Treatment of acute diarrhea flowchart.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have everything I need - the flowchart image and comprehensive treatment details. Here is the complete answer:
Treatment of Acute Diarrhea
Flowchart (Goldman-Cecil Medicine)
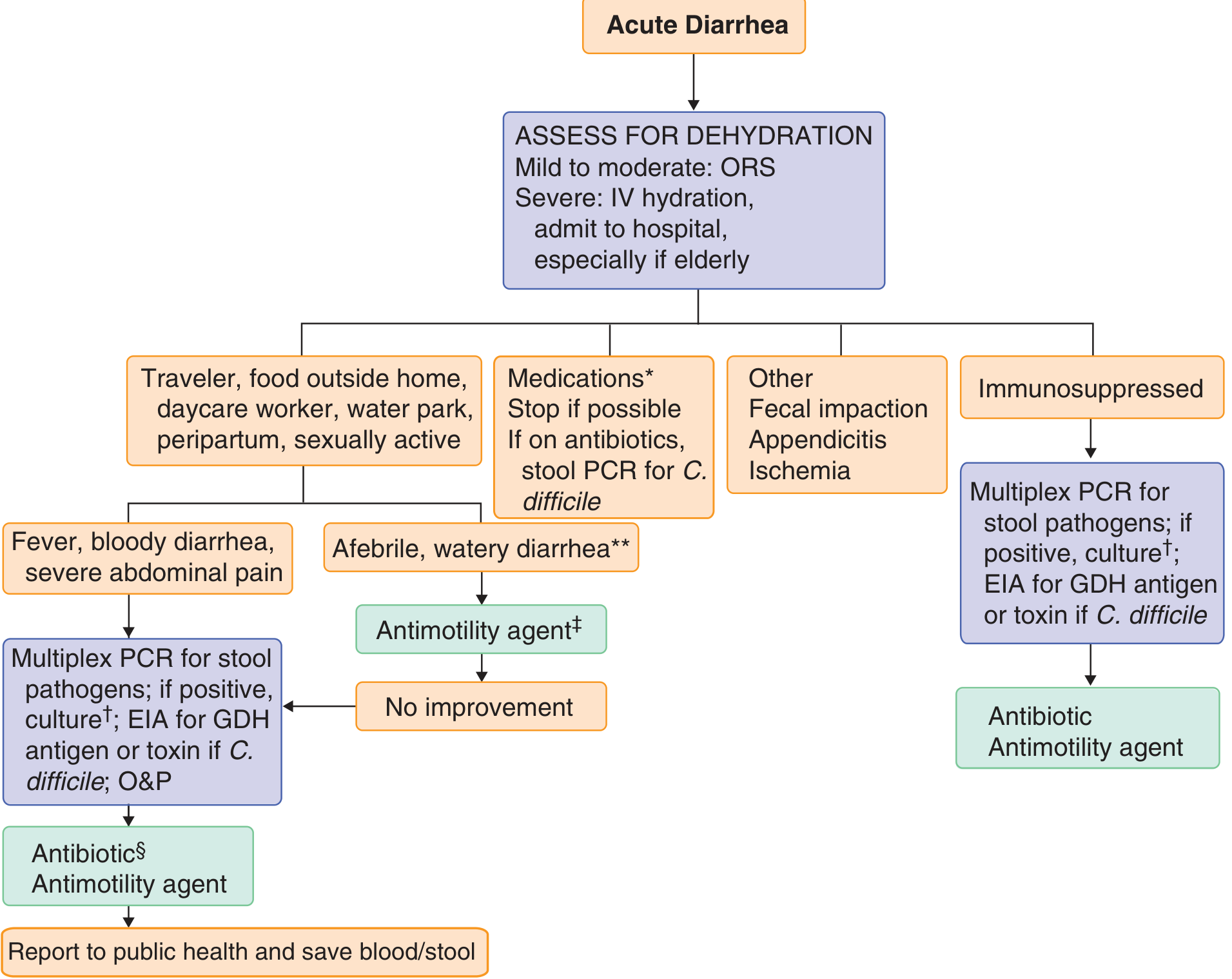
Source: Goldman-Cecil Medicine, International Edition - Fig. 126-1: Approach to the diagnosis and treatment of acute diarrhea.
Flowchart Walkthrough
Step 1 - Assess for Dehydration (ALL patients)
| Severity | Action |
|---|---|
| Mild to moderate | Oral rehydration solution (ORS) |
| Severe | IV hydration (lactated Ringer's or saline); admit to hospital, especially if elderly |
Step 2 - Branch by Clinical Context
A. High-risk exposure (traveler, food outside home, daycare worker, water park, peripartum, sexually active):
- Afebrile, watery diarrhea: Antimotility agent (e.g., loperamide 2 mg QID). If no improvement → workup (below)
- Fever, bloody diarrhea, severe abdominal pain:
- Multiplex PCR for stool pathogens; culture if positive
- EIA for GDH antigen or toxin (if C. difficile suspected)
- Ova & parasites exam
- Then: Antibiotic + antimotility agent
- Report to public health; save blood/stool samples
B. Medications
- Stop offending drug if possible
- If currently on antibiotics: stool PCR for C. difficile
-
700 drugs cause diarrhea (metformin, SSRIs, PPIs, checkpoint inhibitors, laxatives, etc.)
C. Other causes
- Consider fecal impaction, appendicitis, ischemia
D. Immunosuppressed patients
- Multiplex PCR for stool pathogens; culture if positive
- EIA for GDH antigen or toxin if C. difficile suspected
- Then: Antibiotic + antimotility agent
Treatment Details
1. Fluid Replacement
- Mild-moderate dehydration: ORS (Na⁺ 75 mmol/L, osmolarity 245 mmol/L reduced-osmolarity preferred in non-cholera). Infants/children: 50-100 mL/kg over 4-6 hrs. Adults: up to 1000 mL/hr.
- Severe dehydration: IV lactated Ringer's or saline ± potassium + bicarbonate.
- Continue ORS at a rate equaling stool loss + insensible losses until diarrhea ceases.
2. Symptomatic/Antimotility Agents
| Drug | Dose | Notes |
|---|---|---|
| Loperamide | 2 mg PO QID (max 16 mg/day) | Safe in acute/traveler's diarrhea; avoid in dysentery (bloody stool + high fever) |
| Bismuth subsalicylate | 525 mg PO q30-60 min x 5 doses; repeat day 2 | Safe, effective in bacterial diarrhea |
| Racecadotril | 100 mg PO TID (adults); 1.5 mg/kg TID (children) | Enkephalinase inhibitor; antisecretory without paralyzing motility |
| Loperamide + simethicone | 2 mg + 125 mg QID | Reduces cramps and duration of traveler's diarrhea |
Opiates and anticholinergics are not recommended for invasive bacterial diarrhea.
3. Antibiotic Therapy
Empiric (while awaiting cultures):
- 1st line: Fluoroquinolones - Ciprofloxacin 500 mg PO BID x 1-3 days, or Levofloxacin 500 mg PO daily x 1-3 days
- 2nd line: Trimethoprim-sulfamethoxazole 1 DS tablet PO BID x 5 days
- If Campylobacter suspected: add Azithromycin 500 mg/day x 3 days
- Traveler's diarrhea (Mexico): Rifaximin 200 mg TID or 400 mg BID x 3 days (not effective vs. Campylobacter/Shigella)
- Resistant strains (Shigella, Campylobacter): Azithromycin 500 mg day 1, then 250 mg/day x 4 days
Specific indications:
| Pathogen/Situation | Drug |
|---|---|
| Shigellosis | Fluoroquinolone or azithromycin |
| Cholera | Fluoroquinolone or doxycycline |
| C. difficile | Fidaxomicin 200 mg PO BID x 10 days (preferred over vancomycin to prevent recurrence); Vancomycin 125 mg PO QID x 10 days |
| Recurrent C. difficile | Fecal microbiota transplantation (90% resolution) > vancomycin (30%); or bezlotoxumab 10 mg/kg IV x 1 dose |
| Parasites (Giardia, Cryptosporidium) | Metronidazole or specific antiparasitic |
| E. coli O157:H7 | No antibiotics (increases risk of HUS) |
| Viral diarrhea | No antibiotics |
Mandatory antibiotic indications (regardless of pathogen):
- Immunosuppressed patients
- Prosthetic valves, vascular/orthopedic prostheses
- Congenital hemolytic anemias (especially salmonellosis)
- Extremes of age
4. Adjuncts
- Zinc 20 mg elemental PO daily: reduces recurrences in malnourished children
- Probiotics: not beneficial in children with acute diarrhea; insufficient RCT data in adults
- Anxiolytics (diazepam 2 mg PO BID-QID) and antiemetics (promethazine 12.5-25 mg PO) for symptom relief
- Chemotherapy/radiation diarrhea: loperamide + NSAIDs (naproxen 250-500 mg BID); severe cases: octreotide up to 700 mcg/day SQ
- Checkpoint inhibitor diarrhea: stop agent + glucocorticoids (0.5-2 mg/kg prednisone with 4-6 week taper)
Management by Patient Appearance (Sleisenger & Fordtran):
| Patient Appearance | Action |
|---|---|
| Nontoxic | Symptomatic therapy + rehydration only |
| Toxic | Fluid/electrolyte repletion + CBC + metabolic panel + stool cultures/PCR/O&P/C. diff testing ± sigmoidoscopy/colonoscopy |
- Goldman-Cecil Medicine, Ch. 126 (p. 1461)
- Sleisenger and Fordtran's GI and Liver Disease, Table 16.3 (p. 233)
This is a shared conversation. Sign in to Orris to start your own chat.