Peripheral arterial occlusive disease
Reading File
Finding Sources
Searching PubMed
"peripheral arterial disease"[MeSH Terms] AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, rich information to deliver a thorough answer. Let me compile it.
Peripheral Arterial Occlusive Disease (PAOD)
Definition
Peripheral artery disease (PAD) / peripheral arterial occlusive disease is a clinical disorder characterized by stenosis or occlusion in the aorta or the arteries of the limbs, caused most commonly by atherosclerosis. Other causes include thromboembolism, vasculitis, fibromuscular dysplasia, entrapment syndromes, cystic adventitial disease, and trauma.
- Harrison's Principles of Internal Medicine 22e (2025)
Epidemiology and Risk Factors
- Peak prevalence in the sixth and seventh decades of life
- Prevalence is similar in men and women
- Higher prevalence in Black individuals than non-Hispanic white individuals
- Associated with lower socioeconomic status
Risk factors:
| Risk Factor | Notes |
|---|---|
| Cigarette smoking | Most powerful modifiable risk factor |
| Diabetes mellitus | Associated with distal disease |
| Hypercholesterolemia | Elevated LDL and lipoprotein(a) |
| Hypertension | |
| Renal insufficiency / CKD | |
| Homocysteinemia | |
| Age |
- Harrison's 22e; Fuster & Hurst's The Heart, 15e
Pathology
Segmental atherosclerotic lesions cause stenosis or occlusion in large and medium-sized vessels. The lesions consist of:
- Atherosclerotic plaques with calcium deposition
- Thinning of the media
- Patchy destruction of muscle and elastic fibers
- Fragmentation of the internal elastic lamina
- Platelet-fibrin thrombi
Primary sites of involvement:
- Abdominal aorta and iliac arteries - 30% of symptomatic patients
- Femoral and popliteal arteries - 80-90% of patients (most common; the superficial femoral artery accounts for ~70% of cases)
- Tibial and peroneal arteries - 40-50% of patients (more common in elderly and diabetics)
Lesions occur preferentially at arterial branch points where turbulence, altered shear stress, and intimal injury occur.
- Harrison's 22e
Clinical Presentation
Symptoms - Progressive Spectrum
1. Asymptomatic PAD
Fewer than 50% of patients with PAD are symptomatic; many have only slow or impaired gait.
2. Intermittent Claudication
- Pain, ache, cramp, numbness, or fatigue in muscles during exercise, relieved by rest (not by stopping and leaning - which distinguishes it from spinal stenosis/neurogenic claudication)
- Site of claudication is distal to the occlusive lesion:
- Aortoiliac disease: buttock, hip, thigh claudication + impotence = Leriche's syndrome
- Femoral-popliteal disease: calf claudication (most common)
- Tibial/peroneal disease: calf and foot claudication
3. Chronic Limb-Threatening Ischemia (CLTI)
- Rest pain: Worse at night, improved by hanging foot out of bed or sleeping in a chair (gravity restores perfusion pressure). Even the weight of bedclothes exacerbates it.
- Ischemic ulcers: Painful erosions between toes or shallow non-healing ulcers on the dorsum of the feet, shins, and malleoli
- Gangrene: Blackened, mummified tissue; superadded infection makes it "wet"
4. Acute Limb Ischemia ("6 Ps")
- Pain (severe, sudden onset)
- Pallor
- Pulselessness
- Paresthesia
- Paralysis
- Perishing cold (poikilothermia)
Paralysis and paresthesia are the most ominous findings, indicating neurological involvement and threatening limb viability.
- Harrison's 22e; Bailey & Love's Short Practice of Surgery, 28e
Physical Examination
| Finding | Significance |
|---|---|
| Absent/decreased pulses distal to obstruction | Key diagnostic sign |
| Bruits over narrowed artery | Turbulent flow through stenosis |
| Muscle atrophy | Chronic ischemia |
| Hair loss, thickened nails, shiny skin | Chronic ischemia |
| Reduced skin temperature, pallor, cyanosis | Reduced perfusion |
| Elevation pallor → dependent rubor | Buerger's test; rubor = reactive hyperemia |
| Venous guttering on elevation | Severely reduced venous filling pressure |
| Ischemic ulcers / gangrene | CLTI |
A chronically ischemic limb may feel relatively warm (equilibrates to ambient temperature) - in contrast to an acutely ischemic limb which is cold. A dependent chronically ischemic foot may appear red and swollen, mimicking cellulitis, but elevation reveals pallor and venous guttering.
- Bailey & Love's, 28e
Classification
Fontaine Classification (Symptom-Based)
| Stage | Description |
|---|---|
| I | Asymptomatic |
| IIa | Claudication >200 m |
| IIb | Claudication <200 m |
| III | Rest pain |
| IV | Ulceration/gangrene |
Rutherford Classification
| Grade | Category | Description |
|---|---|---|
| 0 | 0 | Asymptomatic |
| I | 1 | Mild claudication |
| I | 2 | Moderate claudication |
| I | 3 | Severe claudication |
| II | 4 | Ischemic rest pain |
| III | 5 | Minor tissue loss |
| III | 6 | Major tissue loss |
Anatomic Classification
-
TASC II (Trans-Atlantic Inter-Society Consensus): classifies lesions A-D based on extent; guides endovascular vs. surgical approach
-
GLASS (Global Limb Anatomic Staging System): newer system for CLTI
-
Fuster & Hurst's The Heart, 15e
Investigation
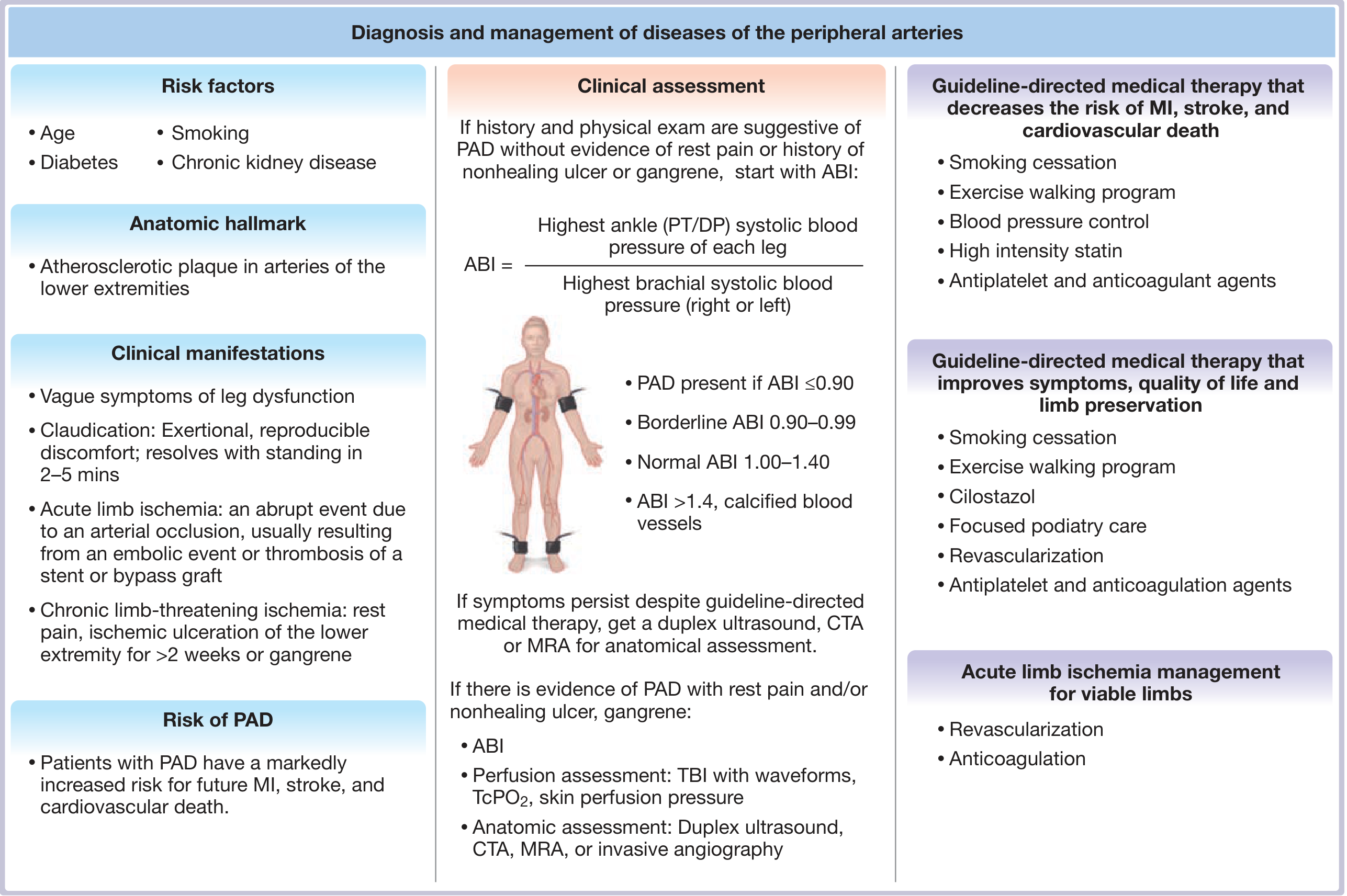
Ankle-Brachial Index (ABI)
The cornerstone non-invasive test. Measured with a Doppler probe and sphygmomanometer:
ABI = Highest ankle (PT or DP) systolic BP / Highest brachial systolic BP
| ABI Value | Interpretation |
|---|---|
| >1.40 | Non-compressible (calcified) vessels - false normal |
| 1.00-1.40 | Normal |
| 0.90-0.99 | Borderline |
| ≤0.90 | PAD (diagnostic) |
| 0.40-0.70 | Claudication typical range |
| <0.40 | Severe ischemia / rest pain |
When the ABI is >1.40 (calcified, incompressible vessels - common in diabetes), the toe-brachial index (TBI) is used (TBI <0.70 = PAD). Digit arteries are less prone to calcification.
Exercise ABI testing can unmask disease in patients with borderline resting ABI.
Vascular Laboratory / Imaging
| Test | Role |
|---|---|
| Hand-held Doppler | Detects flow; triphasic > biphasic > monophasic waveforms indicate increasing severity |
| Duplex ultrasound (DUS) | Provides anatomy + flow assessment; as accurate as angiography in experienced hands; limited in calcified/obese patients |
| CT angiography (CTA) | Excellent anatomic detail; widely available; uses iodinated contrast |
| MR angiography (MRA) | No radiation; good soft tissue contrast; limited in stented segments |
| Digital subtraction angiography (DSA) | Gold standard; reserved for when intervention is planned; Seldinger technique via CFA; up to 5% procedural complication rate |
| TcPO2 / Skin perfusion pressure | Used in CLTI for wound healing prediction |
General blood tests: FBC, blood glucose/HbA1c, lipid profile, renal function (U&E/creatinine), ECG. Co-morbid coronary (50%) and cerebrovascular (25-50%) disease is common.
- Harrison's 22e; Bailey & Love's, 28e
Treatment
1. Risk Factor Modification (for Cardiovascular Risk Reduction)
- Smoking cessation: Single most important intervention. Use counseling + NRT/bupropion/varenicline.
- Statins (high-intensity): Mandatory in all PAD patients. Aim for ≥50% LDL reduction (2018 AHA/ACC guideline). Also reduce adverse limb events including amputation.
- PCSK9 inhibitors: If target not reached on statin; also reduce limb events.
- Antihypertensives: ACE inhibitors/ARBs preferred (reduce cardiovascular events). Beta-blockers do not worsen claudication and can be used for coexisting CAD.
- Glycemic control: Intensive glucose lowering reduces amputation risk. GLP-1 agonists and SGLT2 inhibitors have additional cardiovascular and limb benefits in diabetic PAD patients.
2. Antiplatelet / Antithrombotic Therapy
- Antiplatelet therapy (aspirin or clopidogrel): Recommended for all symptomatic PAD patients.
- Clopidogrel vs. aspirin: Outcomes are similar; clopidogrel is an acceptable first-line choice.
- Dual antiplatelet therapy (DAPT): Benefit over monotherapy in PAD uncertain; increased bleeding risk.
- Vorapaxar (PAR-1 antagonist): Reduces cardiovascular events and acute limb ischemia when added to existing antiplatelet therapy, but increases bleeding.
- Rivaroxaban 2.5 mg BD + aspirin: The COMPASS regimen - improves cardiovascular and limb outcomes in established PAD and after revascularization, but increases bleeding risk.
- Warfarin is not indicated for chronic PAD (no benefit over antiplatelet, more bleeding).
3. Claudication-Specific Therapies
- Supervised exercise training: 30-45 min sessions, ≥3 times/week for ≥12 weeks. Improves walking distance - often equivalent to or better than revascularization for claudication.
- Cilostazol (PDE-3 inhibitor): Increases walking distance by ~50%. Contraindicated in heart failure.
- Foot care: moisturizing creams, well-fitting protective shoes. Avoid elastic compression hose (reduces arterial flow).
4. CLTI-Specific Supportive Measures
- Bed elevation via shock blocks under the bed head (increases gravitational perfusion pressure)
- Bed canopy over the feet (protects from bedcloth pressure)
5. Revascularization
Endovascular:
- Percutaneous transluminal angioplasty (PTA) ± stenting
- Drug-eluting balloons / stents
- TASC A & B lesions generally amenable to endovascular approach
- Caution: paclitaxel-coated devices raised mortality signal in meta-analyses
Surgical:
- Bypass grafting (aortofemoral, femoropopliteal, femorodistal)
- Autologous vein graft preferred for infrapopliteal bypass (better long-term patency)
- Endarterectomy (for focal iliac/common femoral disease)
- TASC C & D lesions typically require surgery
- Open surgery preferred when rapid flow restoration (<24 h) is necessary to prevent limb loss
Decision framework: Endovascular procedures carry lower periprocedural risk but may have lower long-term durability; open surgery has higher upfront risk but more durable results. Patient fitness, anatomy, and limb threat severity guide the choice.
- Harrison's 22e; Fuster & Hurst's, 15e; Bailey & Love's, 28e
Acute Limb Ischemia - Management
Causes: Embolism (AF, valvular disease, mural thrombus) vs. acute thrombosis on existing atherosclerosis vs. graft/stent occlusion.
Immediate:
- IV heparin anticoagulation to prevent clot propagation and re-embolism
- Confirm diagnosis with Doppler, duplex US, CTA, MRA or catheter arteriography
Revascularization options (for viable limbs):
- Catheter-directed thrombolysis (rt-PA, reteplase, tenecteplase): Most effective for acute thrombus in atherosclerotic vessels, grafts, or stents; when surgery is contraindicated; for distal inaccessible vessels. Requires intensive monitoring for hemorrhage.
- Percutaneous mechanical thrombectomy: Uses hydrodynamic or rotational devices; usually combined with pharmacologic thrombolysis.
- Surgical thromboembolectomy / bypass: Preferred when flow must be restored within 24 hours to prevent limb loss.
- Amputation: For non-viable limb (loss of sensation, paralysis, no Doppler flow in arteries or veins).
Long-term: Anticoagulation (warfarin/NOAC) when caused by cardiac thromboembolism. Source treatment for prosthetic valves, infective endocarditis, or atrial myxoma.
- Harrison's 22e
Systemic Risk and Prognosis
PAD is a marker of systemic atherosclerosis. Patients have markedly increased risk of:
- Myocardial infarction (50% have coexisting coronary disease)
- Stroke (25-50% have coexisting cerebrovascular disease)
- Cardiovascular death
5-year cardiovascular mortality in symptomatic PAD is approximately 30%. The limb prognosis in claudicants is relatively benign (only ~1-2% per year progress to major amputation with optimal medical therapy), but the cardiovascular prognosis is serious.
Sources
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapter 292
- Fuster & Hurst's The Heart, 15th Edition - Chapter 26
- Bailey & Love's Short Practice of Surgery, 28th Edition - Chapter 61
- Recent PubMed evidence: Toe-brachial index meta-analysis [PMID: 39474992, Cochrane 2024]; TG-glucose index and PAD meta-analysis [PMID: 39341836, 2024]
Purely , only and only as per sabiston 22 edition
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have the full chapter outline and substantial content. I have all the essential information from Sabiston's PAD chapter (Chapter 103). Let me compile the comprehensive response now.
Peripheral Arterial Occlusive Disease
As per Sabiston Textbook of Surgery (The Biological Basis of Modern Surgical Practice)
Chapter 103 - Authors: Elizabeth G. King, Katharine L. McGinigle, and Alik Farber
Overview and Pathophysiology
PAD in the lower extremities is caused by atherosclerotic plaque reducing oxygenated arterial flow, leading to ischemia. The fundamental mechanism involves progressive atherosclerosis narrowing the lumen of the aorta and lower extremity arteries, reducing perfusion to the tissues distally.
Anatomic patterns of atherosclerotic disease:
- Aortoiliac occlusive disease (AIOD)
- Femoropopliteal disease (most common segment)
- Infrapopliteal / tibial disease (more common in diabetics and elderly)
Epidemiology and Risk Factors
- Prevalence has increased with the aging population, rising obesity rates, and as a complication of diabetes mellitus (DM)
- Many patients are asymptomatic; approximately 10% of patients with PAD have intermittent claudication
- Of all PAD patients with intermittent claudication, about 21% will have progression of disease over 5 years, with an amputation rate of approximately 1%
- Patients with both PAD and DM have a lower extremity amputation rate of 5%, vs. 1.5% for non-diabetic PAD patients
- Minor amputations are 4.6 times more likely in patients with both diagnoses vs. PAD alone
- A twofold increased risk of minor amputations if baseline HbA1c >7%
Risk factors:
- Diabetes mellitus
- Smoking / tobacco use
- Hypertension
- Hyperlipidemia
- Chronic kidney disease
- Obesity
- Age
Cardiovascular co-morbidity burden:
- Patients with PAD and concomitant CAD have higher composite MACE rates (15.3% vs. 8.9%; HR 1.50)
- Patients with prior MI and PAD have double the cardiovascular risk compared to PAD alone (19.3% vs. 8.4%)
Clinical Presentation
Spectrum of Disease
1. Asymptomatic PAD
Most patients are asymptomatic. Detected incidentally or via screening (ABI measurement).
2. Intermittent Claudication (IC)
- Defined as pain, fatigue, or numbness in the lower extremities with activity that is relieved by rest
- About 10% of all PAD patients have IC
- 5-year risk of limb amputation is 5% and predicted 5-year life expectancy is 75-80% (relatively preserved)
- The majority of patients with IC will maintain current function or decline slowly
3. Chronic Limb-Threatening Ischemia (CLTI)
- Defined as arterial occlusive disease causing greater than 2 weeks of symptoms of rest pain or tissue loss with diagnostic study findings confirming arterial insufficiency
- CLTI is an advanced progression of PAD that may lead to minor or major amputation if left untreated
- Less than 5% of patients with PAD progress to CLTI
- A systematic review showed a major amputation rate of 22% if CLTI is left untreated
- Patients with CLTI have 50% 5-year mortality and a much higher amputation risk (compared to IC)
4. Acute Limb Ischemia (ALI)
- Defined as an arterial occlusion with associated symptoms present for less than 2 weeks
- A surgical emergency; irreversible muscle and nerve injury can occur after 6 hours of severe arterial insufficiency
- Incidence: approximately 1.5 cases per 10,000 persons per year
- Associated with high morbidity and mortality: perioperative mortality rates 20-40%, limb loss rates 12-50%
The "Six Ps" of Acute Limb Ischemia
- Pain
- Pulselessness
- Poikilothermia (coolness)
- Paresthesia
- Pallor
- Paralysis
The severity varies based on the duration of occlusion, the location, and the extent of collateral circulation.
Classification Systems
Fontaine Classification (Historical - clinical symptoms only)
| Stage | Description |
|---|---|
| I | Asymptomatic |
| IIa | Claudication >200 m |
| IIb | Claudication <200 m |
| III | Rest pain |
| IV | Ulceration / gangrene |
Rutherford Classification (Clinical symptoms + noninvasive data; separates chronic and acute)
For Chronic PAD:
| Grade | Category | Description |
|---|---|---|
| 0 | 0 | Asymptomatic |
| I | 1 | Mild claudication |
| I | 2 | Moderate claudication |
| I | 3 | Severe claudication |
| II | 4 | Ischemic rest pain |
| III | 5 | Minor tissue loss |
| III | 6 | Major tissue loss |
Rutherford Classification of Acute Limb Ischemia (Table 103.4):
| Category | Description/Prognosis | Sensory Loss | Muscle Weakness | Arterial Doppler | Venous Doppler |
|---|---|---|---|---|---|
| I. Viable | Not immediately threatened | None | None | Audible | Audible |
| IIa. Marginally threatened | Salvageable if promptly treated | Minimal (toes) / none | None | Absent | Audible |
| IIb. Immediately threatened | Salvageable with immediate revascularization | More than toes, rest pain | Mild-moderate | Absent | Audible |
| III. Irreversible | Major tissue loss or permanent neurologic damage | Profound, anesthetic | Profound paralysis (rigors) | Absent | Absent |
Key principle from Sabiston: Irreversibly ischemic limbs (Category III) with major tissue loss or permanent nerve damage with profound sensory/motor loss should be treated with primary extremity amputation. Revascularization of a nonviable extremity in rigor should be avoided as it could lead to multisystem organ failure and death.
SVS WIfI Classification (Wound, Ischemia, Foot Infection) - Table 103.1
A modern system for CLTI that guides limb salvageability and revascularization strategy:
Wound (W) - Grades 0-3:
| Grade | Ulcer | Gangrene |
|---|---|---|
| 0 | No ulcer | No gangrene (ischemic rest pain only) |
| 1 | Small, shallow ulcer on distal leg/foot; no exposed bone (except distal phalanx) | No gangrene |
| 2 | Deeper ulcer with exposed bone, joint, or tendon; shallow heel ulcer without calcaneal involvement | Gangrenous changes limited to digits |
| 3 | Extensive, deep ulcer involving forefoot | Extensive gangrene of forefoot and/or midfoot; full-thickness heel necrosis ± calcaneal involvement |
Ischemia (I) - Grades 0-3:
| Grade | ABI | Ankle Systolic Pressure | TP / TcPO₂ |
|---|---|---|---|
| 0 | ≥0.80 | >100 mmHg | ≥60 mmHg |
| 1 | 0.60-0.79 | 70-100 mmHg | 40-59 mmHg |
| 2 | 0.40-0.59 | 50-70 mmHg | 30-39 mmHg |
| 3 | ≤0.39 | <50 mmHg | <30 mmHg |
Foot Infection (fI) is the third component.
TASC II Classification (Anatomic - guides endovascular vs. surgical approach)
- Published 2000, modified 2007
- Divides lesions into aortoiliac and femoropopliteal segments
- Groups lesion patterns by severity (A to D):
- TASC A & B: Focal/limited disease → endovascular therapy recommended
- TASC C & D: Longer, more severe lesions → surgical bypass recommended
GLASS (Global Limb Anatomic Staging System)
- Newer anatomic classification for CLTI, used with WIfI to guide revascularization strategy
- The GLASS stage (y-axis) combined with WIfI limb risk (x-axis) determines preferred initial revascularization strategy
Diagnostic Modalities
Noninvasive Vascular Studies
Ankle-Brachial Index (ABI)
- Cornerstone non-invasive test
- ABI = Highest ankle systolic BP (posterior tibial or dorsalis pedis) / Highest brachial systolic BP
- ABI ≤0.90 = PAD (diagnostic)
- In CLTI:
- Ischemia Grade 0: ABI ≥0.80
- Grade 1: ABI 0.60-0.79
- Grade 2: ABI 0.40-0.59
- Grade 3: ABI ≤0.39
- When vessels are calcified and non-compressible (ABI >1.40, common in diabetes): use toe pressure (TP) or transcutaneous oxygen pressure (TcPO₂)
Imaging
Duplex Sonography (Duplex Ultrasound)
- Non-invasive; good for femoropopliteal segments
- Operator-dependent; limited in calcified/obese patients
- Can image slow flow (2 cm/s) in infrapopliteal vessels
Computed Tomography Angiography (CTA)
- Excellent for aortoiliac disease; useful for operative planning
- Limited in distal, calcified lower extremity vessels (calcification creates artifact impairing stenosis characterization)
- Advances: dual-energy CTA with bone removal protocols, ultra-high-resolution CT with subtraction techniques are improving assessment
Magnetic Resonance Angiography (MRA)
- Most accurate in meta-analysis comparing contrast-enhanced MRA, duplex, and CTA for lesions with >50% stenosis
- Avoids ionizing radiation; longer acquisition times
- Ability to image blood flow as slow as 2 cm/s - improves imaging of infrapopliteal vessels and identifies bypass targets not seen on DSA (especially in diabetics)
- Emerging techniques: plaque composition assessment, skeletal muscle perfusion, non-contrast methods
Digital Subtraction Angiography (DSA)
- Fluoroscopic technique; intraarterial contrast injection with subtracted images
- Invasive; carries risk of complications
- Key advantage: concurrent therapeutic endovascular intervention at time of imaging
- Intravascular ultrasound (IVUS) can be used as an adjunct during angiography to measure arterial dimensions for balloon/stent sizing and to assess post-intervention results
Non-Interventional (Medical) Management
The noninterventional management of PAD is critically important. Goals:
- Prevent progressive atherosclerosis - reduce Major Adverse Cardiovascular Events (MACEs) (nonfatal stroke + nonfatal MI + cardiovascular death)
- Medically optimize patients before revascularization (better surgical outcomes)
- After revascularization: reduce Major Adverse Limb Events (MALEs) (reinterventions, amputations)
Antithrombotic Therapy
- Multiple RCTs have demonstrated benefit of single antiplatelet therapy for secondary prevention (reduce MI, stroke, death) in PAD
- In asymptomatic PAD: conflicting data for primary prevention (no coexisting CAD/CVD); single antiplatelet may be reasonable in those with reduced ABI and low bleeding risk
- 2022 USPSTF guidance: recommended against initiating aspirin for primary prevention of MACE in the general adult population (ages 40-59: only small net benefit for those with ≥10% 10-year CVD risk; ages ≥60: recommends against)
- Note: USPSTF guidance was for primary prevention - PAD patients with established atherosclerosis are candidates for secondary prevention
Smoking Cessation
The single most important modifiable risk factor. Part of mandatory risk factor modification.
Exercise Therapy
- Supervised exercise therapy is the preferred initial management strategy for IC (along with optimal medical management)
- A systematic review of 10 RCTs (1087 patients) found endovascular revascularization did not provide significant benefit compared to supervised exercise alone for functional performance or quality-of-life
- Exception (CLEVER Trial): In IC secondary to aortoiliac disease, both supervised exercise AND endovascular revascularization improved functional status and quality of life
Treatment of Asymptomatic Disease and Intermittent Claudication
- SVS guidelines: Recommend against invasive treatments for PAD in asymptomatic patients, regardless of hemodynamic measures or imaging findings (in the absence of a threatened bypass graft or stent)
- Cornerstone = lifestyle change + medical therapy to address cardiovascular risk factors
- IC patients are at relatively low risk of adverse outcomes (5-year amputation risk 5%; 5-year life expectancy 75-80%)
- 20-30% of IC patients will develop disability significant enough to warrant intervention
- Indications for intervention in IC (SVS Appropriate Use Criteria 2022):
- Lifestyle-altering symptoms
- After failure of exercise and medical therapy
- Favorable anatomic factors
- Prolonged patency and symptom relief likely
- For femoropopliteal disease: reserve invasive interventions for severe, lifestyle-limiting IC
- For common femoral artery (CFA) disease: open endarterectomy provides greater net benefit than endovascular intervention
- Tibial artery interventions for IC: of unclear benefit; can lead to worsening of PAD and increased risk of limb loss - not recommended
Treatment of Chronic Limb-Threatening Ischemia (CLTI)
- CLTI patients have 50% 5-year mortality and much higher amputation risk than IC patients
- Prognosis determined primarily by limb stage at presentation
Selection of Revascularization Strategy
Aortoiliac Occlusive Disease (AIOD):
- TASC II (2007): Open bypass recommended for TASC C and D (longer, severe lesions); endovascular for TASC A and B
- Note: TASC classifications did not correlate well with expected patency rates (limitation acknowledged)
Infrainguinal Disease:
Three landmark RCTs guide evidence-based treatment in CLI:
- BASIL Trial (2005): Bypass Versus Angioplasty in Severe Ischaemia of the Leg - randomized, controlled, multicenter; established foundation for decision-making in infrainguinal CLTI
- Preferred strategy for infrainguinal disease is determined by GLASS anatomic stage (y-axis) vs. WIfI limb risk (x-axis) (Figure 103.12)
Open Surgical Revascularization
Inflow Bypass Techniques (Aortoiliac):
- Aortofemoral bypass (standard for AIOD)
- End-to-end or end-to-side proximal anastomosis; graft beveled 60 degrees
- Profundaplasty: when DFA and SFA are diseased; preserves long-term patency of anatomic and extraanatomic grafts
- Patent IMA or accessory renal arteries may be reimplanted
Extraanatomic Inflow Bypass:
- Used in high-risk patients or hostile abdomen
Infrainguinal Bypass Techniques:
- Autologous vein is preferred conduit for infrapopliteal bypass
- Femoral triangle anatomy is key: CFA lies lateral to the common femoral vein; DFA exits posterolaterally; great saphenous vein enters anteromedially
- Common femoral artery (CFA) endarterectomy: open surgery preferred for CFA disease
Endovascular Techniques
- Percutaneous transluminal angioplasty (PTA) ± stenting
- Drug-eluting balloons and stents
- For aortoiliac: endovascular approach for TASC A/B lesions
Acute Limb Ischemia - Management
Etiology: Embolism vs. Thrombosis (most common causes)
- Other causes: traumatic injury, aortic dissection, hemodynamic compromise (shock, vasopressors)
Initial management:
- Systemic anticoagulation (prefer agents that allow titration and quick reversal)
- CTA may be the fastest diagnostic tool to guide the operative approach
- Additional diagnostics: echocardiogram (identify embolic sources), aortic cross-sectional imaging, full pulse exam + Doppler, percutaneous arteriography, MRA
Revascularization options:
- Endovascular, open, or hybrid based on anatomy and urgency
- Time to therapy is critical for preserving limb tissue and function
Fasciotomy:
- Four-compartment fasciotomy of the lower extremity should always be considered after revascularization, especially if ischemia time >6 hours
Amputation:
- Category III (Irreversible) ALI → primary amputation (avoid revascularization of nonviable limb in rigor - risk of multisystem organ failure and death)
- Primary amputation also best for patients with poor overall health, devastating tissue loss especially with non-ambulatory status
- Determining the appropriate amputation level requires: full pulse examination + Doppler ultrasonography, CTA, arterial ultrasound, percutaneous arteriography, or MRA
Post-Revascularization
- Specific antithrombotic therapies reduce MALEs (reinterventions and amputations) after revascularization
- Postrevascularization surveillance programs are important for graft patency monitoring
- Assessment of outcomes includes patency rates, limb salvage, and quality-of-life metrics
Source: Sabiston Textbook of Surgery - The Biological Basis of Modern Surgical Practice, Chapter 103 (pages 2307-2409). Authors: Elizabeth G. King, Katharine L. McGinigle, and Alik Farber.
This is a shared conversation. Sign in to Orris to start your own chat.