Randomized clinical trials for psm exam from park,full explanation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed. Here is the full, exam-focused explanation from Park's Textbook of Preventive and Social Medicine.
Randomized Controlled Trials (RCT) - Park's PSM
What is an RCT?
An RCT is an epidemiologic experiment - the gold standard (No. 1 method) for evaluating new programmes or therapies. It is a type of experimental study in which participants are randomly allocated to either a study (experimental) group or a control group, to test the effect of an intervention.
Since its introduction, the RCT has questioned widely used treatments such as:
- Oral hypoglycaemic agents
- Varicose vein stripping
- Tonsillectomy
- Hospitalization of all MI patients
- Multiphasic screening
Design of an RCT (Fig. 9 from Park)
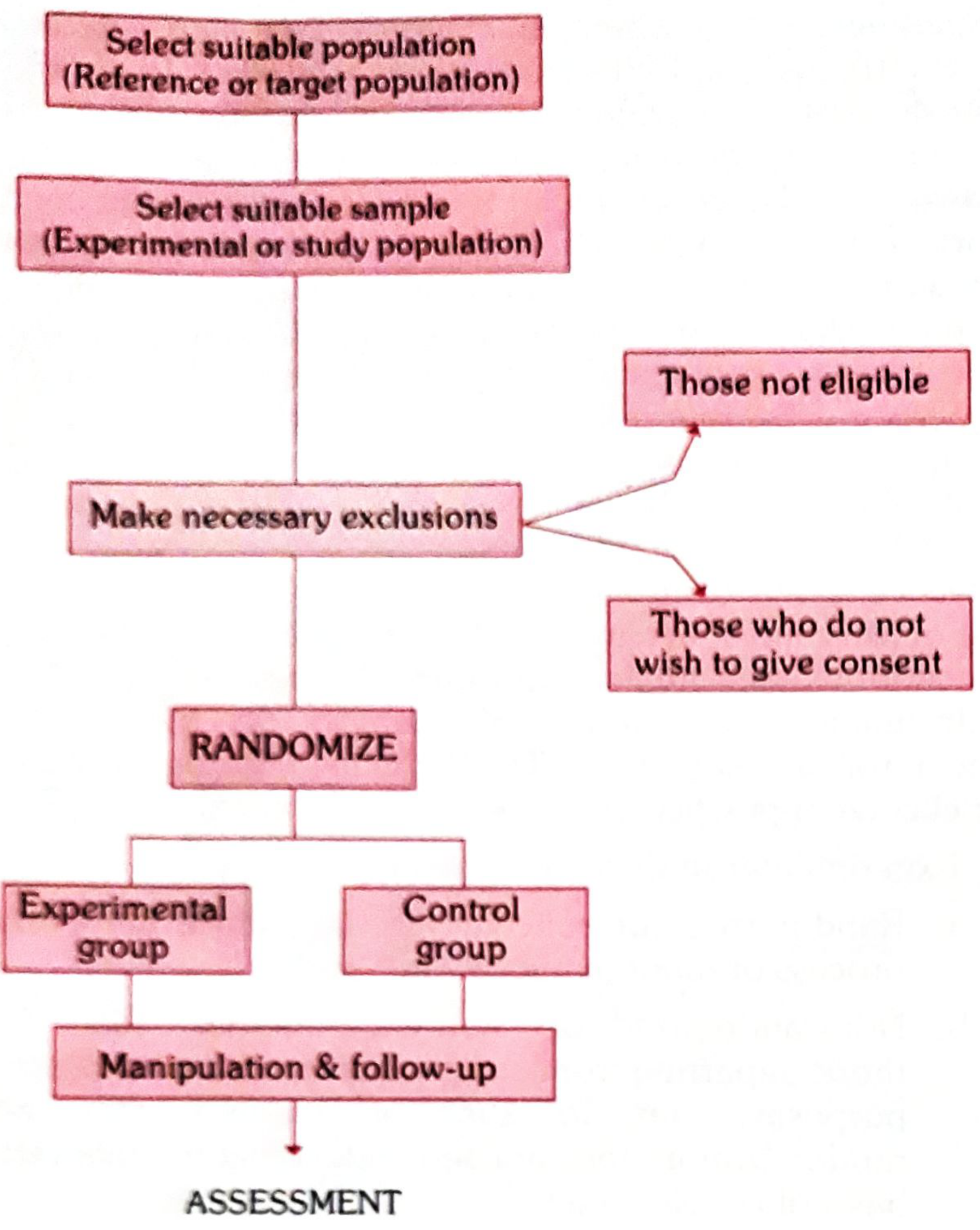
The basic steps are:
- Drawing up a Protocol
- Selecting Reference and Experimental populations
- Randomization
- Manipulation (Intervention)
- Follow-up
- Assessment of outcome
Step 1: The Protocol
- Specifies aims, objectives, questions to be answered
- Criteria for selection of study and control groups
- Sample size, procedures for allocation, treatments to be applied
- Standardization of procedures and schedules
- Responsibilities of all parties involved
- Essential especially in multi-centre trials
- Must be strictly adhered to throughout the study
- Purpose: to prevent bias and reduce sources of error
Pilot studies (preliminary test runs) may be done to test feasibility, operational efficiency, and to detect flaws before the final protocol is agreed upon.
Step 2: Selecting Reference and Experimental Populations
| Term | Definition |
|---|---|
| Reference (Target) population | The population to which findings will be applicable if the trial is successful. Can be broad (all of mankind) or limited (school children, obstetric population, industrial workers, etc.) |
| Experimental (Study) population | Derived from the reference population; the actual participants. Ideally randomly chosen from the reference population. |
Criteria for participants (volunteers):
- Must give informed consent - agree after being fully informed of purpose, procedures, and possible dangers
- Should be representative of the reference population
- Must be eligible/qualified - e.g., must be anaemic if testing an anti-anaemia drug; must be susceptible (non-immune) if testing a vaccine
A stable population whose cooperation is assured should be chosen to minimize losses to follow-up.
Step 3: Randomization
Definition: A statistical procedure by which participants are allocated into groups (study and control) to receive or not receive an experimental intervention.
Purpose:
- Eliminates selection bias
- Allows comparability - "like compared with like"
- Distributes known and unknown confounding factors equally between groups
- The investigator has no control over who goes into which group
"Randomization is the heart of a controlled trial." - Park
- Randomization ensures every individual gets an equal chance of being placed in either group
- Done only after the participant has entered the study (after qualifying and giving informed consent)
- Best done using a table of random numbers
- If variables like age/sex could affect outcome, the population is stratified into subgroups, then randomized within each subgroup
Key distinction: In analytical studies, there is NO randomization (groups are already differentiated as diseased/non-diseased). Comparability in analytical studies is achieved only by matching.
Step 4: Manipulation (Intervention)
- The experimental group receives the intervention (drug, vaccine, dietary component, habit modification, new procedure)
- This creates an independent variable (the intervention)
- The outcome (e.g., incidence of disease, survival time, recovery period) is the dependent variable
Step 5: Follow-up
- Both groups examined at defined intervals in a standard manner with equal intensity under the same circumstances
- Duration based on when a significant difference (e.g., mortality) is expected to be demonstrable
- Some losses to follow-up (attrition) are inevitable - due to death, migration, loss of interest
- Substantial attrition makes it difficult to generalise results
Step 6: Assessment of Outcome
Results compared as:
- Positive results: Benefits - reduced incidence/severity of disease, reduced cost
- Negative results: Side-effects, complications, deaths
Differences tested for statistical significance.
Sources of Bias in Assessment:
| Type of Bias | Who is Biased | Also Called |
|---|---|---|
| Subject variation | Participant - feels better knowing they received new treatment | Placebo effect |
| Observer bias | Investigator - influenced knowing which group the patient is in | Ascertainment bias |
| Evaluation bias | Investigator - subconsciously gives favourable outcome report | - |
Randomization and sample size cannot guard against these biases. The solution is blinding.
Blinding
| Type | Who is Blinded |
|---|---|
| Single blind | Participant only does not know group allocation |
| Double blind | Neither the doctor nor the participant knows group allocation - most frequently used |
| Triple blind | Participant + investigator + data analyst are all blind - ideal but rare |
When outcome is death, blinding is not essential.
Study Designs in RCTs
1. Concurrent Parallel Study Design
- Two randomly assigned groups: one gets treatment, other does not
- Patients remain in their assigned group for the entire duration
- Standard RCT design
2. Cross-over Study Design
- Each patient serves as his own control
- Group A gets treatment, Group B gets placebo - then they switch after a washout period
- Washout period allows elimination of drug ("carry-over effects")
Advantages of cross-over:
- All patients receive the new therapy at some point
- Requires fewer patients
Disadvantages - NOT suitable when:
- The drug cures the disease (nothing left to cross over with)
- Drug effective only during a certain stage of disease
- Disease changes radically during the study period
Types of Randomized Controlled Trials
1. Clinical Trials
- Evaluate therapeutic agents, mainly drugs
- Examples:
- Beta-blockers in reducing cardiovascular mortality post-MI
- Folate supplementation to prevent recurrence of neural tube defects
- Aspirin on cardiovascular mortality
- Beta-carotene on cancer incidence
- Efficacy of tonsillectomy for recurrent throat infection
- Coronary bypass surgery for prevention of MI
- Not all clinical trials can be blinded (e.g., tonsillectomy - surgical vs. non-surgical is obvious)
2. Preventive Trials
- Test primary preventive measures - vaccines and chemoprophylactic drugs
- Classic example: 1946 MRC UK trial of whooping cough vaccine
- May require application to groups rather than individuals
3. Risk Factor Trials
- Test whether elimination of a suspected risk factor reduces disease incidence
- E.g., dietary fat reduction and coronary artery disease
- More difficult - risk factors are deeply ingrained habits
4. Cessation Experiments
- Withdrawal of a harmful agent already in use
- Classic example: Retrolental fibroplasia (RLF) - RLF was caused by high oxygen concentrations given to premature infants. A controlled trial confirmed oxygen was the cause; withdrawing it led to a dramatic fall in RLF incidence (see the graph showing peak in 1952-53, then sharp drop after 1953)
5. Caesarian (Natural) Experiments / Unplanned Experiments
- Evaluating effects of naturally occurring "experiments"
- Since most diseases are fatal/disabling, deliberate human experiments to confirm aetiology are rarely possible
6. Evaluation of Health Services
- Assessing effectiveness and efficiency of health care delivery systems
- Classic Indian example: Controlled trials in chemotherapy of tuberculosis in India - demonstrated that domiciliary (home) treatment of pulmonary TB was as effective as costlier hospital/sanatorium treatment - ushered in the era of domiciliary treatment
- South-East London multiphasic screening trial - led to withholding vast resources for national multiphasic screening in UK
- Studies showing nurses and paramedical workers can perform tasks traditionally done by physicians = health services research
Non-Randomized (Non-Experimental) Trials
When RCTs are not possible:
- Ethical reasons (e.g., smoking and lung cancer - cannot deliberately expose people)
- Some preventive measures applicable only on community-wide basis (e.g., water fluoridation)
- Disease frequency is low and natural history is long (e.g., cancer cervix) - requires thousands of people for a decade or more - cost prohibitive
Types of Non-Randomized Trials:
- Uncontrolled trials - no comparison group (e.g., Pap smear/cervical cancer screening introduced in 1920s without RCT; evidence built from over a dozen uncontrolled studies)
- Historical controls - compare with past data
- Community trials - intervention applied to entire community
In non-randomized trials: no randomization → low comparability → higher chance of spurious result. Validity of causal inference is largely a matter of extra-statistical judgement.
Advantages of RCTs
- Randomization ensures comparability between groups (controls for both known and unknown confounders)
- Blinding reduces observer and subject bias
- Prospective design - allows direct measurement of incidence and causal inference
- Results can be analysed for statistical significance
- Gold standard for evaluating new therapies and preventive measures
Limitations/Disadvantages of RCTs
- Ethical issues - cannot withhold proven treatment or expose to harm
- Expensive and time-consuming
- Difficult to maintain blinding for surgical or behavioural interventions
- Attrition (drop-outs) can compromise results
- Results may not be generalizable if study population differs from reference population
- Volunteer bias - those who consent may differ from those who do not
- Cannot be done for rare diseases or conditions with long natural history
High-Yield Exam Points Summary
| Point | Key Fact |
|---|---|
| RCT is | Epidemiologic experiment, No. 1 evaluation method |
| Heart of RCT | Randomization |
| Randomization eliminates | Selection bias |
| Randomization done using | Table of random numbers |
| Randomization done | After informed consent and eligibility confirmed |
| Criteria for participants | Informed consent + representative + eligible/susceptible |
| Most used blinding | Double blind |
| Ideal blinding | Triple blind |
| Cross-over design - patient is | His own control |
| Washout period needed for | Carry-over effects |
| TB trial in India showed | Domiciliary = Sanatorium treatment |
| RLF cause found by | Cessation experiment (withdrawal of high O2) |
| Whooping cough vaccine trial | 1946, MRC UK |
| Attrition means | Losses to follow-up |
| Non-randomized trial limitation | Low comparability, extra-statistical judgement needed |
- Park's Textbook of Preventive and Social Medicine, Chapter on Experimental Epidemiology (pp. 94-98)
Compare and contrast incidence and prevalence
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
All the core content is now in hand. Here is the full comparison directly from Park's PSM.
Incidence vs Prevalence - Park's PSM
Definitions
Incidence
"The number of new cases occurring in a defined population during a specified period of time."
Formula:
$$\text{Incidence Rate} = \frac{\text{Number of NEW cases of a disease in a given time period}}{\text{Population at-risk during that period}} \times 1000$$
Example: 500 new cases in a population of 30,000 in a year = 500/30,000 × 1000 = 16.7 per 1,000 per year
Important: Incidence rate MUST include the unit of time (e.g., "per 1,000 per year"). Writing "16.7 per 1,000" alone is inadequate.
Prevalence
"All current cases (old AND new) existing at a given point in time, or over a period of time, in a given population."
Although called a "rate," prevalence is technically a ratio.
Types of Prevalence
(a) Point Prevalence
- All current cases (old + new) at one point in time
- The "point" may practically span a few days or weeks (time needed to examine the population)
- When "prevalence rate" is used without qualification, it means point prevalence
Formula:
$$\text{Point Prevalence} = \frac{\text{All current cases (old + new) at a given point in time}}{\text{Estimated population at that same point in time}} \times 100$$
(b) Period Prevalence
- All current cases (old + new) existing during a defined period (e.g., annual prevalence)
- Includes cases arising before the period but extending into it, PLUS cases arising during the period
Formula:
$$\text{Period Prevalence} = \frac{\text{Existing cases (old + new) during a given time interval}}{\text{Estimated mid-interval population at-risk}} \times 100$$
The Classic Diagram (Fig. 2 from Park)
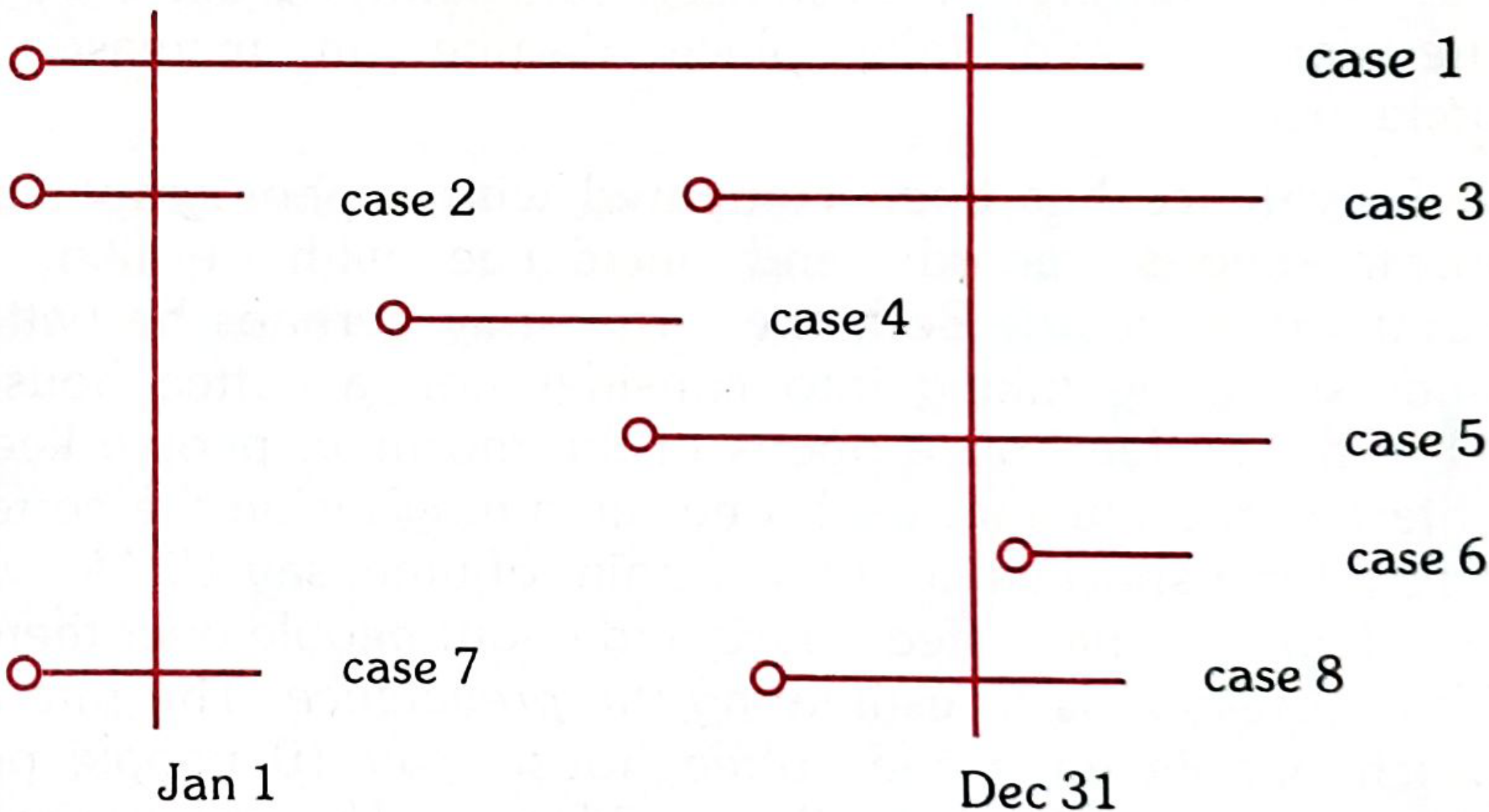
Using Fig. 2 (cases 1-8 shown across the year Jan 1 to Dec 31):
| Measure | Cases Counted |
|---|---|
| Incidence (new cases arising during the year) | Cases 3, 4, 5, 8 |
| Point prevalence (Jan 1) | Cases 1, 2, 7 |
| Point prevalence (Dec 31) | Cases 1, 3, 5, 6 |
| Period prevalence (whole year) | Cases 1, 2, 3, 4, 5, 6, 7, 8 |
Comparison Table
| Feature | Incidence | Prevalence |
|---|---|---|
| Definition | New cases in a time period | All cases (old + new) at a point/period |
| Cases counted | NEW cases only | OLD + NEW cases |
| Time dimension | Rates over a period (dynamic) | Snapshot at a point in time (static) |
| Expressed as | Rate (per 1,000 per year) | Ratio/proportion (per 100 or 1,000) |
| Denominator | Population at-risk | Population at-risk |
| Influenced by | Risk factors, exposure | Incidence + Duration of disease |
| Analogy (Park) | A film - continuous record | A photograph - instantaneous record |
| Study design | Cohort studies (prospective) | Cross-sectional (prevalence) surveys |
| Best used for | Aetiology, causation research | Administrative/planning purposes |
| Used in | Acute conditions primarily | Chronic conditions primarily |
Relationship Between Incidence and Prevalence
$$\boxed{P = I \times D}$$
Where:
- P = Prevalence
- I = Incidence
- D = Mean duration of illness
Derivations:
- Incidence = P/D
- Duration = P/I
Example: Incidence = 10/1,000/year; Mean duration = 5 years → Prevalence = 10 × 5 = 50 per 1,000
The Bathtub/Tap Analogy (Fig. 3 from Park)
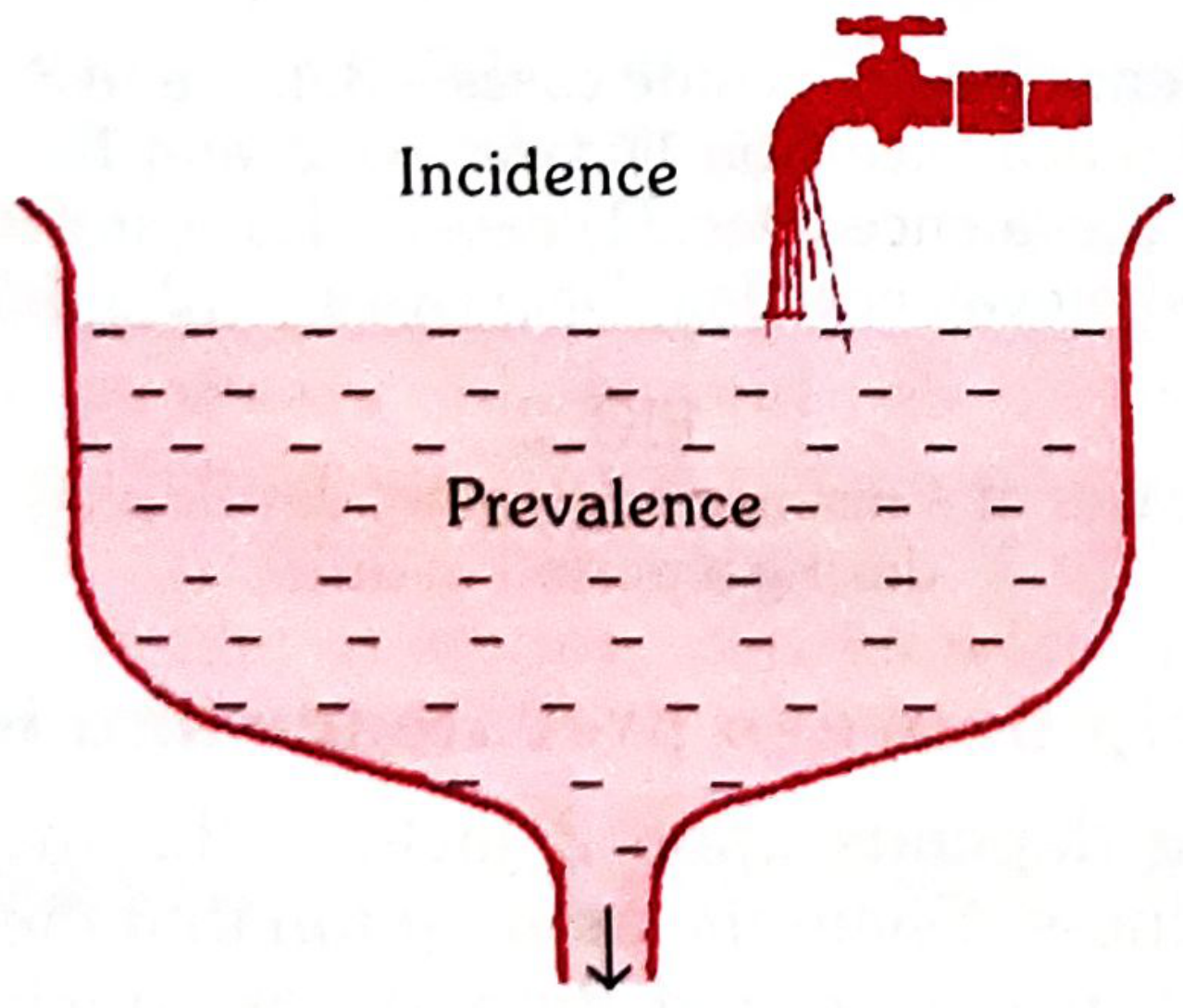
- Incidence = the tap (rate at which new cases pour in)
- Prevalence = the water level in the tub (all existing cases)
- Recovery/Death = the drain (cases leaving the pool)
The water level (prevalence) goes up when the tap (incidence) flows faster OR when the drain (recovery/death) slows down.
Coffee House Analogy (Park)
- Counting people inside the coffee house at 10 AM = Prevalence
- Rate at which people enter per hour = Incidence
What Affects Prevalence?
Prevalence increases when:
- Incidence increases
- Duration of disease increases (e.g., effective treatment that prevents death but does not cure)
- In-migration of cases
- Out-migration of healthy people
Prevalence decreases when:
- Incidence decreases
- More rapid recovery (shorter duration)
- More rapid death (shorter duration)
- New effective cure introduced
Paradox from Park: A treatment that prevents death but does not cure may paradoxically increase prevalence even without any change in incidence (e.g., early antiretrovirals in HIV).
Conversely, if duration decreases sufficiently, prevalence can fall despite a rise in incidence.
Uses of Each Measure
Uses of Incidence Rate
- To control disease - identifies rate of new case occurrence
- Aetiological research - studies causation, distribution, and pathogenesis
- Testing efficacy of preventive and therapeutic measures
- Monitoring and evaluation of disease control activities
- Optimal measure for formulating and testing aetiological hypotheses
Uses of Prevalence Rate
- Estimates the magnitude of health/disease burden in the community
- Identifies high-risk populations
- Administrative and planning purposes - estimating hospital beds, manpower needs, rehabilitation facilities
- Used when incidence data is unavailable (with caution - duration element must be assessed)
Limitations
| Incidence | Prevalence | |
|---|---|---|
| Limitation | Requires prospective follow-up - expensive, time-consuming | NOT ideal for studying aetiology - mixes incidence (causal factors) with duration (prognostic factors) |
| When not preferred | Difficult to obtain for rare/chronic diseases | Cannot establish causation |
High-Yield Exam Points
| Point | Key Fact |
|---|---|
| Incidence = | New cases / Population at-risk × 1,000 |
| Must express incidence as | Per 1,000 per year (time unit mandatory) |
| Prevalence = | All cases (old+new) / Population × 100 |
| "Prevalence rate" without qualifier = | Point prevalence |
| Incidence used for | Acute conditions, aetiology |
| Prevalence used for | Chronic conditions, planning |
| Incidence vs Prevalence analogy | Film vs Photograph |
| P = I × D means | TB - high prevalence relative to incidence (long duration) |
| Food poisoning - | Practically no prevalence (too short-lived) |
| Homicides - | Strictly no prevalence |
| Cross-sectional study measures | Prevalence |
| Cohort study measures | Incidence |
| Prevalence pool decreased by | Recovery, death, decreased incidence |
- Park's Textbook of Preventive and Social Medicine, pp. 72-74
This is a shared conversation. Sign in to Orris to start your own chat.