Functional areas of brain
Reading File
Finding Sources
Searching the Web
functional areas of the brain cerebral cortex lobes
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
Now I have rich content from multiple authoritative textbooks and excellent diagrams. Let me compile the comprehensive answer.
Functional Areas of the Brain
The cerebral cortex - a thin (2-5 mm) layer covering the brain's surface containing over 80 billion neurons - is organized into discrete functional regions. Korbinian Brodmann (1909) mapped 52 cytoarchitecturally distinct areas, still used today as reference. The cortex broadly divides into motor areas, sensory areas, and association areas.
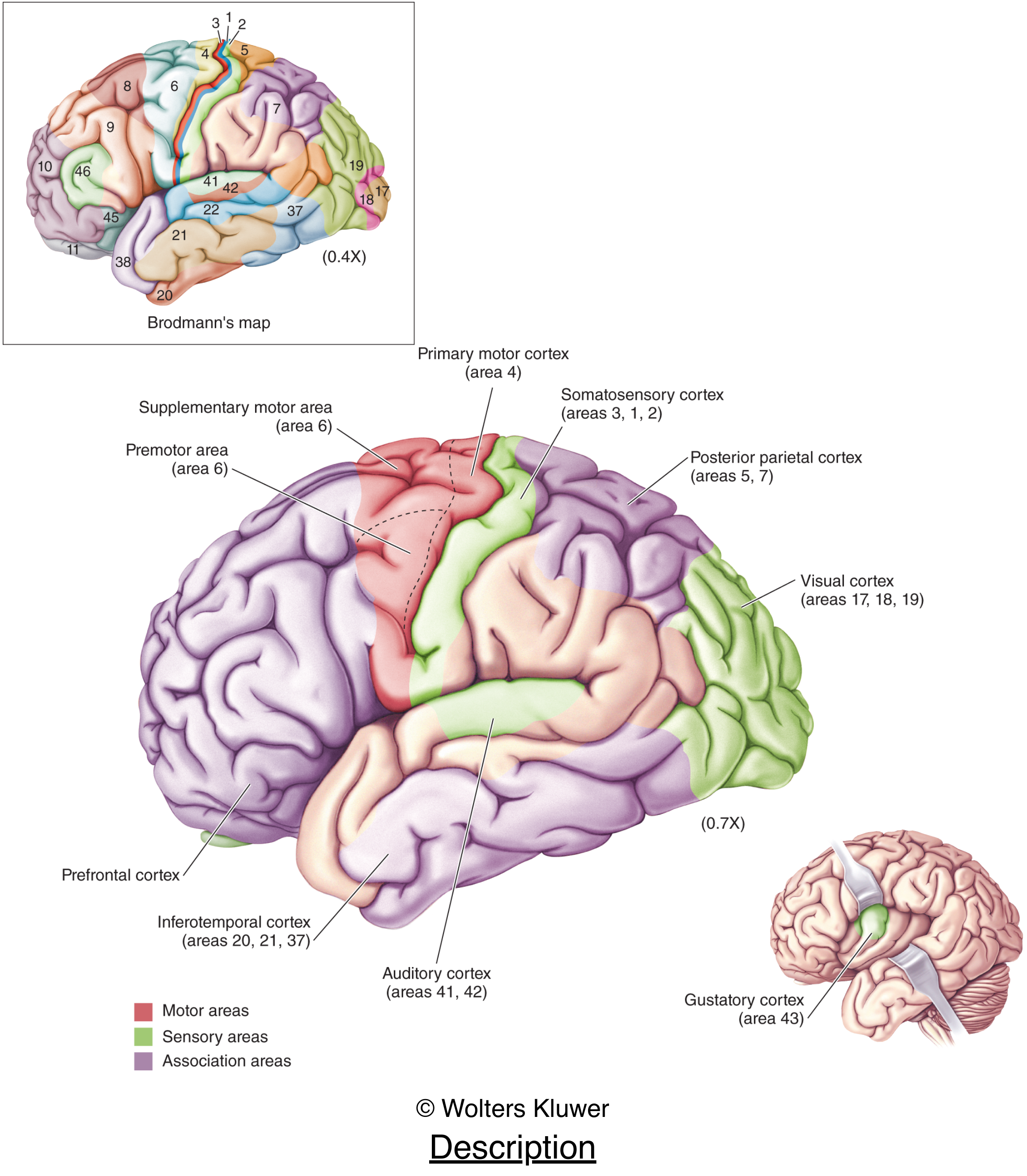
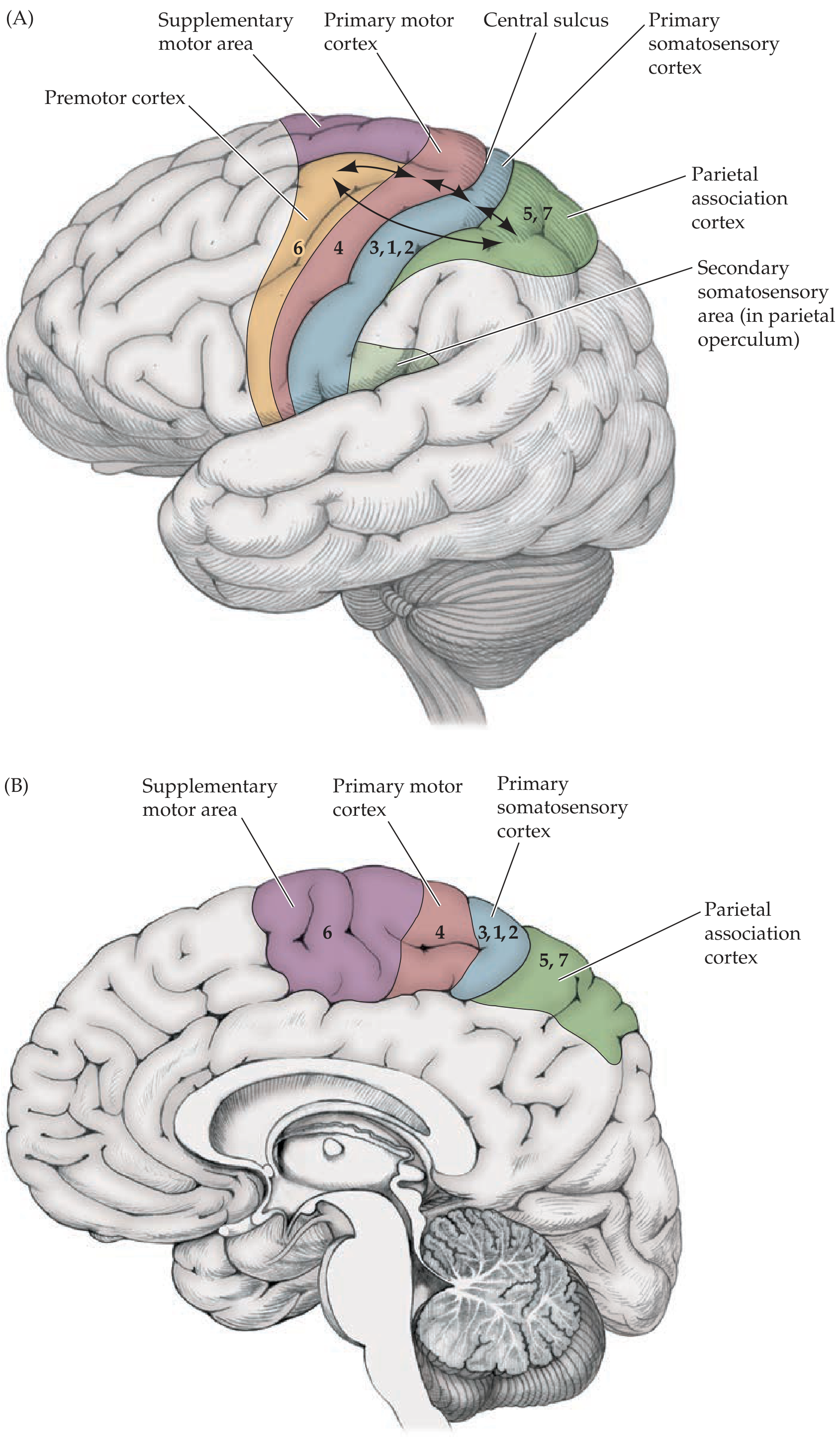
1. Motor Areas (Frontal Lobe)
Primary Motor Cortex - Brodmann Area 4
- Location: Precentral gyrus, just anterior to the central (Rolandic) sulcus
- Function: Voluntary movement control; sends long fibers down the corticospinal tract to spinal cord motor neurons
- Key feature: Somatotopically organized - the motor homunculus maps body parts to cortical regions, with the face and hands having disproportionately large representations
Premotor Cortex - Brodmann Area 6
- Location: Lateral surface, just anterior to primary motor cortex
- Function: Higher-order planning and preparation for limb movements; guides movements based on sensory cues
Supplementary Motor Area (SMA) - Brodmann Area 6 (medial)
- Location: Medial surface of the frontal lobe
- Function: Planning and sequencing of complex voluntary movements; bilateral coordination
Frontal Eye Fields - Brodmann Area 8
- Location: Middle and superior frontal gyri
- Function: Voluntary saccadic (rapid) eye movements
Broca's Area - Brodmann Areas 44 & 45
- Location: Posterior part of the inferior frontal gyrus (triangular and opercular portions), left hemisphere in most right-handers
- Function: Speech production (expressive language); damage causes Broca's aphasia - non-fluent speech with intact comprehension
2. Somatosensory Areas (Parietal Lobe)
Primary Somatosensory Cortex - Brodmann Areas 3, 1, 2
- Location: Postcentral gyrus, immediately posterior to the central sulcus
- Function: Receives and processes touch, pain, temperature, proprioception from the contralateral body
- Key feature: The sensory homunculus maps body surface onto the cortex; hands, lips, and tongue have the largest representations
Secondary Somatosensory Cortex
- Location: Parietal operculum (lower end of postcentral gyrus, abutting the Sylvian fissure)
- Function: Further processing of touch and pain; integrates input from both sides of the body
Posterior Parietal Cortex - Brodmann Areas 5 & 7
- Location: Superior parietal lobule
- Function: Visuomotor integration, spatial perception, stereognosis (recognizing objects by touch); damage causes apraxia and spatial neglect
Inferior Parietal Lobule - Brodmann Areas 39 & 40
- Supramarginal gyrus (Area 40): Reading, phonological processing
- Angular gyrus (Area 39): Language comprehension, reading, writing, arithmetic
- Wernicke's Area (posterior Area 22 + Area 39/40): Language comprehension; damage causes Wernicke's aphasia - fluent but meaningless speech
3. Visual Areas (Occipital Lobe)
| Area | Brodmann | Location | Function |
|---|---|---|---|
| Primary visual cortex (V1) | 17 | Banks of the calcarine fissure | Basic visual perception (edges, orientation) |
| Secondary visual cortex (V2) | 18 | Medial & lateral occipital gyri | Depth, color processing |
| Tertiary visual cortex (V3/V5) | 19 | Lateral occipital gyri | Color, motion, depth |
Two major visual processing streams arise from V1:
- Dorsal stream ("where/how"): V1 → parietal cortex - spatial location and visually-guided movement
- Ventral stream ("what"): V1 → inferotemporal cortex - object and face recognition
4. Auditory Areas (Temporal Lobe)
| Area | Brodmann | Location | Function |
|---|---|---|---|
| Primary auditory cortex (A1) | 41 | Heschl's gyrus (transverse temporal gyrus), on the superior surface of the superior temporal gyrus | Sound frequency (tonotopic organization) |
| Secondary auditory cortex | 42 | Superior temporal gyrus adjacent to Heschl | Speech and complex sound processing |
| Higher-order auditory cortex | 22 | Superior temporal gyrus | Language comprehension (includes Wernicke's area posteriorly) |
Important asymmetry: The planum temporale (posterior to Heschl's gyrus) is ~1/3 larger in the left hemisphere in most right-handers, correlating with language dominance.
5. Other Specific Sensory Areas
| Sense | Area | Location |
|---|---|---|
| Olfactory (smell) | Areas 28, 34, 35, 38 | Parahippocampal gyrus, temporal pole, pyriform cortex |
| Gustatory (taste) | Area 43 | Parietal operculum / insula (buried in Sylvian fissure) |
| Vestibular | Area 2v | Parietal operculum |
6. Association Areas
These make up the bulk of the human cortex and integrate information across modalities:
Prefrontal Cortex - Brodmann Areas 9, 10, 11, 12, 46
- Function: Working memory, executive function, decision-making, personality, abstract thinking, impulse control; damage causes frontal lobe syndrome (disinhibition, poor planning)
- Dorsolateral prefrontal cortex (DLPFC): Working memory and planning
- Orbitofrontal cortex: Reward processing and social behavior
Posterior Parietal - Temporal - Occipital (PTO) Association Cortex - Area 37, 39, 40
- Multimodal integration of vision, touch, and spatial information; critical for reading and calculation
Inferotemporal Cortex - Areas 20, 21, 37
- Function: Complex object recognition, face recognition (fusiform face area), form vision
Limbic Association Cortex - Areas 23-32, cingulate gyrus
- Function: Emotion processing, memory consolidation, motivation; forms part of the Papez circuit
7. The Sensory & Motor Homunculi
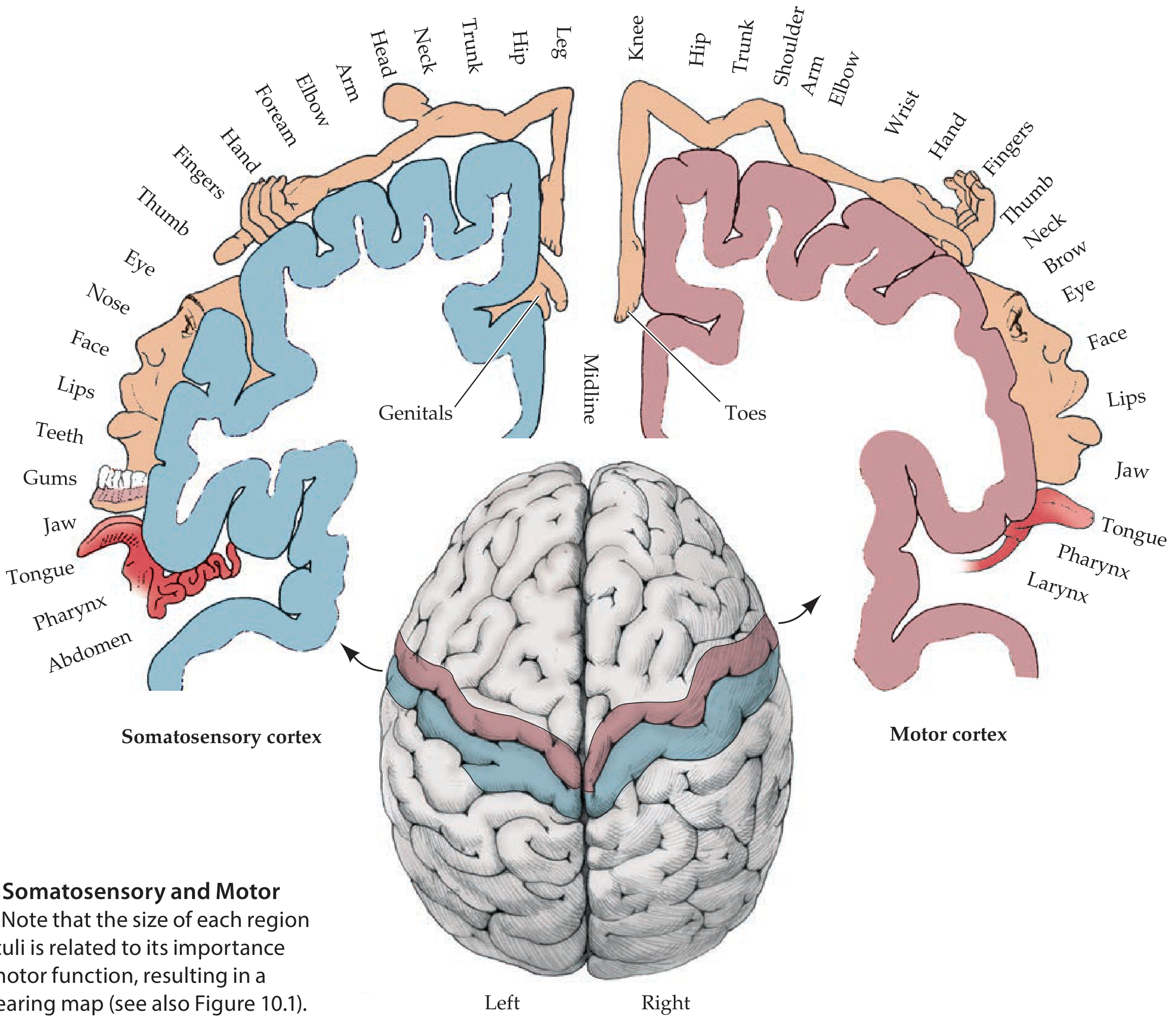
The cortical representation of body parts is proportional to functional importance, not body size. The hands, face, lips, and tongue occupy far more cortical area than the trunk or legs, reflecting the precision of movement and sensitivity required.
Summary Table: Brodmann Areas Quick Reference
| Brodmann Area | Functional Area | Key Function |
|---|---|---|
| 1, 2, 3 | Primary somatosensory cortex | Touch/proprioception |
| 4 | Primary motor cortex | Voluntary movement |
| 5, 7 | Posterior parietal association | Spatial/visuomotor |
| 6 | Premotor + SMA | Movement planning |
| 8 | Frontal eye fields | Saccadic eye movements |
| 9-12, 46 | Prefrontal cortex | Executive function |
| 17 | Primary visual cortex (V1) | Basic vision |
| 18-19 | Secondary/tertiary visual | Color, depth, motion |
| 20, 21 | Inferotemporal | Object/face recognition |
| 22 | Higher auditory cortex | Speech comprehension |
| 41, 42 | Primary/secondary auditory | Hearing |
| 44, 45 | Broca's area | Speech production |
| 39 | Angular gyrus | Reading, language |
| 40 | Supramarginal gyrus | Phonological processing |
Sources: - Neuroanatomy through Clinical Cases 3rd Ed. - Neuroscience: Exploring the Brain 5th Ed. - Guyton & Hall Medical Physiology - Localization in Clinical Neurology 8e
Wallenberg syndrome
Reading File
Searching the Web
Wallenberg syndrome lateral medullary syndrome clinical features management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Wallenberg Syndrome (Lateral Medullary Syndrome)
Eponym: Named after German neurologist Adolf Wallenberg, who described it in 1895 and provided the precise anatomical description in 1901.
Also called: Posterior Inferior Cerebellar Artery (PICA) syndrome, Vertebral Artery syndrome, Lateral Medullary Syndrome (LMS).
Anatomy of the Lateral Medulla
The lateral medulla contains a wedge-shaped region supplied by the PICA (or directly by the vertebral artery). The structures packed into this small area explain the rich clinical syndrome:
| Structure | Function |
|---|---|
| Spinal nucleus & tract of CN V (trigeminal) | Ipsilateral facial pain/temperature |
| Spinothalamic tract | Contralateral body pain/temperature |
| Nucleus ambiguus (CN IX, X, XI) | Swallowing, phonation, palatal elevation |
| Descending sympathetic fibers | Ipsilateral Horner's syndrome |
| Vestibular nuclei | Vertigo, nystagmus, nausea/vomiting |
| Inferior cerebellar peduncle | Ipsilateral cerebellar signs |
| Nucleus tractus solitarius | Taste, autonomic regulation |
The pyramidal tract, tongue (CN XII), and dorsal columns are spared, as they lie in the medial medulla.
Etiology
Most commonly caused by ischemic infarction of the dorsolateral medulla. In a series of 130 consecutive patients with pure lateral medullary infarctions:
- Large vessel atherosclerosis (vertebral or PICA stenosis/occlusion): ~50%
- Vertebral artery dissection: ~15% - especially in younger patients, often preceded by neck pain or recent neck manipulation
- Small vessel disease: ~13%
- Cardioembolism: ~5%
Less common causes include cocaine abuse, medullary tumors (usually metastases), demyelination (MS), abscess, vascular malformation hemorrhage, radionecrosis, and neck trauma.
Classic Clinical Features
The hallmark is a crossed sensory deficit - ipsilateral face, contralateral body.
1. Sensory
- Ipsilateral facial hypalgesia and thermoanesthesia - loss of pain and temperature on the same side face (spinal nucleus/tract of CN V)
- Contralateral body hypalgesia and thermoanesthesia - loss of pain and temperature in the trunk and limbs on the opposite side (spinothalamic tract)
- Vibration, proprioception, and touch are preserved (medial lemniscus is in medial medulla)
2. Motor/Bulbar
- Dysphagia - difficulty swallowing
- Dysarthria/dysphonia/hoarseness - weakness of palate, pharynx, vocal cord
- Ipsilateral palatal, pharyngeal, and vocal cord paralysis (nucleus ambiguus involvement - CN IX, X)
- No limb weakness (pyramids are spared)
3. Sympathetic
- Ipsilateral Horner's syndrome - ptosis, miosis, anhidrosis (descending hypothalamospinal sympathetic fibers)
4. Vestibular/Cerebellar
- Vertigo, nausea, vomiting (vestibular nuclei)
- Nystagmus (horizontal, torsional, or mixed)
- Ipsilateral cerebellar ataxia - limb ataxia, gait ataxia, falling to the side of the lesion (inferior cerebellar peduncle)
- Lateropulsion - strong tendency to fall/veer toward the side of the lesion
5. Ocular
- Skew deviation and ocular tilt reaction
- Multiple types of nystagmus (horizontal, torsional, mixed)
- Gaze-holding abnormalities
- Smooth pursuit defects
The Triad
The clinical triad of Horner syndrome + ipsilateral ataxia + contralateral hypalgesia is the best identifier of lateral medullary infarction.
Rare/Additional Features
Described in extensive case series:
- Wild arm ataxia (lateral cuneate nucleus involvement)
- Central neuropathic pain with allodynia
- Loss of taste (nucleus tractus solitarius - rostral/lateral zone)
- Inability to sneeze (sneezing center in spinal trigeminal nucleus)
- Autonomic dysfunction - tachycardia, blood pressure lability
- Ondine's curse (central hypoventilation syndrome) - failure of automatic breathing; life-threatening if not recognized; due to lesions of nucleus ambiguus and adjacent reticular formation
- Contralateral hyperhidrosis with ipsilateral anhidrosis (sympathetic disruption)
- Opalski syndrome - Wallenberg + ipsilateral hemiparesis (lesion extends to pyramidal decussation at the caudal medulla)
Sensory Pattern Variants
The crossed pattern is the classic presentation, but variants occur based on lesion location:
- Far lateral lesion: Ipsilateral face + contralateral foot/leg only (selective sacral/lumbar spinothalamic fibers hit, which are located most laterally)
- Mediolateral lesion: Ipsilateral face + contralateral entire hemibody (unilateral pattern) - ventral trigeminothalamic tract also affected
- Rostral medullary lesion: More severe dysphagia, hoarseness, facial paresis
- Caudal medullary lesion: More marked vertigo, nystagmus, gait ataxia
Diagnosis
Imaging
- MRI with diffusion-weighted imaging (DWI) is the investigation of choice - confirms the infarct in the lateral medulla
- DWI positive from day 1 (earliest indicator)
- T2-weighted MRI may not show the infarct initially; becomes visible after several days
- MRA (MR Angiography) - shows loss of flow in the vertebral artery or PICA; identifies arterial dissection
- T1-weighted axial MRI through the vertebral arteries - bright intramural signal (crescent sign) indicates vertebral dissection
Treatment
| Aspect | Management |
|---|---|
| Acute ischemic stroke | IV thrombolysis (tPA) within 4.5 hours if eligible (high risk in this region - use with caution) |
| Vertebral dissection | Antiplatelet agents (aspirin); some use anticoagulation (controversial) |
| Atherosclerotic disease | Antiplatelet therapy (aspirin, clopidogrel), statins, blood pressure control |
| Dysphagia | Nasogastric feeding, speech therapy, swallowing rehabilitation |
| Nausea/vertigo | Antiemetics, vestibular suppressants short-term |
| Neuropathic pain | Gabapentin, TCAs, or other neuropathic pain agents |
| Ondine's curse | Mechanical ventilation, close respiratory monitoring |
| Rehabilitation | Physiotherapy (ataxia, lateropulsion), speech therapy, occupational therapy |
Prognosis
Recovery is generally good for most deficits. In the case example from the textbook, at 11-day follow-up, the patient no longer had nausea, vertigo, or nystagmus and could walk, with only mild residual Horner's, slight sensory deficit, and trace ataxia. Dysphagia and ataxia typically improve over weeks to months. Neuropathic pain can be a persistent, troublesome long-term complication.
- Wallenberg syndrome is the most common posterior circulation stroke syndrome, accounting for ~2-3% of all ischemic strokes
- It is the most prevalent syndrome related to intracranial vertebral artery occlusion
Memory Aid
"AEIOU" or think of the lateral medulla contents:
Ipsilateral side (same as lesion): Horner's + facial pain/temp loss + cerebellar ataxia + bulbar palsy (dysphagia, hoarseness) Contralateral side (opposite): body pain/temp loss
Spared (medial medulla): Motor power of limbs, tongue, vibration/proprioception
Sources: - Localization in Clinical Neurology, 8e - Neuroanatomy through Clinical Cases 3rd Ed. - K.J. Lee's Essential Otolaryngology
Circle of willis for anatomy test
Reading File
Finding Sources
Searching the Web
circle of Willis anatomy components branches clinical importance
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Finding Sources
I now have all the material needed for a thorough, exam-ready answer. Let me compile it.
Circle of Willis - Complete Anatomy Guide
Overview
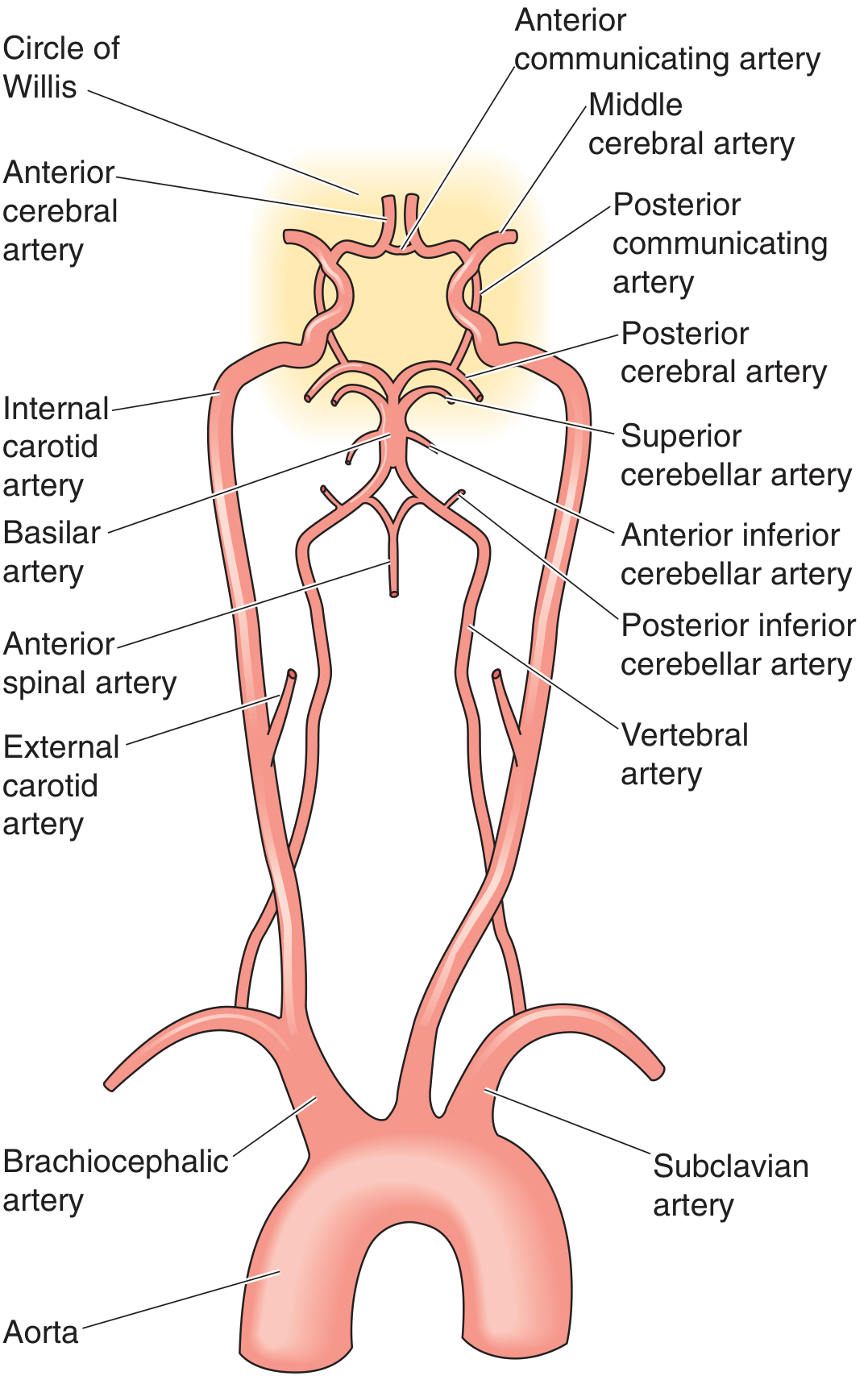
The Circle of Willis (circulus arteriosus cerebri) is an anastomotic arterial ring at the base of the brain, located in the interpeduncular cistern of the subarachnoid space, surrounding the ventral surface of the diencephalon. It connects the anterior circulation (internal carotid arteries) with the posterior circulation (vertebrobasilar system), providing collateral pathways if any one vessel is occluded.
A complete, full-caliber Circle of Willis is present in only ~34% of individuals - anatomical variants are the rule, not the exception.
Formation - From Aorta to Circle
Anterior Circulation (Internal Carotid System)
- Aorta → brachiocephalic artery (right) / direct (left) → common carotid arteries
- Common carotid bifurcates → internal carotid artery (ICA) + external carotid artery
- ICA ascends through carotid canal → cavernous sinus (carotid siphon S-bend) → pierces dura → supraclinoid segment
- ICA terminal branches (mnemonic OPAAM):
- Ophthalmic artery
- Posterior communicating artery (PComm)
- Anterior choroidal artery
- Anterior cerebral artery (ACA)
- Middle cerebral artery (MCA)
Posterior Circulation (Vertebrobasilar System)
- Subclavian arteries → vertebral arteries (ascend through foramina transversaria of C6-C1)
- Vertebral arteries enter foramen magnum → unite at pontomedullary junction to form basilar artery
- Basilar artery ascends along ventral pons → terminates at midbrain by bifurcating into posterior cerebral arteries (PCA)
Components of the Circle
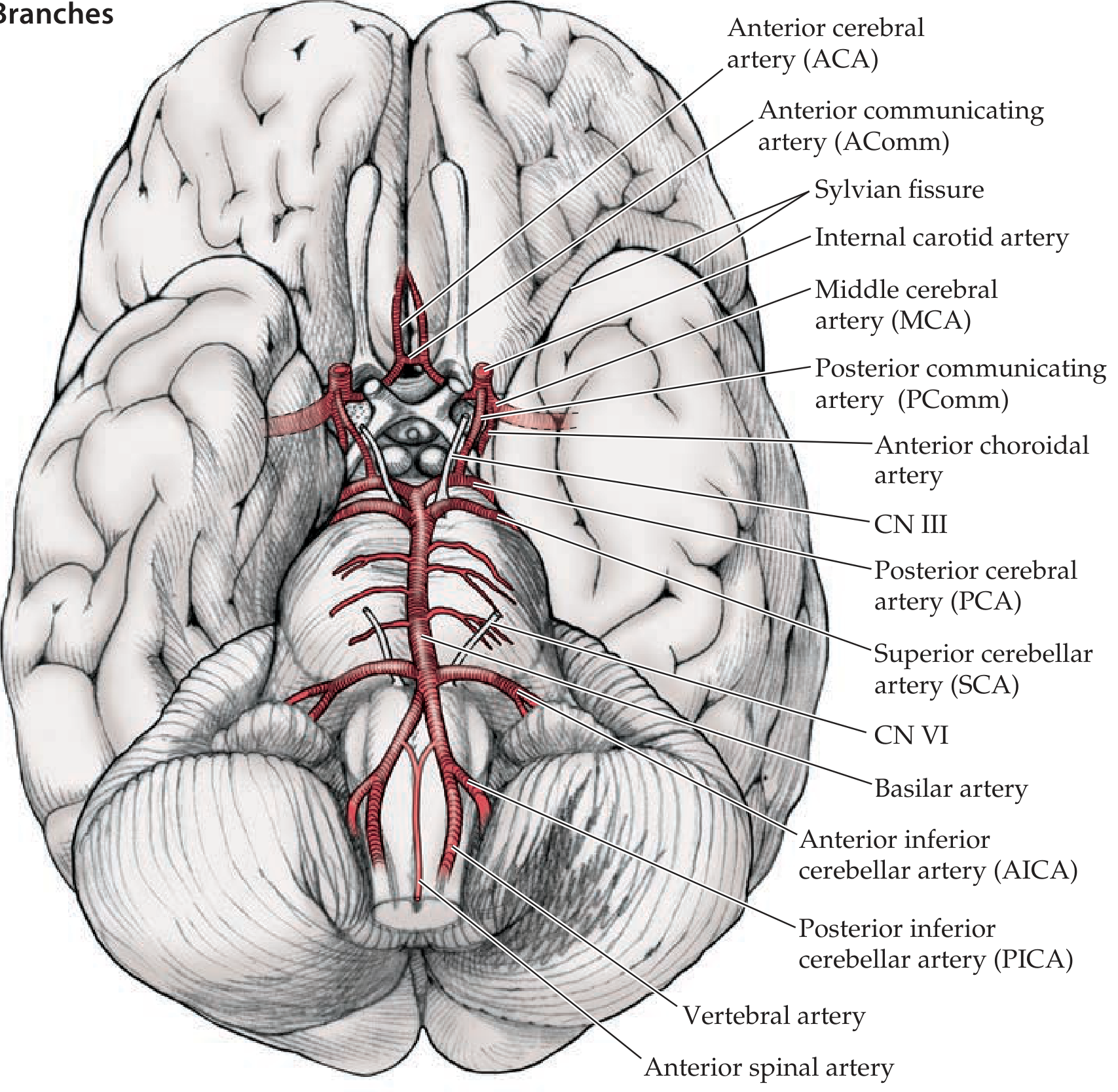
The circle itself is formed by 9 vessels:
| Vessel | Number | Origin | Position in Circle |
|---|---|---|---|
| Internal carotid artery (ICA) | ×2 | Common carotid | Lateral inflow |
| Anterior cerebral artery (ACA) - A1 segment | ×2 | ICA | Anterior |
| Anterior communicating artery (AComm) | ×1 | Connects L+R ACA | Anterior midline connector |
| Posterior communicating artery (PComm) | ×2 | ICA | Links anterior + posterior |
| Posterior cerebral artery (PCA) - P1 segment | ×2 | Basilar artery | Posterior |
The MCA does NOT form part of the circle - it is a terminal branch of the ICA that exits laterally.
Architecture: Anterior vs. Posterior
AComm
ACA ——|—— ACA
| |
ICA ICA
| |
PComm PComm
| |
PCA ——basilar—— PCA
(top of basilar)
Anterior part of the circle:
- Right ACA (A1) + AComm + Left ACA (A1)
Posterior part of the circle:
- Right PCA (P1) + Right PComm → Right ICA ← Left ICA ← Left PComm + Left PCA (P1)
The Three Main Cerebral Arteries and Their Territories
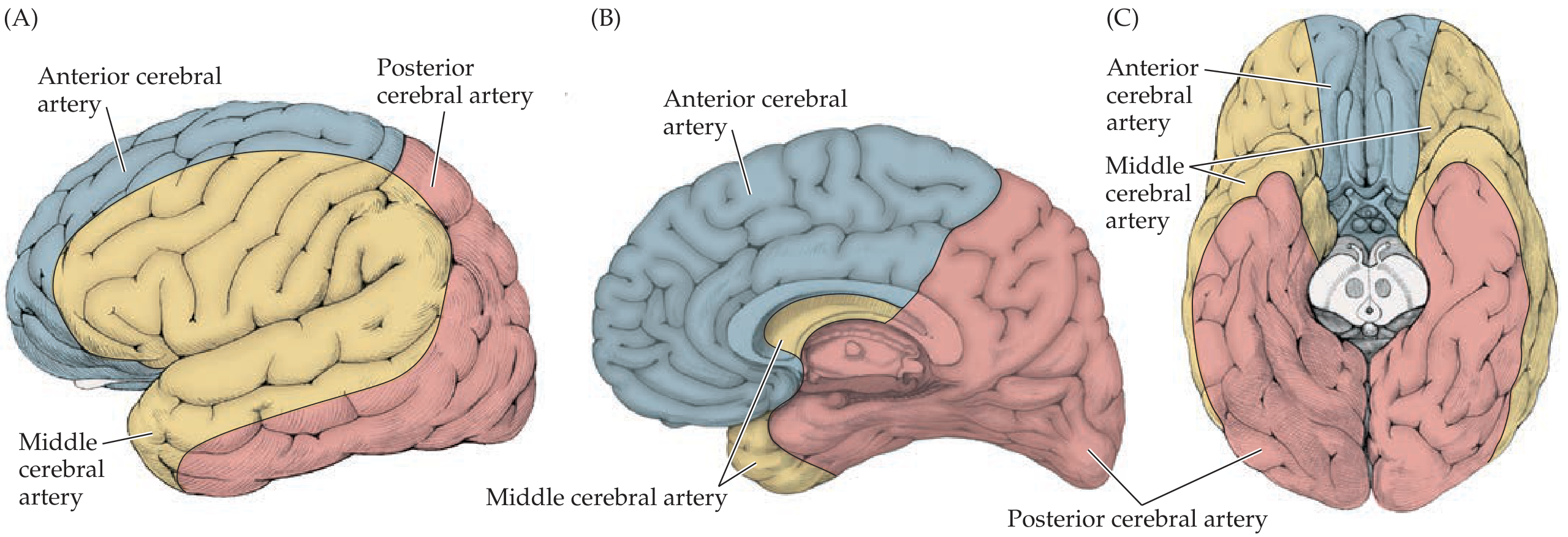
Anterior Cerebral Artery (ACA)
- Passes forward and medially, then curves up and over the corpus callosum in the interhemispheric fissure
- Major branches: pericallosal and callosomarginal arteries
- Territory: Medial surface of frontal and parietal lobes - supplies the leg/foot area of the motor and sensory homunculi
- Occlusion: Contralateral leg weakness/sensory loss, urinary incontinence, abulia (if bilateral)
Middle Cerebral Artery (MCA)
- Turns laterally into the Sylvian fissure; divides into superior and inferior divisions
- Superior division: Cortex above Sylvian fissure - lateral frontal lobe, peri-Rolandic (face, arm motor/sensory)
- Inferior division: Cortex below Sylvian fissure - lateral temporal, parietal
- Territory: Most of the dorsolateral convexity - the largest territory of any cerebral artery
- Occlusion: Contralateral hemiplegia/hemisensory loss (face + arm > leg), homonymous hemianopia, aphasia (dominant hemisphere), neglect (non-dominant)
Posterior Cerebral Artery (PCA)
- Curves back from top of basilar, sweeps around the midbrain
- Territory: Inferior and medial temporal lobe, medial occipital lobe (visual cortex)
- Occlusion: Contralateral homonymous hemianopia (with macular sparing), visual agnosia, alexia without agraphia (left PCA), memory deficits (hippocampus)
Penetrating (Deep) Vessels Arising Near the Circle
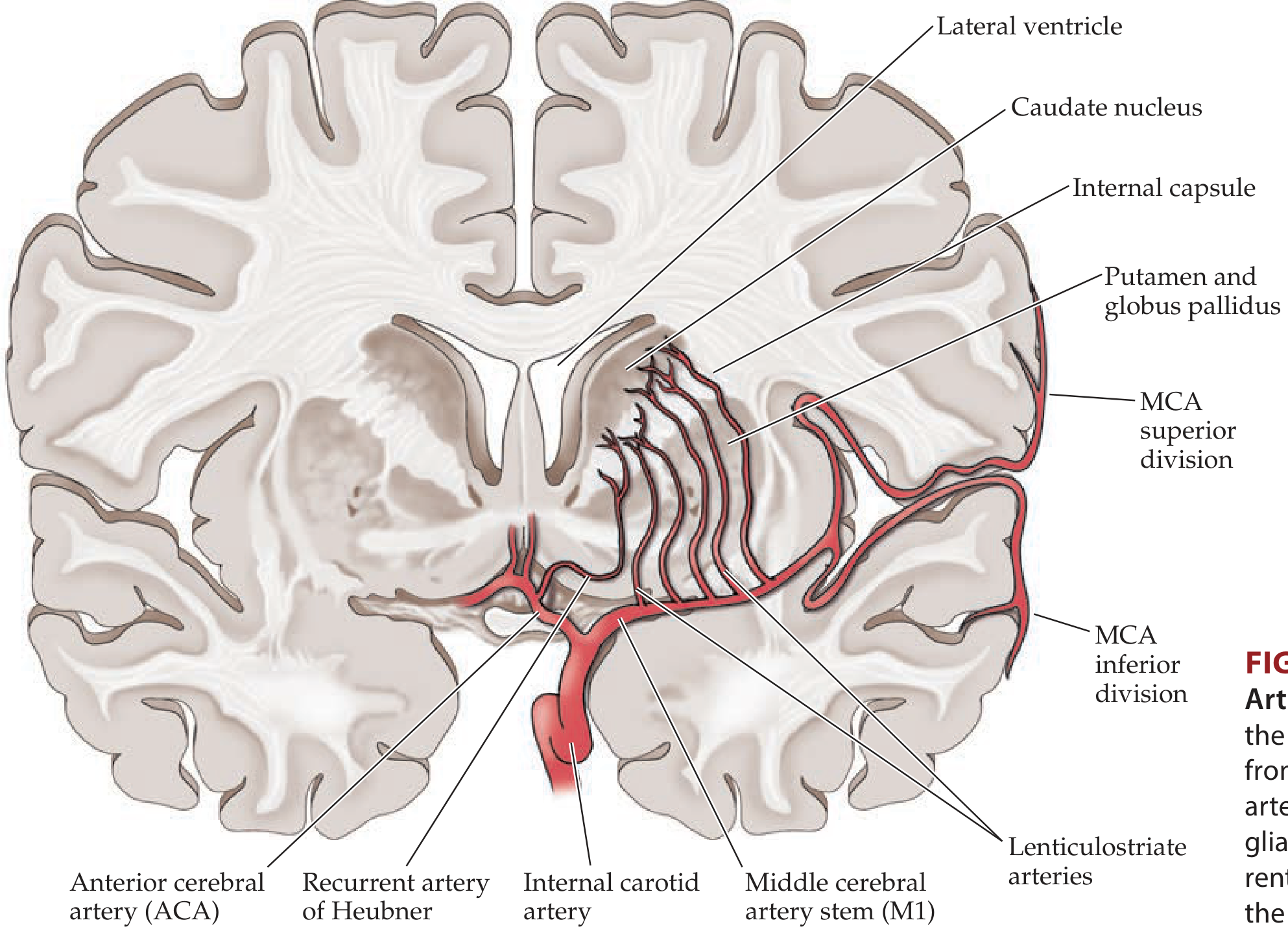
| Vessel | Origin | Territory |
|---|---|---|
| Lenticulostriate arteries | Proximal MCA (M1) | Basal ganglia (putamen, caudate), internal capsule |
| Anterior choroidal artery | ICA (just before bifurcation) | Globus pallidus, posterior limb of internal capsule, thalamus (part of lateral geniculate) |
| Recurrent artery of Heubner | Proximal ACA (A1/A2 junction) | Head of caudate, anterior putamen, anterior internal capsule |
| Thalamoperforator arteries | Proximal PCA / top of basilar | Thalamus, midbrain |
High-yield: The lenticulostriate arteries are "end arteries" with no collateral supply - they are especially prone to hypertensive damage (lacunar infarcts + hypertensive hemorrhage).
Branches of the Basilar Artery (Posterior Circulation)
| Branch | Territory | Syndrome if occluded |
|---|---|---|
| PICA (Posterior Inferior Cerebellar A.) | Lateral medulla + inferior cerebellum | Wallenberg syndrome |
| AICA (Anterior Inferior Cerebellar A.) | Lateral lower pons + anterior cerebellum | AICA syndrome (ipsilateral CN VII, VIII deficits) |
| SCA (Superior Cerebellar A.) | Superior cerebellum, dorsal pons | Cerebellar ataxia, CN IV palsy |
| Basilar perforators | Pons | Various pontine syndromes |
| PCA (terminal branch) | Occipital + medial temporal | Hemianopia, memory loss |
Clinical Significance - High-Yield for Exams
1. Berry (Saccular) Aneurysms
The most common sites of intracranial aneurysms, in order of frequency:
| Location | % of all aneurysms |
|---|---|
| AComm (anterior communicating artery) | ~35% - most common overall |
| PComm origin (ICA-PComm junction) | ~30% - causes CN III palsy (blown pupil) |
| MCA bifurcation | ~20% |
| Basilar tip | ~5% |
| Others | ~10% |
Rupture → subarachnoid hemorrhage ("thunderclap headache," worst headache of life)
2. Collateral Flow
The circle's function is to equalize pressure and provide collateral flow when one vessel is compromised. However, because a complete ring exists in only ~34%, many patients have inadequate collateral protection.
3. CN III Compression
A PComm aneurysm lies directly adjacent to CN III as it passes from the midbrain to the cavernous sinus. Expansion compresses CN III → ipsilateral pupil dilation (mydriasis), ptosis, and "down-and-out" eye = a neurosurgical emergency.
4. Anterior Choroidal Artery Occlusion
Produces the classic triad: contralateral hemiplegia + hemisensory loss + homonymous hemianopia (due to posterior limb of IC + lateral geniculate involvement) - mimics MCA stroke but without cortical signs.
Memory Mnemonics
Components of the Circle - "2 ICA, 2 ACA, 1 AComm, 2 PComm, 2 PCA"
ICA branches - OPAAM: Ophthalmic, Posterior communicating, Anterior choroidal, Anterior cerebral, Middle cerebral
Aneurysm sites (most to least common): "AComM Prefers Making Big Others wait" → AComm, PComm, MCA, Basilar, Others
Source: - Neuroanatomy through Clinical Cases 3rd Ed. - Medical Physiology (Boron & Boulpaep)
Concise it
Circle of Willis — Concise
What It Is
An anastomotic arterial ring at the base of the brain connecting the anterior (internal carotid) and posterior (vertebrobasilar) circulations. Provides collateral flow. Complete ring present in only ~34% of people.
9 Vessels That Form the Circle
| Vessel | Count |
|---|---|
| Internal carotid artery (ICA) | ×2 |
| Anterior cerebral artery - A1 segment (ACA) | ×2 |
| Anterior communicating artery (AComm) | ×1 |
| Posterior communicating artery (PComm) | ×2 |
| Posterior cerebral artery - P1 segment (PCA) | ×2 |
MCA does NOT form part of the circle - it exits laterally.
Simple Diagram
AComm
ACA ——+—— ACA
| |
ICA ICA
| |
PComm PComm
| |
PCA —basilar— PCA
ICA Branches Mnemonic — OPAAM
Ophthalmic → PComm → Anterior choroidal → ACA → MCA
3 Main Cerebral Artery Territories
| Artery | Territory | Occlusion = ? |
|---|---|---|
| ACA | Medial frontal + parietal | Contralateral leg weakness/sensory loss |
| MCA | Lateral convexity (largest territory) | Contralateral face + arm > leg, aphasia/neglect |
| PCA | Occipital + medial temporal | Homonymous hemianopia, memory loss |
Deep Penetrating Arteries (High-Yield)
| Artery | Origin | Supplies |
|---|---|---|
| Lenticulostriate | MCA (M1) | Basal ganglia, internal capsule |
| Anterior choroidal | ICA | Posterior limb IC, globus pallidus, thalamus |
| Recurrent artery of Heubner | ACA (A1/A2) | Head of caudate, anterior IC |
| Thalamoperforators | Basilar tip / PCA | Thalamus, midbrain |
Basilar Artery Branches
PICA → lateral medulla (Wallenberg)
AICA → lower pons + anterior cerebellum
SCA → superior cerebellum
PCA (terminal) → occipital + medial temporal
Berry Aneurysm Sites (Most → Least Common)
- AComm (~35%) - most common
- PComm (~30%) - compresses CN III (blown pupil)
- MCA bifurcation (~20%)
- Basilar tip (~5%)
Rupture → subarachnoid haemorrhage (thunderclap headache)
This is a shared conversation. Sign in to Orris to start your own chat.