Cardiopulmonary bypass
Reading File
Finding Sources
Searching the Web
cardiopulmonary bypass mechanism complications current overview
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have rich, comprehensive content from multiple authoritative sources. Let me compile the full answer.
Cardiopulmonary Bypass (CPB)
Cardiopulmonary bypass is a technique that temporarily takes over the pumping and oxygenation functions of the heart and lungs, allowing the heart to be stopped for open cardiac surgery. It provides an extracorporeal circuit that diverts venous blood from the patient, oxygenates it, removes CO2, and returns it to the arterial circulation.
Indications
CPB is used for:
- Coronary artery bypass grafting (CABG)
- Open valve repair or replacement
- Repair of congenital heart defects
- Aortic root and ascending aorta surgery
- Cardiac transplantation
- Selected non-cardiac emergencies (e.g., massive PE refractory to other measures)
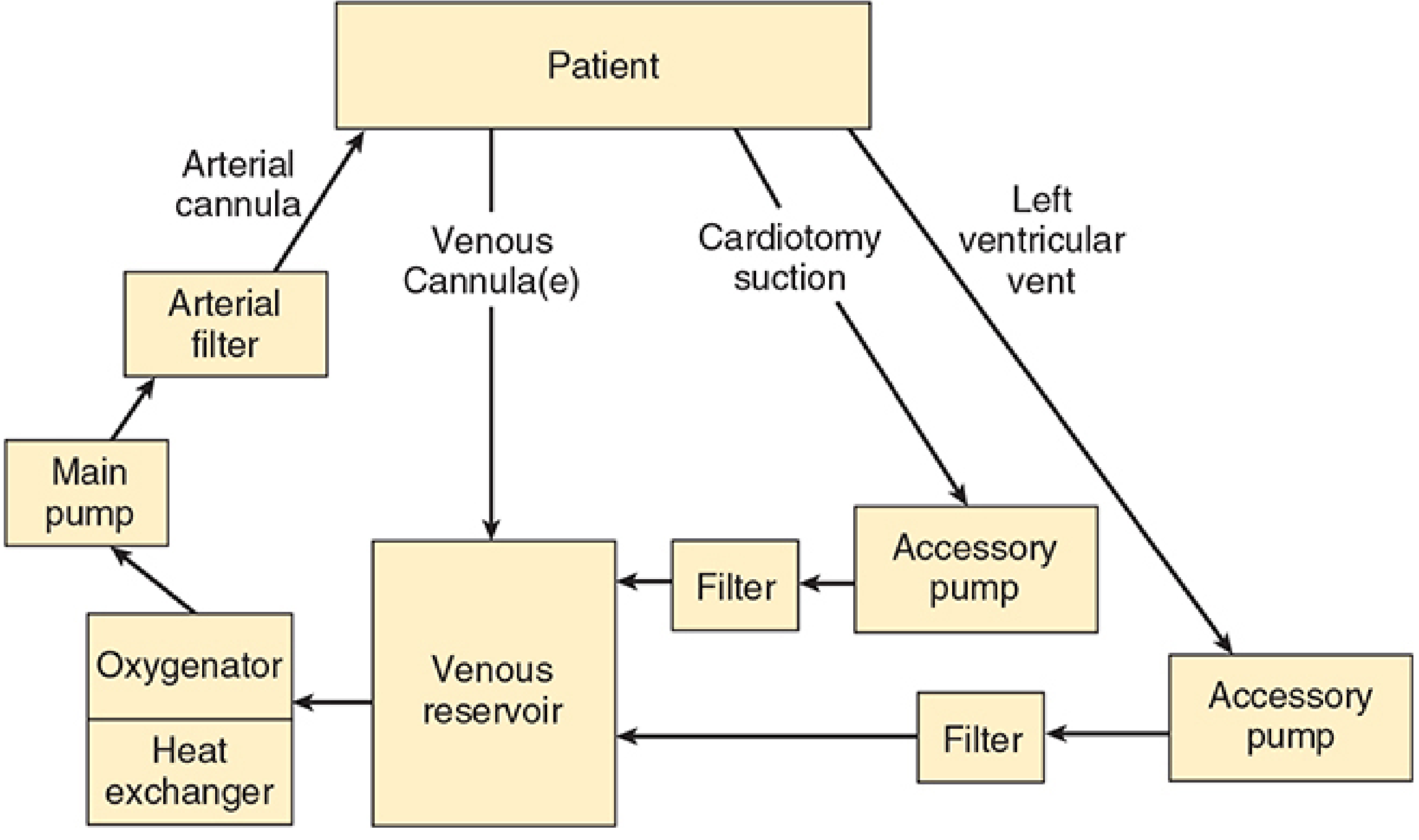
The CPB Circuit - Components
The typical machine has six essential components (Morgan & Mikhail, p. 811):
| Component | Function |
|---|---|
| Venous reservoir | Collects deoxygenated blood from the patient via venous cannulae |
| Oxygenator | Adds O2, removes CO2 across a gas-permeable silicone membrane |
| Heat exchanger | Controls blood temperature - allows cooling and rewarming |
| Main pump | Propels oxygenated blood back to the patient (roller or centrifugal) |
| Arterial filter | Removes microemboli (pore size 20-40 µm) before blood returns |
| Tubing | Conducts blood between components and cannulae |
Accessory pumps handle cardiotomy suction (blood salvage), left ventricular venting, and cardioplegia delivery.
Venous Reservoir
Blood drains by gravity from the right atrium, superior/inferior vena cava, or femoral vein into the reservoir. The driving force depends on the height difference between patient and reservoir and the resistance of cannulae and tubing - functioning like a siphon. Air in the venous line can cause an "air lock," stopping flow. If the reservoir empties with a roller pump running, air can be propelled into the patient, which is catastrophic.
Oxygenator
Modern units use membrane oxygenators - thin gas-permeable silicone membranes that allow equilibration with the gas mixture. This replaced older bubble oxygenators (which caused foaming and more blood trauma). The perfusionist can independently control PaO2 (by adjusting FiO2) and PaCO2 (by adjusting total gas flow rate). A volatile anesthetic is frequently added to the gas mixture to maintain anesthesia during bypass.
Pumps
- Roller pumps: compress flexible tubing in a rotating fashion, propelling a precise volume per revolution. Risk: if reservoir is empty, pump propels air.
- Centrifugal pumps: use a rotating cone to create flow by centrifugal force. Will not pump air (safer), but do not deliver a fixed volume per revolution and require flow monitoring.
Circuit Prime
Before use, the circuit is primed with 1200-1800 mL of fluid (typically lactated Ringer's) free of air bubbles. Other additives include colloid (albumin or starch), mannitol (promotes diuresis), heparin (500-5000 units), and bicarbonate. At the onset of bypass, hemodilution typically drops the hematocrit to ~22-27% in adults - acceptable because hypothermia reduces O2 consumption. Blood is added to the prime for neonates, infants, and severely anemic adults.
Cannulation Strategies
Standard (central) approach:
- Venous: cannula in right atrium or bicaval cannulae (SVC and IVC) - bicaval approach is preferred for intracardiac procedures to prevent air entrainment
- Arterial return: ascending aorta (most common) - blood is returned against the closed aortic valve, perfusing the coronary arteries and the rest of the arterial tree retrogradely
Peripheral (femoral) approach: femoral artery for arterial return, femoral vein for venous drainage - used for minimally invasive surgery, redo sternotomy, or aortic dissection where central cannulation is unsafe. Risk of retrograde embolization of aortic atheroma.
Anticoagulation
Full anticoagulation with unfractionated heparin is mandatory before cannulation to prevent clotting in the extracorporeal circuit.
- Dose: typically 300-400 units/kg IV
- Monitoring: Activated Clotting Time (ACT) - a point-of-care bedside test of the intrinsic clotting pathway
- Target ACT for CPB: >480 seconds (some centers use >400 s)
- ACT is checked every 30-60 minutes during bypass
- Reversal: protamine sulfate at end of bypass to neutralize heparin (1 mg per 100 units heparin given)
- Heparin resistance: can occur with antithrombin III deficiency - treat with FFP or antithrombin concentrate
Physiology During CPB
CPB creates distinctly non-physiological conditions:
| Parameter | During CPB |
|---|---|
| Flow | Non-pulsatile (continuous), usually 2.0-2.5 L/min/m² |
| Mean arterial pressure | Lower than normal, typically 50-80 mmHg |
| Temperature | Variable - normothermia (37°C) to deep hypothermia (15°C) |
| Hematocrit | Diluted to ~22-27% |
| CO2 management | pH-stat vs alpha-stat (see below) |
Temperature Management
Hypothermia reduces metabolic rate and O2 demand, protecting organs during the period of reduced/absent perfusion:
- Mild (32-37°C): minor procedures
- Moderate (26-32°C): most cardiac surgery
- Deep hypothermic circulatory arrest (DHCA) at ~15-20°C: allows complete circulatory arrest for up to ~60 minutes - used for complex aortic arch repairs and neonatal congenital heart surgery. Brain protection involves ice packing around the head, methylprednisolone 30 mg/kg, and mannitol 0.5 g/kg.
pH Management During Hypothermia
- Alpha-stat: CO2 is not added; blood gas values are corrected to 37°C; blood becomes relatively alkalotic at lower temperatures. Preferred for adults - better cerebral autoregulation.
- pH-stat: CO2 is added to maintain pH 7.40 and PaCO2 40 mmHg at actual (low) body temperature. Increases cerebral blood flow. May be preferable in children undergoing DHCA for better neurological outcomes.
Myocardial Protection
After the aorta is cross-clamped (isolating the heart from systemic circulation), cardioplegia is delivered to arrest the heart and protect the myocardium:
- Composition: high-potassium solution that depolarizes and arrests the heart in diastole, plus cold temperature (4-10°C) to reduce metabolic rate. May be crystalloid or blood-based (blood cardioplegia better preserves O2 delivery)
- Delivery routes:
- Antegrade: into aortic root or directly into coronary ostia - flows with coronary circulation
- Retrograde: via coronary sinus - used when antegrade delivery is limited (severe coronary disease, aortic regurgitation); often combined with antegrade for maximum protection
- Topical hypothermia: cold saline or ice-slush bathing the heart surface provides additional protection
- Volatile anesthetic preconditioning: volatile agents (e.g., isoflurane, sevoflurane) precondition the myocardium against ischemia-reperfusion injury and reduce infarct size
Signs of inadequate myocardial protection at end of bypass: asystole, conduction blocks, poor contractility, systemic hyperkalemia (from excessive cardioplegia volume).
Weaning from CPB
Discontinuation of bypass requires a systematic checklist approach:
Prerequisites before weaning:
- Rewarming complete (core temp ≥36-37°C)
- Hemostasis established, surgical repair complete
- Electrolytes normalized (especially K+, Ca2+, Mg2+)
- Heart rate and rhythm adequate (pacing if needed)
- De-airing of cardiac chambers completed
- Ventilation re-established
- Vasopressors/inotropes ready
Weaning process: gradually reduce CPB flow while increasing cardiac filling, monitoring TEE and hemodynamics. The perfusionist slowly releases venous clamps as cardiac output takes over.
Causes of difficulty weaning (Table from Barash):
- Inadequate myocardial protection / intraoperative infarction
- Reperfusion injury
- Uncorrected surgical lesion
- Severe ventricular dysfunction (RV or LV)
- Air embolism, tamponade
- Severe dysrhythmias
Inotropic support options: epinephrine, dopamine, dobutamine, milrinone (phosphodiesterase inhibitor - also reduces PVR/SVR). Calcium salts are particularly useful in children and when ionized calcium is low.
Complications of CPB
CPB triggers a systemic inflammatory response by exposing blood to non-endothelial surfaces. Major complications:
1. Neurological
- Stroke (macroembolism from aortic atheroma, air, debris; incidence ~1-5% after CABG)
- Neurocognitive dysfunction (subtle cognitive decline, memory impairment - common post-op)
- Both result from microemboli, hypoperfusion, or inflammatory mediators
2. Cardiac
- Myocardial stunning / low cardiac output syndrome
- Reperfusion arrhythmias (AF most common postoperatively)
- Perioperative MI
3. Renal
- Acute kidney injury (AKI) - from non-pulsatile flow, hemolysis, microemboli, inflammatory mediators, contrast if angiography preceded surgery
- Hemoglobinuria from RBC destruction in circuit
4. Pulmonary
- Post-pump pulmonary dysfunction ("pump lung") - from systemic inflammatory response, complement activation, neutrophil sequestration in lungs
- Atelectasis, prolonged ventilation
5. Haematological
- Coagulopathy: dilution of clotting factors and platelets, platelet dysfunction from circuit contact, fibrinolysis - major cause of post-CPB bleeding
- Heparin rebound (heparin redistributes from tissue depots after protamine reversal)
- Heparin-induced thrombocytopenia (HIT) - delayed but serious; alternative anticoagulation required
6. Gastrointestinal
- GI complications (acute cholecystitis, mesenteric ischemia, upper GI bleeding, pancreatitis) occur more commonly with prolonged CPB time, elderly patients, cardiogenic shock, and postoperative renal failure (Yamada's Gastroenterology)
7. Air Embolism
- Catastrophic if massive air enters arterial line - cardiac surgery team must be vigilant about reservoir levels, de-airing cardiac chambers before weaning
Pediatric Considerations
- Circuit prime volume is often 200-300% of an infant's blood volume, so blood must be added to prevent dangerous hemodilution
- Mean arterial pressure is lower (20-50 mmHg) due to high compliance of the arterial system and intracardiac/extracardiac shunts
- High flow rates (up to 200 mL/kg/min) may be needed
- Intense inflammatory response - corticosteroids (methylprednisolone) are commonly given prophylactically
- Modified ultrafiltration post-bypass: removes inflammatory cytokines and reverses hemodilution
- pH-stat management associated with better neurological outcomes when DHCA is used
- Post-CPB hemostatic defects are pronounced - FFP and platelets often required
The Perfusionist
Operation of the CPB machine is managed by a certified clinical perfusionist - a specialized allied health professional. Safe conduct of CPB demands continuous, clear communication among the surgeon, anesthesiologist, and perfusionist.
Summary
CPB is a life-saving but physiologically stressful technique. Its success depends on:
- A properly primed and vented extracorporeal circuit
- Adequate anticoagulation (ACT-guided heparin dosing)
- Appropriate flow rates and perfusion pressure
- Temperature management matched to the surgical plan
- Optimal myocardial protection
- Systematic weaning with inotropic support as needed
- Thorough reversal of anticoagulation and hemostasis
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e, pp. 811-875
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, Chapter 39
- Pye's Surgical Handicraft, 22nd Edition, p. 242
- Yamada's Textbook of Gastroenterology, 7e
This is a shared conversation. Sign in to Orris to start your own chat.