/bells-palsy-handout/Bells_Palsy_Patient_Handout.docx" doc.save(out) print(f"Saved: {out}") PYEOF python3 /tmp/workspace/bells-palsy-handout/create_handout.py
Bells Palsy Patient Handout
Word Document · DOCX
- What Is Bell's Palsy? - Simple explanation of the nerve inflammation and why it is not a stroke
- Recovery Timeline - Colour-coded table from Days 1-3 through 3-6 months, with good prognostic signs highlighted
- Eye Care - The most detailed section (flagged in orange as the highest priority), covering:
- Daytime drops, bedtime ointment, overnight taping technique, and outdoor protection
- Step-by-step eyelid taping instructions
- A bold warning callout about overnight eye protection
- Seek Help Immediately If... - Red-flag symptoms listed clearly
- Medications - Corticosteroids and antivirals explained in plain terms
- Facial Exercises - 6 named exercises with instructions, plus a caution not to force movements
- Long-Term Watch - Synkinesis, crocodile tears, and hemifacial spasm explained simply
- Follow-Up Appointments - GP, neurology, and ophthalmology timelines