donot make any file rather write it in chat. Need more information on specific pathologies (VKH management, melanoma workup, diabetic monitoring)?
VKH Management, Choroidal Melanoma Workup, and Diabetic Retinopathy Monitoring
1. Vogt-Koyanagi-Harada (VKH) - Full Management
Pathophysiology & Background
Four Clinical Phases
| Phase | Features |
|---|---|
| Prodromal | Meningismus, encephalopathy, cranial nerve palsies, tinnitus, vertigo, deafness, hypersensitivity of skin to touch |
| Acute Uveitic | Bilateral granulomatous anterior/posterior uveitis, multifocal choroidal infiltration, Dalen-Fuchs nodules, vitritis, papillitis, serous/exudative retinal detachments, ciliary effusion |
| Convalescent | Alopecia, poliosis, vitiligo, "sunset glow" fundus (RPE/choroidal depigmentation), Sugiura sign (perilimbal depigmentation in Japanese patients) |
| Chronic Recurrent | Smouldering anterior uveitis with exacerbations, subretinal fibrosis, NVD/NVE, glaucoma, cataract |
Diagnostic Criteria (Modified)
- Complete VKH: All 5 criteria present
- Incomplete VKH: Criteria 1-3 + either 4 or 5
- Probable VKH (isolated ocular): Criteria 1-3 only
- No history of penetrating ocular trauma
- No evidence of other ocular disease
- Bilateral uveitis (anterior or panuveitis)
- Neurological/auditory findings
- Dermatological findings (not preceding CNS/ocular onset) - alopecia, poliosis, vitiligo
Investigations
- Lumbar puncture (if diagnosis uncertain): transient lymphocytic pleocytosis + melanin-containing macrophages in CSF
- FA (acute phase): multifocal hyperfluorescent dots at RPE level, followed by subretinal dye pooling; chronic phase shows RPE window defects
- FAF: hyperautofluorescence at serous detachment sites
- OCT: quantifies subretinal fluid; subretinal septae are characteristic; septae height correlates with disease activity
- ICGA: stromal hypofluorescent dark dots in active disease (more sensitive than FA for choroidal involvement)
- B-scan US: diffuse choroidal thickening; excludes posterior scleritis
- UBM: demonstrates ciliary effusion
Treatment
- First line: High-dose oral prednisolone 1-2 mg/kg/day, tapered over 3-6 months
- May be preceded by IV methylprednisolone pulse: 500-1000 mg/day for severe disease
- Anterior uveitis: topical steroids + cycloplegics
- Steroid-resistant: add immunosuppressives (methotrexate, mycophenolate, azathioprine)
- Biologics: Infliximab (anti-TNF) should be used early if no steroid response - do not delay escalation
Complications to Monitor
- Macular neovascularization, subretinal fibrosis, NVG, cataract, glaucoma
- Prognosis depends on early disease control - neurological/auditory features tend to resolve; skin/hair changes typically persist
2. Choroidal Melanoma - Full Workup
Background
- Most common primary intraocular malignancy in adults; accounts for 80% of uveal melanomas
- Distinct molecular profile from cutaneous melanoma (BAP1 mutations in ~50%, NOT BRAF/RAS-driven)
- Peak presentation: ~60 years. Metastasis: liver (primary), then bone/lung. Only 1-2% have detectable metastases at presentation
- 10-year mortality: up to 50%
Signs
- Subretinal fluid (SRF)
- Thickness ≥2 mm with abrupt choroidal elevation
- Geographic orange pigment (lipofuscin) over the lesion
- Dome, mushroom, or plateau shape with apical congested vessels
- "Collar stud" shape if Bruch membrane breach occurs
- Break in Bruch membrane with subretinal hemorrhage
- Growth on serial imaging
Risk Factor Mnemonic for Nevus-to-Melanoma Transformation: TFSOM-DIM
- T - Thickness >2 mm (ultrasound)
- F - Fluid subretinal (OCT)
- S - Symptoms (visual loss, VA <20/50)
- O - Orange pigment/hyperautofluorescence (AF imaging)
- M - Melanoma hollow (low internal reflectivity on A-scan US)
- D - Diameter >5 mm (photography)
- I - ---
- M - ---
If 4 or more TFSOM-DIM factors are present, >50% chance of growth - treat as small choroidal melanoma
Workup Protocol
- Complete dilated fundus exam with 20D lens; detailed clinical drawing noting size and location
- Color fundus photography - baseline for diameter tracking and documentation of growth
- OCT with enhanced-depth imaging (EDI-OCT) - overlying retinal changes, SRF, tumor profile
- Fundus autofluorescence (FAF) - orange pigment (lipofuscin), RPE disturbance
- B-scan ultrasonography - tumor thickness, internal acoustic qualities (low internal reflectivity = "hollow" = melanoma); A-scan for reflectivity pattern
- FA - intrinsic "double circulation" pattern; helps exclude differential
- ICGA - hypofluorescence throughout; better defines tumor extent vs FA (less RPE interference)
- MRI - demonstrates extraocular/orbital extension, assists in differentials
- Fine needle biopsy or 25G vitrectomy biopsy - when diagnosis cannot be established by non-invasive means
- Immunocytochemistry (PAX8): melanoma and melanocytoma are PAX8-negative; pigmented adenocarcinoma is PAX8-positive
Genetic/Molecular Analysis
- Chromosome 3 monosomy (M3) + chromosome 8q gain (i8q): strongly correlates with poor prognosis - especially together
- BAP1 mutation (~50%): associated with higher metastatic risk
- Use Liverpool Uveal Melanoma Prognosticator (LUMPO) online tool for individualized survival prediction
- Low-risk genetic profiles can have reduced surveillance intensity
Systemic Metastatic Workup
- Liver function tests + liver ultrasound (mainstay - liver is the primary metastatic site)
- Chest X-ray (low yield unless liver disease present)
- Whole-body PET/CT - greater sensitivity for extrahepatic metastases but high radiation dose; role still being defined
Treatment (size-based)
| Tumor Size | Treatment |
|---|---|
| Small (<2 mm thick, no high-risk features) | Observation q3-4 months x 1, then annually |
| Small-medium (<20 mm diameter, ≤10 mm thick) | Episcleral plaque brachytherapy (Ru-106 or I-125) - survival equivalent to enucleation |
| Large / vision-threatening / extraocular | Enucleation |
| Ciliary body involvement | Proton beam radiotherapy, or enucleation |
3. Diabetic Retinopathy - Monitoring & Management
Risk Factors for Progression
- Duration of diabetes (most important predictor)
- Poor glycemic control (high HbA1c) - DCCT/UKPDS confirmed tight control reduces DR risk
- Caution: rapid improvement in glucose control can paradoxically worsen retinopathy short-term
- Hypertension, hyperlipidaemia, pregnancy, anaemia, cataract surgery
ETDRS Classification + Monitoring Intervals
| Category | Key Signs | Review Interval |
|---|---|---|
| No DR | None | 12 months |
| Very Mild NPDR | Microaneurysms only | 12 months |
| Mild NPDR | MA + haemorrhages + exudates + CWS, below moderate level; no IRMA | 6-12 months (based on severity, systemic factors) |
| Moderate NPDR | Severe retinal haemorrhages (>ETDRS photo 2A) in 1 quadrant; cotton-wool spots; venous beading | ~6 months |
| Severe NPDR (Pre-proliferative) | 4-2-1 rule: haemorrhages in all 4 quadrants OR venous beading in ≥2 quadrants OR IRMA in ≥1 quadrant | 3-4 months; consider PRP |
| PDR (Non-high-risk) | NVD or NVE without high-risk features | 2-3 months; consider early PRP |
| High-risk PDR | NVD >1/3 disc area OR NVD + VH/preretinal haemorrhage OR NVE >1/2 disc area + haemorrhage OR any NVI/NVA | Urgent PRP or anti-VEGF |
| Advanced disease | TRD, persistent VH, NVG | Vitreoretinal surgery evaluation |
Clinically Significant Macular Oedema (CSMO) Criteria (ETDRS)
- Retinal thickening within 500 μm of the fovea center
- Hard exudates within 500 μm of fovea with adjacent thickening
- Retinal thickening ≥1 disc area in size, part of which is within 1 disc diameter of fovea
Treatment Summary
- Anti-VEGF (intravitreal) - first-line for centre-involving DME with VA loss (ranibizumab, aflibercept, bevacizumab, faricimab)
- Intravitreal steroids (triamcinolone, dexamethasone implant) - second-line or for pseudophakic patients
- Focal/grid laser - for non-centre-involving DME or adjunct
- PRP (panretinal photocoagulation) - indicated for:
- NVD ≥1/4-1/3 disc area
- Any NVD + preretinal/VH
- NVE ≥1/2 disc area + preretinal/VH
- Any NVI or NVA
- Anti-VEGF - alternative to PRP; preferred if DME coexists or peripheral view is limited by VH. Use cautiously in unreliable patients (risk of worsening if lost to follow-up)
- Dense, non-clearing VH causing significant VA loss
- Traction RD involving or progressing toward macula
- Macular ERM / VMT causing significant symptoms
- Dense premacular haemorrhage
- Chronic DME unresponsive to other treatment
- Severe neovascular/fibrous proliferation unresponsive to laser or anti-VEGF
Pregnancy Monitoring (Diabetic Retinopathy)
| Baseline DR Status | Risk | Eye Exam Schedule |
|---|---|---|
| Gestational diabetes | No DR risk | None needed |
| No/minimal NPDR | Progression unlikely | 1st and 3rd trimester |
| Mild-to-moderate NPDR | Progression up to 50%; postpartum regression common | Every trimester |
| High-risk NPDR | Progression up to 50% | Monthly |
| PDR | Tends to progress rapidly | Monthly; treat promptly |
DME in late pregnancy often resolves postpartum and may not need treatment if it develops late in gestation. If DR is present, review frequency should reflect individual risk - up to every 2 weeks in severe cases.
- VKH: Don't delay steroid escalation to biologics - infliximab early if steroid-resistant. FAF and OCT (subretinal septae) are key imaging tools.
- Melanoma: TFSOM-DIM mnemonic for nevus risk stratification; genetic profiling (BAP1, chr 3) drives metastatic surveillance intensity; liver ultrasound is the primary metastatic screening tool.
- Diabetic monitoring: The 4-2-1 rule identifies severe NPDR ready for PRP; anti-VEGF has largely replaced focal laser as first-line for centre-involving DME; pregnancy dramatically accelerates DR - monthly monitoring for PDR.
what are missing in the word file? detailed evaluation and add the contents to the word file but write it in chat no need for pdf or file
Gap Analysis: What's Missing from the Word Document (ERD.docx)
MISSING PART: RHEGMATOGENOUS RETINAL DETACHMENT (RRD)
MISSING PART 3 (to insert before current Part 3): RHEGMATOGENOUS RETINAL DETACHMENT (RRD)
- A full-thickness retinal break - a tear (U-shaped/horseshoe, caused by vitreoretinal traction) or a round hole (caused by retinal atrophy without traction)
- Liquefied (synchytic) vitreous - vitreous that has undergone syneresis (gel-to-liquid transformation) and can therefore pass through the break
- Posterior Vitreous Detachment (PVD): With age (or myopia, trauma), the vitreous cortex separates from the retinal surface. At sites of abnormal vitreoretinal adhesion (lattice degeneration, cystic tufts, vitreous base anomalies), this traction tears the retina rather than cleanly separating from it, producing a horseshoe (U-shaped) tear
- Once a break exists, synchytic vitreous passes through it into the subretinal space, progressively separating the neurosensory retina from the RPE
- The RPE pump cannot compensate once the volume of entering fluid exceeds its clearance capacity
| Break Type | Mechanism | Risk of RD |
|---|---|---|
| Horseshoe/U-tear | PVD traction avulses a flap of retina; vitreous remains attached to the flap | High - open flap acts as a valve |
| Round/atrophic hole | Focal retinal atrophy, no vitreous traction | Low in emmetropes; higher in high myopes |
| Dialysis | Tear at the ora serrata; associated with blunt trauma | Moderate - slow accumulation |
| Giant retinal tear (GRT) | >90 degrees circumferential tear; high myopia, trauma, Stickler syndrome | Very high; surgical emergency |
| Operculated hole | Complete avulsion of a retinal flap; traction released; vitreous pulls the "lid" away | Lower than horseshoe tear (traction relieved) |
- Lattice degeneration: Most important predisposing lesion. Present in 8-10% of the population but accounts for 20-30% of all RRDs. Sharply demarcated areas of retinal thinning with a criss-cross pattern of white lines (sclerosed vessels), pigment, and sometimes atrophic holes or U-tears at the posterior edge. Prophylactic treatment of asymptomatic lattice is NOT routinely indicated - the lifetime risk of RD from any given area of lattice is low
- Cystic retinal tufts: Present in up to 5% of the population; strong vitreoretinal adhesion causes U-tears and round holes; may account for 5-10% of RDs
- Snailtrack degeneration: Tightly packed snowflakes; round holes common; prophylaxis not needed
- Degenerative retinoschisis: A split within the retinal layers (at the outer plexiform layer); outer layer holes + inner layer holes together can cause RRD, but with good prognosis due to slow accumulation of fluid
- Myopia: High myopes (>6 dioptres) have a 10x increased lifetime risk. Elongated globe, thinner peripheral retina, earlier vitreous liquefaction, and a higher prevalence of lattice
- Age: PVD incidence rises steeply after 50 years; acute symptomatic PVD is the most common precipitant of RRD
- Ocular surgery: Prior cataract surgery (especially complicated by posterior capsule rupture) dramatically increases risk - YAG laser capsulotomy is an additional, though smaller, risk factor
- Trauma: Blunt trauma causes dialysis (traumatic RD) and giant retinal tears; penetrating trauma causes direct retinal breaks
- Family history: First-degree relatives of RRD patients have 5x increased risk
- Fellow eye: After RRD in one eye, the fellow eye has a 10-15% lifetime risk; lattice is often bilateral
- Stickler syndrome: Autosomal dominant mutation in COL2A1 or COL11A1; most common hereditary cause of RRD; bilateral giant retinal tears
- Marfan syndrome: Ectopia lentis + vitreous degeneration + high myopia
- Previous vitreoretinal surgery: Sclerotomy sites and membrane peeling can create breaks
- Photopsia (flashing lights): The cardinal early warning symptom. Caused by mechanical traction on the retina at the site of vitreoretinal adhesion during acute PVD. Typically monocular, in the temporal field, and associated with eye movement
- New floaters: Pigmented vitreous cells (Tobacco dust/Shafer's sign - pigment cells from torn RPE in the anterior vitreous) are pathognomonic of a retinal break with possible imminent RRD. A sudden shower of new floaters (from vitreous haemorrhage or collagen fibres released during acute PVD) is also an urgent symptom
- Visual field defect (curtain/shadow): The detachment extends as a dark curtain or shadow from the periphery. The field defect is usually in the opposite direction to the break (inferior break → superior field defect; superior break → inferior field defect). This field defect may progress over hours to days
- Central vision loss: Indicates macular involvement - this converts the case from urgent to an emergency
- Metamorphopsia (distortion): Occurs when SRF has reached the macula but not yet caused complete macular detachment
KEY POINT: In exudative and tractional RD, photopsia is characteristically absent. The presence of photopsia strongly favours rhegmatogenous RD - it implies vitreoretinal traction pulling mechanically at the retina.
- Tobacco dust (Shafer's sign): Pigmented cells in the anterior vitreous, seen on slit-lamp examination as dark cells tumbling in the vitreous cavity, anterior to the hyaloid face. Virtually pathognomonic of a full-thickness retinal break. Must be actively looked for on slit-lamp exam in any patient with acute PVD symptoms
- Vitreous haemorrhage: From tearing of a superficial retinal blood vessel at the break site. Blood in the vitreous appears as red cells or a haze. Dense VH obscures the fundus and mandates B-scan ultrasound
- Convex, corrugated, opaque detachment: The detached retina is grey-white and corrugated (unlike the smooth convex surface of exudative RD). It undulates with eye movement (cf. tractional RD which is tethered and immobile)
- The retinal break: A full-thickness break appears as a red/orange area against the grey-white detached retina - the choroidal vasculature is visible through it. U-tears have the flap pointing anteriorly (toward the vitreous base) and a "horse-shoe" shape
- Absence of shifting fluid: Unlike exudative RD, the SRF in RRD does NOT shift with gravity - it is anchored by the break and vitreous traction
- Intraocular pressure (IOP): Characteristically lower in the detached eye than the fellow eye (by 5-8 mmHg) due to increased RPE pumping. A paradoxically high IOP can occur in Schwartz-Matsuo syndrome (shed photoreceptor outer segments clog the trabecular meshwork)
- Relative afferent pupillary defect (RAPD): Present in large RDs due to reduced retinal input from the detached area
- Subretinal demarcation lines ("tide marks"): Pigmented lines at the posterior extent of chronic SRF, forming after ~3 months. Represent RPE cell proliferation at the border between flat and detached retina
- Intraretinal cysts: Develop after ~1 year of detachment
- Fixed retinal folds: PVR-related (see below)
| Feature | RRD | Exudative RD | Tractional RD | Retinoschisis |
|---|---|---|---|---|
| Retinal breaks | Present | Absent | Absent | Outer layer holes only |
| Fluid shifts | Absent | Present | Absent | Absent |
| Retinal surface | Corrugated, opaque | Smooth, translucent | Concave, taut | Smooth, dome-shaped, translucent |
| Photopsia | Present (acute) | Absent | Absent | Absent |
| Tobacco dust | Present | Absent | Absent | Absent |
| Retinal mobility | Freely mobile, undulates | Freely mobile | Severely reduced | Immobile |
| Visual field defect | Relative | Relative | Relative | Absolute (splitting of neurons) |
| Choroid visible? | Obscured by opaque retina | May be visible (tumour/HTN) | Obscured | Normal choroid visible through schisis |
- Slit-lamp biomicroscopy: Look for Shafer's sign (tobacco dust), lens status, presence of PVD, vitreous haemorrhage, uveitis
- Indirect ophthalmoscopy with scleral depression: Mandatory. The single most important clinical tool for break detection. Scleral depression extends the visible field to the ora serrata, revealing peripheral breaks. Both eyes must be examined - the fellow eye may have asymptomatic lattice or breaks requiring prophylaxis
- Widefield fundus photography / Optos: Documents extent of RD and break location; useful for serial monitoring of untreated/treated cases
- B-scan ultrasonography: When vitreous haemorrhage, dense cataract, or corneal opacity prevents fundal view. Shows the detached retina as a highly reflective mobile membrane with open anterior end (attached at ora serrata and optic disc). Good mobility distinguishes RRD from tractional RD (immobile)
- OCT: Confirms subretinal fluid, identifies macular-on vs macular-off status, detects subtle subfoveal SRF not visible ophthalmoscopically, and assesses photoreceptor layer integrity for prognosis
- Macula-on RRD (SRF has not yet reached the fovea): Urgent surgery within 24-48 hours - every hour increases the risk of SRF reaching the macula
- Macula-off RRD (fovea detached): Early surgery - within 7-10 days gives better visual outcomes than late repair. Beyond 10-14 days of macular detachment, photoreceptor degeneration becomes irreversible
- Exception: Chronic RRD with stable demarcation lines and no recent progression - can be timed semi-electively
- Patient positioned so the retinal break is in the most dependent position (reduces SRF spread)
- Nil by mouth if urgent surgery
- Minimise physical activity
- Office-based procedure: intravitreal gas bubble (SF₆ 20% or C₃F₈ 12-16%) + laser or cryotherapy to seal the break
- Gas bubble mechanically seals the break from inside; RPE pump reabsorbs SRF over days
- Requires the break to be in the upper two-thirds of the retina (supine position allows bubble to reach it)
- Break or cluster of breaks must span less than 1-2 clock hours
- Advantages: minimally invasive, no anaesthesia, preserves conjunctiva
- Limitations: single-session reattachment rate ~70-80% (inferior to scleral buckle or PPV); new breaks may develop elsewhere; not suitable for inferior or giant breaks
- External procedure: a silicone explant is sutured to the sclera, creating an inward indentation (buckle) that closes the retinal break by apposing the RPE to the sensory retina, and relieves dynamic vitreoretinal traction at the site
- Cryotherapy applied around the break before buckle placement creates chorioretinal adhesion
- Subretinal fluid drainage may be performed if SRF is deep or the retina does not reattach spontaneously
- Configurations: radial (for single U-tear), segmental, circumferential, or encircling (360-degree band for multiple breaks or PVR)
- Indications: young patients (preserves accommodation by avoiding vitrectomy), inferior breaks, traumatic dialysis, phakic eyes without significant vitreous opacification
- Complications: induced myopia, anisometropia, strabismus (muscle traction), scleral buckle extrusion, choroidal detachment
- Internal approach: removal of vitreous + fluid-air exchange + laser retinopexy + tamponade (gas or silicone oil)
- Retinotomy or drainage of SRF performed under perfluorocarbon liquid (PFCL) if retina is bullous
- Gas tamponade (SF₆ or C₃F₈) for most cases; silicone oil for inferior breaks, PVR, patients unable to posture, or chronic detachments
- Combined PPV + scleral buckle for giant retinal tears, PVR (stage C and above), and complex detachments
- Increasingly preferred over scleral buckling by many surgeons, especially for pseudophakic patients and those with:
- Posterior breaks (macular holes causing RD)
- Giant retinal tears
- Significant vitreous haemorrhage
- PVR
- Grade A: Vitreous haze, pigment clumps
- Grade B: Retinal wrinkling, rolled edge of break, decreased retinal mobility
- Grade C: Full-thickness fixed retinal folds (anterior or posterior)
- Gas tamponade requires face-down or specific head positioning for days to weeks
- Silicone oil removal 3-6 months postoperatively once retina stable
- New break surveillance: fellow eye and operated eye must be monitored at 1-2 weeks, 1 month, 3 months, then annually
- Cataract formation: accelerated after PPV in phakic patients (often within 1-2 years)
- Single-operation reattachment rates: 80-90% with modern vitrectomy; 85-90% with scleral buckle
- Final anatomical reattachment (after re-operations): >95%
- Visual outcome: Primarily determined by macular involvement duration:
- Macula-on repair: 90%+ achieve >6/12 BCVA
- Macula-off <1 week: 50-70% achieve >6/12
- Macula-off >1 month: <20% achieve >6/12; mean BCVA ~6/60
MISSING FROM COMPARISON TABLE (Part 4)
| Feature | Exudative RD | Tractional RD | Rhegmatogenous RD |
|---|---|---|---|
| Mechanism | BRB breakdown / RPE pump failure | Fibrovascular membrane contraction | Liquefied vitreous through retinal break |
| Retinal breaks | Absent | Absent (present in TRD-RRD) | Present (defining feature) |
| Retinal shape | Convex, smooth, dome-like | Concave, tent-shaped, taut | Convex, corrugated, opaque |
| Shifting fluid | Present (pathognomonic) | Absent | Absent |
| Retinal mobility | High, undulates freely | Severely reduced, tethered | High, undulates freely |
| Photopsia | Absent | Absent | Present (vitreoretinal traction) |
| Tobacco dust (Shafer's sign) | Absent | Absent | Present (pathognomonic) |
| Floaters | If vitritis present | If VH from NVs | Acute shower (VH or PVD fibres) |
| Onset | Variable (acute in VKH; gradual in tumours) | Gradual, insidious | Acute (hours to days) |
| IOP in affected eye | Normal/variable | Normal/variable | Low (or high in Schwartz-Matsuo) |
| Bilateral | Often (VKH, HTN, metastases) | Rarely | Rarely (10-15% fellow eye risk) |
| B-scan | Smooth dome; T-sign; choroidal mass | Concave, immobile retina; adherent hyaloid; FVMs | Highly mobile membrane; open anteriorly; no adherent hyaloid |
| OCT | SRF without breaks; choroidal thickening | ERMs; traction bands; macular SRF | SRF under macula; break at outer retina; photoreceptor disruption |
| FA | Pinpoint RPE leaks (VKH); hot spot (CSC) | NVD/NVE; ischaemia | Not usually diagnostic; may show vascular changes at break margins |
| Tobacco dust | Absent | Absent | Present |
| Main causes | Tumours, VKH, scleritis, CSC, HTN | PDR, ROP, trauma, FEVR, sickle cell | PVD, myopia, lattice degeneration, trauma, post-cataract |
| Treatment | Treat underlying cause (NO surgery) | Pars plana vitrectomy + pre-op anti-VEGF | PR / Scleral buckle / PPV + retinopexy + tamponade |
| Prognosis | Good if cause treated early | Guarded; depends on macula | Excellent if macula-on; guarded if macula-off >1 month |
MISSING SPECIFIC DETAILS WITHIN EXISTING SECTIONS
Gap 1 - VKH Section (Section 2.3B): Missing Detailed Management
- Specific diagnostic workup before starting treatment: lumbar puncture is required when diagnosis is uncertain (CSF shows transient lymphocytic pleocytosis + melanin-containing macrophages in VKH). HLA-DR4/DRw53 typing is supportive but not diagnostic alone
- Exact steroid dosing protocol: IV methylprednisolone 500-1000 mg/day for 3 days, then oral prednisolone 1-2 mg/kg/day (maximum 60-80 mg/day), tapered over 3-6 months minimum - NOT over 6-12 months as stated in the treatment section (the 3-6 month taper applies; longer courses for refractory disease)
- Steroid-sparing agents with doses: azathioprine 1-2 mg/kg/day, mycophenolate mofetil 1-1.5 g twice daily, cyclosporine 3-5 mg/kg/day
- Biological agents - infliximab: Should be introduced early in steroid-resistant disease, not after multiple failed agents. Typical dose: 5 mg/kg IV at weeks 0, 2, 6, then every 8 weeks
- Monitoring for recurrence: Recurrent anterior uveitis occurs in up to 50-70% of cases in the chronic recurrent phase. Sunset glow fundus appearance indicates quiescent choroidal depigmentation - RPE window defects on FA confirm past damage
- Topical therapy: Topical corticosteroids (prednisolone acetate 1% hourly initially) + cycloplegics (atropine 1% or cyclopentolate 1%) for anterior segment involvement - prevent posterior synechiae
- Imaging-guided tapering: OCT-guided tapering is recommended - taper steroids only when OCT shows complete SRF resolution. Premature tapering is the most common cause of flare
Gap 2 - Choroidal Melanoma Section (Section 2.3A): Missing Detailed Workup
- Differential diagnosis from choroidal nevus: The critical distinction using the TFSOM-DIM mnemonic (Thickness >2 mm, Fluid subretinal, Symptoms, Orange pigment, Melanoma-hollow, Diameter >5 mm) - if 4+ factors present, >50% chance of melanoma. This is the most important clinical tool and is entirely absent
- PAX8 immunocytochemistry: Melanoma and melanocytoma are PAX8-negative; pigmented adenocarcinoma is PAX8-positive - useful when diagnosis uncertain after biopsy
- Genetic profiling: BAP1 mutation (~50% of uveal melanomas) = higher metastatic risk; chromosome 3 monosomy (M3) + chromosome 8q gain together = worst prognosis; Liverpool Uveal Melanoma Prognosticator (LUMPO) online tool for individualised survival prediction
- Follow-up for choroidal nevus: Low-risk nevus: annual dilated exam; high-risk nevus (TFSOM-DIM 3+ factors): every 3-6 months with OCT, AF, and US
- Histological cell types: Spindle cell (better prognosis, arranged in bundles), epithelioid cell (larger, more pleomorphic, higher mitotic rate, worse prognosis), mixed type
- Systemic surveillance intensity based on genetic profile: low-risk chromosomal profile allows reduced surveillance; high-risk profile (M3, BAP1+) warrants 6-monthly liver ultrasound
Gap 3 - Diabetic Retinopathy Section: Entirely Missing
- DR Classification table (ETDRS): No DR → Very mild NPDR → Mild NPDR → Moderate NPDR → Severe NPDR (4-2-1 rule) → PDR → High-risk PDR → Advanced diabetic eye disease, with monitoring intervals for each
- The 4-2-1 rule for severe NPDR: Haemorrhages in 4 quadrants OR venous beading in 2+ quadrants OR IRMA in 1+ quadrant = severe NPDR → 3-4 month review, consider PRP
- CSMO criteria (Clinically Significant Macular Oedema - ETDRS definition): retinal thickening within 500 μm of fovea centre; hard exudates within 500 μm with adjacent thickening; retinal thickening ≥1 disc area within 1 disc diameter of fovea
- Pregnancy monitoring table: Gestational diabetes (no risk), no/minimal NPDR (1st + 3rd trimester), mild-moderate NPDR (every trimester), high-risk NPDR/PDR (monthly)
- First-line treatment for centre-involving DME: Anti-VEGF (ranibizumab, aflibercept, bevacizumab, faricimab) - this is entirely absent from the document
- Indications for vitrectomy in DME: dense non-clearing VH, macular TRD, ERM/VMT, premacular haemorrhage, chronic DME unresponsive to other treatment
- Systemic risk factor modification: The document mentions PDR as a cause of TRD but never mentions that tight glycaemic control (HbA1c target <7%), blood pressure control, and lipid management are the most important factors in DR prevention and post-surgical TRD recurrence prevention
MISSING FROM PARTS 5 AND 6
Gap 4 - Key Trials: Missing RRD Trial Evidence
- PIVOT Trial and SPR Study (Scleral Buckling versus Primary Vitrectomy in Rhegmatogenous Retinal Detachment): Multicenter RCT comparing scleral buckle vs PPV for primary RRD in phakic and pseudophakic eyes. Key finding: No significant difference in anatomical reattachment or BCVA at 2 years overall; but scleral buckle showed advantage in phakic patients (avoids vitrectomy-induced cataract), while PPV showed advantage in pseudophakic patients with posterior breaks
- DIODE RCT (Pneumatic Retinopexy vs Vitrectomy - PIVOT trial, JAMA 2019, PMID 31050750): Pneumatic retinopexy achieved non-inferior BCVA outcomes vs PPV for primary RRD with breaks in the superior 8 clock hours, with fewer re-operations than vitrectomy at 12 months. Single-operation success rate: 81% for PR vs 80% for PPV - re-establishing pneumatic retinopexy as a valid primary treatment option
Gap 5 - Recent Advances: Missing RRD and PVR Advances
- Wide-field imaging for RRD break detection: Optomap ultra-wide field (200°) fundus photography now detects peripheral breaks not visible on standard 45° fundus photography. Studies show up to 15% of breaks in RRD are detected only on wide-field imaging, missed by standard photography
- PVR pharmacotherapy - anti-PVR adjuvants: Intraocular 5-fluorouracil + low molecular weight heparin (LMWH) in the irrigation fluid during PPV for PVR reduces RPE cell proliferation intraoperatively; evidence from the Silicone Study. Emerging: intravitreal methotrexate and anti-PDGF agents under investigation for PVR prevention
- Subretinal tissue plasminogen activator (tPA) displacement for submacular haemorrhage associated with RRD from giant retinal tears causing submacular blood
- OCT-guided timing of RRD surgery: Swept-source OCT now identifies early subfoveal SRF in supposedly "macula-on" RRDs, reclassifying them as macula-threatened and urgently escalating surgical timing
MISSING FROM MNEMONICS SECTION (Part 8)
- B - Break in the full-thickness retina (defining feature)
- R - Red horseshoe/U-tear visible on indirect ophthalmoscopy
- E - Emergency if macula-on (repair within 24-48 hours)
- A - Acute photopsia + floaters + tobacco dust = PVD with break
- K - Kanski: "Always examine the fellow eye - bilateral risk in myopia, Stickler, lattice"
Summary Table of All Gaps
| Gap | Location | What's Missing | Severity |
|---|---|---|---|
| No RRD chapter | Major structural gap | Full section on RRD pathogenesis, risk factors, symptoms, signs, investigations, surgery | Critical |
| Three-way comparison table | Part 4 | RRD column in the exudative vs tractional table | Critical |
| VKH detailed management | Section 2.3B | LP workup, exact steroid doses, infliximab dosing, monitoring, imaging-guided tapering | Significant |
| Melanoma workup | Section 2.3A | TFSOM-DIM mnemonic, PAX8, genetic profiling, LUMPO tool, nevus follow-up schedule | Significant |
| DR monitoring chapter | Entirely absent | Full ETDRS classification, monitoring intervals, CSMO criteria, pregnancy table, anti-VEGF for DME, systemic targets | Critical |
| RRD clinical trials | Part 5 | PIVOT trial (PR vs PPV), SPR Study (SB vs PPV) | Significant |
| RRD surgical advances | Part 6 | Wide-field imaging for break detection, PVR pharmacotherapy, OCT-guided timing | Moderate |
| RRD mnemonic | Part 8 | No mnemonic for the most common RD type | Minor |
i don't need RRD, only ERD, TRD and combined TRD and RRD, so what are missing in the word file? detailed evaluation and add the contents to the word file but write it in chat no need for pdf or file from top to bottom everything
Complete Gap Analysis + Missing Content: ERD.docx (ERD = Exudative + Tractional + Combined TRD-RRD)
SCOPE CONFIRMED FROM THE DOCUMENT
- Part 1: Foundations
- Part 2: Exudative (Serous) RD
- Part 3: Tractional RD
- Part 4: Comparison Table (Exudative vs Tractional only)
- Part 5: Key Clinical Trials
- Part 6: Recent Advances
- Part 7: Prognosis
- Part 8: Mnemonics
IDENTIFIED GAPS - IN ORDER OF APPEARANCE
GAP 1 - Part 1.3 (Classification Table): Combined TRD-RRD Missing as a Fourth Type
| Type | Mechanism | Retinal Breaks |
|---|---|---|
| Rhegmatogenous RD | Full-thickness retinal break allows liquefied vitreous to pass beneath the retina | Present (tear or hole) |
| Tractional RD | Fibrovascular membranes pull the retina away from the RPE mechanically | Absent (primary) |
| Exudative (Serous) RD | Fluid leaks from abnormal vessels or RPE failure accumulates under the retina | Absent |
| Combined Tractional-Rhegmatogenous RD | Fibrovascular traction creates a full-thickness retinal break; the RD then acquires rhegmatogenous characteristics and progresses rapidly | Present (secondary, traction-induced) |
Teaching point: Combined TRD-RRD is the most surgically urgent non-exudative RD. When traction creates a full-thickness break in a previously pure tractional detachment, the slow, contained progression of TRD suddenly converts to the rapid, expanding behaviour of rhegmatogenous RD. This transformation is recognised clinically by sudden acceleration of the detachment and on B-scan by increased retinal mobility at the break site. It significantly escalates surgical urgency and complexity.
GAP 2 - Part 2.3B (VKH): Shallow Clinical Description - Missing Detailed Staging, Diagnostic Criteria, and Full Workup
- No history of penetrating ocular trauma or surgery preceding the initial uveitis onset
- No clinical or laboratory evidence of other ocular disease
- Bilateral uveitis (anterior granulomatous uveitis, or panuveitis with multifocal serous retinal detachments)
- Neurological/auditory findings: meningismus, tinnitus, CSF pleocytosis, encephalopathy, cranial nerve palsies
- Dermatological findings occurring after ocular/CNS onset: alopecia, poliosis (premature whitening of lashes/brows/hair), vitiligo
- OCT (most useful): Subretinal fluid with characteristic septae dividing the fluid into compartments. Height of subretinal fluid on OCT correlates with disease activity. EDI-OCT shows subfoveal choroidal thickening >500 μm in active disease. OCT is used to guide steroid taper - fluid must be fully resolved before dose reduction
- Fluorescein Angiography (FA): Acute uveitic phase - multiple early hyperfluorescent pinpoint leaks at RPE level (due to focal RPE breakdown), then late pooling of dye within serous detachment areas. Chronic/convalescent phase - RPE window defects from depigmentation
- Fundus Autofluorescence (FAF): Hyperautofluorescence in areas of active serous detachment. Important non-invasive monitoring tool for disease activity
- ICGA: More sensitive than FA for choroidal involvement. Shows multiple hypofluorescent dark spots (stromal hypofluorescence) in active disease, corresponding to choroidal inflammatory infiltrates. Spots resolve with treatment - ICGA is the most sensitive tool for detecting subclinical active disease
- B-scan ultrasonography: Diffuse choroidal thickening; confirms/excludes posterior scleritis as differential; UBM (ultrasound biomicroscopy) can demonstrate ciliary effusion and forward rotation of the iris-lens diaphragm
- Lumbar puncture: When diagnosis is uncertain. CSF shows transient lymphocytic pleocytosis and melanin-containing macrophages. Normal LP does not exclude VKH
- HLA typing: HLA-DR1 and HLA-DR4 support the diagnosis across racial groups; HLA-DRw53 also associated. Not diagnostic alone
- Systemic workup: FBC, ESR/CRP, LFTs, chest imaging (exclude sarcoidosis), audiogram (document hearing loss), dermatology review for vitiligo/poliosis
- IV methylprednisolone pulse: 500-1000 mg/day for 3 consecutive days (for severe exudative RD with significant bilateral serous detachments)
- Transition to oral prednisolone 1-2 mg/kg/day (maximum 60-80 mg/day) immediately after pulse
- Maintain high-dose for minimum 2-4 weeks until FA/OCT shows complete SRF resolution
- Taper by 10 mg decrements every 2-4 weeks from high dose, then 5 mg decrements below 20 mg/day
- Minimum total steroid course: 3-6 months for first episode; up to 12+ months for chronic recurrent disease
- Topical prednisolone acetate 1% (q1-2h initially, tapering) + cycloplegic (atropine 1% or cyclopentolate 1%) for anterior uveitis - prevents posterior synechiae
- Azathioprine: 1-2 mg/kg/day orally; onset 6-8 weeks; monitor FBC and LFTs monthly; check TPMT enzyme level before starting
- Mycophenolate mofetil (MMF): 1-1.5 g twice daily; preferred over azathioprine by many centres; better tolerated; similar efficacy
- Cyclosporine A: 3-5 mg/kg/day in 2 divided doses; monitor renal function and BP; risk of nephrotoxicity limits long-term use
- Methotrexate: 15-25 mg/week with folic acid 5 mg/week; commonly used in steroid-dependent VKH; monitor LFTs
- Infliximab (anti-TNF-α): 5 mg/kg IV at weeks 0, 2, 6, then every 8 weeks. Should be introduced early in steroid-resistant or rapidly relapsing disease - do not wait through multiple failed conventional immunosuppressants. Screen for latent TB before starting. Key: early escalation to infliximab in refractory VKH is now the recommended approach per Kanski's 10th edition
- Adalimumab: 40 mg SC every 2 weeks; alternative to infliximab; convenient subcutaneous route
- Rituximab: Anti-CD20 for refractory cases unresponsive to anti-TNF; limited evidence but case series support its use
- OCT at every follow-up visit to monitor SRF resolution - the only objective guide to taper
- FA every 3 months in active disease; ICGA if subclinical activity suspected despite apparent clinical improvement
- IOP monitoring: glaucoma develops in 20-40% of chronic recurrent VKH; may require topical IOP-lowering therapy or trabeculectomy
- Slit-lamp exam at every visit: posterior synechiae, cataract development, KPs
- Long-term complications to monitor: subretinal neovascularization (CNV), subretinal fibrosis, neovascular glaucoma, tractional changes from chronic inflammation
GAP 3 - Part 2.3A (Choroidal Melanoma): Missing Nevus vs Melanoma Distinction, Full Workup, Genetic Analysis, and Follow-up Schedule
- Flat or minimally elevated (<2 mm thick)
- Well-circumscribed grey-brown pigmented lesion
- Usually <5 mm in diameter
- Overlying drusen (which increase with age)
- T - Thickness >2 mm (B-scan ultrasound)
- F - Fluid subretinal (OCT)
- S - Symptoms: visual loss, VA <20/50 (Snellen)
- O - Orange pigment/hyperautofluorescence (fundus autofluorescence imaging)
- M - Melanoma hollow: low internal acoustic reflectivity (A-scan ultrasound)
- D - Diameter >5 mm (fundus photography)
- I - (Absence of drusen - absence of drusen on OCT increases risk)
- M - (Marginal location within 3 mm of disc or fovea)
Rule: If 4 or more TFSOM-DIM factors are present, the lesion has >50% chance of demonstrating growth and should be treated as a small choroidal melanoma.
- Complete dilated fundus examination with a 20-diopter indirect lens and Goldmann 3-mirror contact lens for detailed slit-lamp assessment; careful clinical drawing of size, shape, location, pigmentation, and relation to disc/fovea
- Baseline colour fundus photography and wide-field imaging - documents diameter for serial comparison; tracks growth
- OCT with Enhanced Depth Imaging (EDI-OCT) - measures tumour height; identifies subretinal fluid; assesses overlying retinal layers and photoreceptor integrity; choroidal structure beneath the lesion
- Fundus Autofluorescence (FAF) - documents orange pigment (lipofuscin = hyperautofluorescence); RPE disruption pattern; helps risk-stratify
- B-scan ultrasonography - measures tumour apical height (most accurate method); acoustic solidity: melanoma shows low internal reflectivity ("acoustic quietness"/"hollow") on A-scan, a key distinguishing feature from haemangioma (high reflectivity) and metastasis (variable)
- Fluorescein Angiography (FA) - melanoma shows "double circulation" (intrinsic tumour vasculature in arterial phase + late diffuse leakage); helps confirm vascularised lesion; orange pigment blocks background fluorescence
- Indocyanine Green Angiography (ICGA) - hypofluorescent throughout the study (ICG does not accumulate in melanoma vasculature); better defines tumour borders with less RPE interference than FA; most useful for diffuse melanomas
- MRI with gadolinium - T1 hyperintensity (due to melanin paramagnetic effect), T2 hypointense; used to confirm extraocular extension/orbital invasion; helps differentiate from subretinal haemorrhage; useful when ultrasound is equivocal
- Fine needle aspiration biopsy (FNAB) or 25G vitrectomy-assisted biopsy - when diagnosis cannot be established by non-invasive means; provides tissue for histopathology and genetic analysis
- Immunocytochemistry - PAX8 staining on biopsy material: melanoma and melanocytoma are PAX8-negative; pigmented adenocarcinoma of the RPE is PAX8-positive - critical distinction with overlapping histological features
- Systemic metastatic staging:
- Liver function tests (LFTs) + liver ultrasound - the liver is the primary site of uveal melanoma metastasis; these are the mainstay of surveillance
- Chest X-ray (rarely positive without liver disease; low yield as first-line)
- Whole-body PET-CT - greater sensitivity for extrahepatic metastases particularly in bone and lung; reserved for high-risk cases (M3, BAP1+); involves significant radiation dose
- Chromosome 3 monosomy (M3): Loss of one copy of chromosome 3; present in ~50% of uveal melanomas; strongly correlates with metastatic risk
- Chromosome 8q gain (i8q): Amplification of 8q; when combined with M3 = worst prognosis group (5-year metastatic rate >70%)
- BAP1 mutation: Tumour suppressor gene on chromosome 3p; somatic mutation in ~50% of uveal melanomas; BAP1-mutated tumours = higher epithelioid cell content + significantly increased metastatic risk; germline BAP1 mutations also exist (BAP1 tumour predisposition syndrome)
- Chromosome 6p gain: Associated with spindle cell histology and low metastatic risk
- Gene expression profiling (GEP): Class 1A/1B (low risk) vs Class 2 (high risk) - high sensitivity and specificity for metastatic risk prediction
- Liverpool Uveal Melanoma Prognosticator (LUMPO): Free online tool that combines tumour size, cell type, mitotic count, and genetic data to generate individualised 5- and 10-year survival estimates. Use for patient counselling and to guide surveillance intensity
| Risk Category | Criteria | Ocular Follow-up | Systemic Surveillance |
|---|---|---|---|
| Choroidal nevus - Low risk | 0-2 TFSOM-DIM factors, stable | Annual dilated exam | None |
| Choroidal nevus - High risk | 3+ TFSOM-DIM factors | Every 3-6 months with OCT, AF, US | Annual LFTs + liver US |
| Small melanoma (post-treatment, low-risk genetics) | Class 1A GEP / chromosome 6p gain / no M3 | Every 3-6 months | Annual LFTs + liver US |
| Small-medium melanoma (high-risk genetics) | M3 + i8q, BAP1+, Class 2 GEP | Every 3-6 months | Every 6 months: LFTs, liver US; annual PET-CT or MRI liver |
| Post-enucleation | Any | Annual | Every 6 months: LFTs, liver US |
GAP 4 - Part 2.3 (Section 2.3B): Sympathetic Ophthalmia - Missing Workup and Management Details
- Identical immunosuppressive strategy to VKH: IV methylprednisolone pulse → oral prednisolone 1-2 mg/kg/day → slow taper over 6-12 months
- Steroid-sparing: azathioprine or MMF added early in refractory or chronic cases
- The exciting eye (injured eye): Enucleation of the injured eye within 2 weeks of injury before sympathetic ophthalmia develops may prevent the condition. However, once sympathetic ophthalmia is established, enucleation of the exciting eye does NOT prevent progression in the sympathising eye and is generally avoided (the exciting eye may ultimately have better vision)
- Long-term monitoring for cataract, glaucoma, and subretinal neovascularization - same as VKH
- Prognosis: with aggressive therapy, 75% of sympathising eyes retain VA better than 6/60; relapses occur in 50% of cases and may be delayed for years
GAP 5 - Part 2.3C (Posterior Scleritis): Missing Systemic Associations and Complete Workup
- B-scan ultrasound: T-sign (pathognomonic) - fluid in Tenon's capsule creates a dark anechoic triangle posterior to the globe at the optic nerve insertion; choroidal thickening also visible
- MRI orbit with gadolinium: Scleral enhancement; T2 hypointensity of the inflamed sclera; orbital fat infiltration; excludes posterior uveal tumour
- FA: Disc leakage, multiple pinpoint RPE leaks, late subretinal pooling - similar to VKH; distinguishable by clinical context (pain, T-sign)
- Systemic workup: FBC, ESR/CRP, ANA, ANCA (Wegener's/GPA), RF (rheumatoid arthritis), HLA-B27 (spondyloarthropathy), VDRL + FTA-ABS (syphilis), ACE + chest CXR (sarcoidosis), complement levels (SLE)
- Rheumatology referral: Mandatory - up to 50% of posterior scleritis cases are associated with systemic autoimmune disease
- Rheumatoid arthritis (most common)
- Systemic lupus erythematosus (SLE)
- Granulomatosis with polyangiitis (formerly Wegener's)
- Relapsing polychondritis
- Ankylosing spondylitis / spondyloarthropathy
- Inflammatory bowel disease (Crohn's, UC)
- Polyarteritis nodosa
- Herpes zoster (infectious posterior scleritis)
- NSAIDs (indometacin 100 mg/day or flurbiprofen 300 mg/day) - for mild non-necrotising disease
- Oral prednisolone 1 mg/kg/day - for moderate-severe disease
- IV methylprednisolone for severe or necrotising disease
- Immunosuppressives (MMF, azathioprine, methotrexate) for recurrent/refractory or when underlying autoimmune disease requires disease-modifying therapy
- Biologics (rituximab for GPA-associated; infliximab for IBD-associated)
GAP 6 - Part 3 (Tractional RD): Missing Combined TRD-RRD as a Dedicated Subsection
- Pure TRD: slow, contained, anchored at traction points; SRF shallow; rarely extends to ora serrata
- Combined TRD-RRD: rapid progression; SRF extends anteriorly toward ora serrata; the detachment becomes bullous in the sector of the break; dramatically increased surgical urgency
- Proliferative Diabetic Retinopathy (PDR): Most common cause. Dense fibrovascular membranes at the NVD/NVE sites contract forcefully enough to avulse a full-thickness flap of retina, creating a traction tear
- Anti-VEGF crunch syndrome: VEGF withdrawal after injection causes rapid fibrous consolidation and contraction of pre-existing membranes, creating new traction tears - hence the 3-7 day window for vitrectomy
- Retinopathy of Prematurity (ROP): Stage 4b/5 - advancing fibrovascular ridge contraction creates peripheral breaks; transition from Stage 4 (partial TRD) to Stage 5 (total TRD/combined) can occur through break formation
- Penetrating trauma with proliferative vitreoretinopathy (PVR): Post-traumatic fibrocellular membranes cause traction tears in scarred retina
- Sickle cell retinopathy: Sea-fan fibrovascular fronds can create peripheral traction tears
| Feature | Pure TRD | Combined TRD-RRD |
|---|---|---|
| Progression rate | Slow, often stable for months | Rapid - hours to days |
| Retinal configuration | Concave, taut, contained | Bullous, balloon-like anteriorly in sector of break |
| SRF extent | Shallow; rarely reaches ora serrata | Extends to or near ora serrata |
| Retinal mobility | Severely reduced | Increased at the break site - the RRD component is mobile |
| B-scan | Incomplete, adherent hyaloid; concave immobile retina | Increased mobility of the detached retina at the break; adherent vitreous component remains |
| OCT | SRF under macula; epiretinal membranes | Break visible; SRF volume dramatically increased; rapid macular involvement |
| Surgical urgency | Urgent-elective (depending on macula) | Emergency |
Critical Clinical Rule: Any sudden acceleration of a previously stable TRD, sudden vision deterioration, or new bullous component in a known TRD patient should be assumed to be combined TRD-RRD until proven otherwise on B-scan. Surgical timing changes to emergency.
- B-scan ultrasonography (most important): Detects the break and the increased mobility component. The pure TRD shows an immobile concave retina; the combined type shows a zone of hypermobility at the break site with anterior SRF. Essential when VH obscures the fundal view (which is common in these eyes)
- Wide-field fundus photography/indirect ophthalmoscopy: To document the extent of the bullous RD and locate the break if visible
- OCT: Documents macular status - on or off; quantifies SRF; is the macula at acute risk?
- All standard TRD steps apply (core vitrectomy, PVD induction, membrane dissection, endolaser, tamponade)
- Additional requirement: The retinal break created by traction must be identified, surrounded by endolaser, and adequately tamponaded to seal it (treating both the tractional and rhegmatogenous components simultaneously)
- PFCL (perfluorocarbon liquid): More commonly required in combined TRD-RRD than pure TRD because the mobile bullous RD must be flattened before membrane dissection can proceed safely. PFCL is injected into the vitreous cavity to hydraulically flatten the retina, allowing membrane peeling on a stable surface
- Relaxing retinotomies: May be required when the retina is foreshortened (PVR component) and cannot reach the RPE even after membrane removal; a circumferential incision through the retina allows it to unfold and flatten
- Retinal tamponade choice:
- Gas (C₃F₈ 14-16%): For combined TRD-RRD where the break is in the upper retina and the retina can be fully reattached; absorbed over 6-8 weeks
- Silicone oil (1000-5000 cSt): Preferred for: inferior breaks, PVR-associated cases, patients who cannot maintain positioning, poor compliance patients, or cases with high re-detachment risk. Must be removed at 3-6 months; risk of band keratopathy, glaucoma, and emulsification with long-term retention
- Scleral buckling as adjunct to PPV: Added when PVR is present or peripheral traction cannot be fully relieved by vitrectomy alone; supports the retinal break from the outside and provides additional vitreous base support
- Pre-operative anti-VEGF remains beneficial for the active neovascular component
- However, if the combined TRD-RRD developed because of anti-VEGF crunch (membrane contraction after delayed surgery), the treating surgeon must be prepared for aggressive intraoperative membrane dissection - the membranes will be denser and more fibrotic than in a primary case
- Worse than pure TRD because of: larger SRF volume requiring reabsorption, higher PVR risk (break creation triggers RPE cell dispersal), greater retinal manipulation required intraoperatively
- Single-surgery anatomical reattachment: ~70-80% (vs 85-95% for pure TRD)
- PVR develops as a postoperative complication in 10-20% of combined TRD-RRD cases
- Visual outcome: primarily determined by duration of macular detachment; macula-off >2 weeks carries poor visual prognosis even after successful anatomical reattachment
- Re-operation rate: 15-25%
GAP 7 - Part 3.3 (TRD Aetiology): Missing Aetiology Subsection Depth
- Zone I: Posterior (worst prognosis if neovascularisation occurs here)
- Zone II: Mid-peripheral
- Zone III: Far peripheral (best prognosis)
- Stage 1: Demarcation line
- Stage 2: Ridge (elevated demarcation)
- Stage 3: Ridge with extraretinal fibrovascular proliferation
- Stage 4A: Partial TRD, macula-on
- Stage 4B: Partial TRD, macula-off
- Stage 5: Total TRD (funnel-shaped detachment)
- Type 1 ROP (treat): Zone I, any stage with plus disease; Zone I, Stage 3 (any); Zone II, Stage 2 or 3 with plus disease → laser photocoagulation to avascular retina + intravitreal anti-VEGF (bevacizumab or ranibizumab)
- Type 2 ROP (watch): Zone I, Stage 1 or 2 without plus; Zone II, Stage 3 without plus
- Stage 4-5 TRD: Vitrectomy (lens-sparing PPV for 4A; total PPV or scleral buckling for 4B/5); prognosis deteriorates sharply for Stage 5 (total TRD - often <10% chance of functional vision)
- Stage I: Peripheral arteriolar occlusion
- Stage II: Peripheral arteriovenous anastomoses
- Stage III: Neovascular/fibrovascular proliferations (sea fans)
- Stage IV: Vitreous haemorrhage
- Stage V: Tractional or rhegmatogenous retinal detachment
GAP 8 - Part 3.4 (TRD Investigations): Missing OCT-A Details and Rubeosis Assessment
- Rubeosis iridis (neovascularisation of the iris - NVI): Indicates severe, diffuse retinal ischaemia driving anterior segment neovascularisation. NVI/NVA (neovascularisation of the angle) heralds neovascular glaucoma (NVG) - the most serious long-term complication of PDR. Its presence: (1) signals extremely high VEGF burden, (2) indicates the retinal ischaemia is too severe for anti-VEGF alone to control, (3) is a poor prognostic sign for post-vitrectomy vision, and (4) mandates urgent combined treatment (anti-VEGF injection + PRP + vitrectomy)
- Gonioscopy: Mandatory when NVI is suspected to detect angle neovascularisation before IOP rises (NVG is often diagnosed late because patients feel no symptoms until the angle closes)
- Full-field ERG provides an objective measure of overall retinal function in TRD eyes
- Reduced b-wave amplitude indicates inner retinal ischaemia/dysfunction
- Severely attenuated ERG in a pre-surgical eye (particularly the b/a wave ratio) predicts poor visual outcome even after successful anatomical reattachment
- Particularly useful in eyes with dense VH where OCT cannot assess macular function
GAP 9 - Part 4 (Comparison Table): Missing Combined TRD-RRD Column
| Feature | Exudative RD | Tractional RD | Combined TRD-RRD |
|---|---|---|---|
| Mechanism | BRB breakdown / RPE pump failure | Fibrovascular membrane contraction | Traction creates full-thickness break → RRD superimposed |
| Retinal breaks | Absent | Absent | Present (traction-induced) |
| Retinal shape | Convex, smooth, dome-like | Concave, tent-shaped, taut | Bullous anteriorly (RRD component) + concave traction component |
| SRF extent | May extend to ora serrata | Shallow; rarely reaches ora serrata | Extends anteriorly toward ora serrata rapidly |
| Shifting fluid | Present (pathognomonic) | Absent | Absent |
| Retinal mobility | High, undulates freely | Severely reduced, tethered | Mixed - reduced at traction sites; increased mobility at break |
| Photopsia | Absent | Absent | Variable - may appear when break forms |
| Progression rate | Variable | Slow, months-years stable | Rapid - hours to days after break formation |
| Bilateral | Often (VKH, HTN, metastases) | Rarely (bilateral PDR) | Rarely |
| B-scan | Smooth dome; T-sign; choroidal mass | Adherent hyaloid; concave immobile retina; FVMs | Zone of increased mobility at break; FVMs; adherent hyaloid remaining |
| OCT | SRF without breaks; choroidal thickening | ERMs; traction bands; macular SRF | Break visible; large SRF volume; rapid macular involvement |
| FA | Pinpoint RPE leaks (VKH); hot spot (CSC) | NVD/NVE; ischaemia zones | NVD/NVE + break margins |
| Main causes | Tumours, VKH, scleritis, CSC, HTN | PDR, ROP, trauma, sickle cell, FEVR | PDR (crunch/advanced), ROP Stage 4B/5, trauma + PVR |
| Surgical urgency | Not surgical (treat cause) | Urgent-elective | Emergency |
| Treatment | Treat underlying cause (NO RD surgery) | PPV + pre-op anti-VEGF | Emergency PPV + PFCL + break sealing + endolaser + silicone oil/gas |
| Prognosis | Good if cause treated early | Guarded; depends on macula | Worse than pure TRD; high PVR risk; 15-25% re-operation |
GAP 10 - Part 5 (Key Trials): Missing VKH and Melanoma Trial Evidence
- Multiple retrospective studies consistently show that early, high-dose corticosteroids (initiated within 2 weeks of onset) are associated with significantly better visual outcomes and lower rates of chronic recurrent disease than delayed or low-dose treatment
- Key lesson: Delayed or inadequate initial treatment is the strongest predictor of development of chronic recurrent VKH, sunset glow fundus, and permanent vision loss
- The minimum recommended oral steroid course is 6 months for first-episode VKH - shorter courses lead to high relapse rates
- Several retrospective cohort studies (including Japanese multicentre data) show that early addition of azathioprine or MMF as a steroid-sparing agent from the outset (rather than waiting for steroid failure) reduces the cumulative steroid dose, minimises systemic side effects, and is associated with lower rates of chronic disease
- Anti-TNF biologics (infliximab, adalimumab): Multiple case series and a prospective observational study confirm rapid disease control in refractory VKH; infliximab shows faster SRF resolution on OCT than continued steroid escalation alone in steroid-resistant cases
- The COMS enrolled over 2,882 patients across three trials:
- Large tumour trial: Enucleation with vs without pre-enucleation external beam radiotherapy → no survival difference; pre-enucleation radiation not recommended
- Medium tumour trial: Iodine-125 brachytherapy vs enucleation → no significant difference in 5-year mortality (19% vs 18%); brachytherapy established as eye-sparing equivalent for medium tumours
- Small tumour observational study: Small melanomas (<3.1 mm apical height, <16 mm base) → 31% had growth at 5 years; COMS risk factors for growth overlap with TFSOM-DIM factors
- COMS long-term data: 10-year all-cause mortality 34% for medium tumours; liver metastasis accounts for the vast majority of deaths
GAP 11 - Part 6 (Recent Advances): Missing Specific ERD and Combined TRD-RRD Advances
- FDA-approved refillable ocular implant surgically inserted into the vitreous cavity; continuously delivers ranibizumab into the eye
- Refilled every 24 weeks in clinic (vs monthly intravitreal injections)
- ARCHWAY Phase 3 trial: Non-inferior to monthly ranibizumab for nAMD; refill success rate >98%
- Relevance to TRD/PDR: If validated in PDR trials, PDS could transform management by eliminating injection burden in patients requiring chronic anti-VEGF for PDR - the most common cause of TRD
- Current limitation: Surgical implantation risk including conjunctival erosion, endophthalmitis, and vitreous haemorrhage; not yet approved for PDR specifically
- Dexamethasone intravitreal implant (Ozurdex): 0.7 mg biodegradable implant; provides 3-4 months of anti-inflammatory and anti-exudative effect; used as adjunct when anti-VEGF alone inadequate for DME; useful post-vitrectomy where anti-VEGF injections can be technically difficult
- Fluocinolone acetonide implant (Iluvien): 0.19 mg; 36-month sustained release; FDA-approved for chronic DME; reduces injection frequency dramatically in pseudophakic patients; cataract and IOP elevation in phakic patients limits use
- Emerging intraoperative technique: during PPV for combined TRD-RRD with submacular haemorrhage (from NV bleeding at the break site), subretinal injection of tPA (0.5 mg/0.1 mL) + C₃F₈ gas bubble displaces submacular blood and potentially reduces photoreceptor damage
- Evidence from small case series and retrospective studies; being evaluated in prospective trials
- 3D digital visualisation platforms display the surgical field on a 4K 3D screen instead of through the eyepiece; surgeon looks at the screen rather than through the microscope
- Benefits: improved depth perception at low illumination (reduces phototoxic damage to the macula during long TRD cases), ergonomic operating position, teaching/sharing the view
- Increasingly adopted for complex TRD and combined TRD-RRD cases where operating time is prolonged
GAP 12 - Part 7 (Prognosis): Missing Combined TRD-RRD Prognosis Section
- Overall prognosis is worse than pure TRD due to the added rhegmatogenous component and its consequences
- Anatomical reattachment (single surgery): ~70-80%, compared to 85-95% for pure TRD; lower because of more complex membrane dissection requirements, break sealing challenge, and higher PVR incidence
- PVR as post-surgical complication: Develops in 10-20% of combined TRD-RRD cases, compared to 5-10% for pure TRD; RPE cells dispersed through the break during the rhegmatogenous phase proliferate post-operatively on the retinal surfaces
- Visual outcome: Critically dependent on three factors:
- Duration of macular detachment (same rules as pure TRD: <1 week = better chance; >6 months = very poor)
- Presence of PVR at surgery
- Pre-existing photoreceptor damage from chronic DR/ischaemia
- Re-detachment rate: 15-25%; primarily due to PVR; managed with re-vitrectomy + silicone oil in most cases
- Neovascular glaucoma: Highest risk in combined TRD-RRD from PDR (Cao et al. BMC Ophthalmol 2025, PMID 40155830) because: ischaemia is most severe, surgery is most extensive, and hypotony post-vitrectomy can paradoxically worsen NV angle disease
- Systemic control: HbA1c <7%, BP control, and nephrology co-management are the most important modifiable factors for preventing re-detachment and the fellow eye from progressing to the same stage
GAP 13 - Part 8 (Mnemonics): Missing Combined TRD-RRD Mnemonic and VKH Staging Mnemonic
- R - Rapid acceleration of a previously stable TRD = assume combined until proven otherwise
- A - Anti-VEGF crunch = break formation if vitrectomy delayed >14 days
- P - PFCL required - bullous RD must be flattened before membrane dissection
- I - Increased retinal mobility on B-scan at the break site (cf. pure TRD which is immobile)
- D - Dual treatment: seal the break AND peel the membranes in one operation
- P - Prodromal (meningism, tinnitus, headache)
- U - Uveitic (bilateral serous RD, granulomatous uveitis, papillitis)
- C - Convalescent (sunset glow fundus, vitiligo, poliosis, alopecia)
- C - Chronic recurrent (anterior uveitis, glaucoma, cataract, subretinal fibrosis)
If 4 or more factors: treat as small melanoma. If <4: high-risk nevus surveillance.
GAP 14 - References Section: Missing Citations for Added Content
-
Herbort CP Jr, et al. Modified criteria for the diagnosis of Vogt-Koyanagi-Harada disease. Jpn J Ophthalmol. 2020.
-
Shields CL, et al. Choroidal nevus transformation into melanoma: analysis of 2514 consecutive cases. Arch Ophthalmol. 2009;127(8):981-987.
-
Shields CL, et al. TFSOM-DIM: A new mnemonic for choroidal nevus. JAMA Ophthalmol. 2019.
-
Collaborative Ocular Melanoma Study Group. COMS randomized trial of iodine 125 brachytherapy for choroidal melanoma. Arch Ophthalmol. 2006;124(12):1684.
-
Yannuzzi LA, et al. Optic disc pit maculopathy. Trans Am Ophthalmol Soc. 1988.
-
International Classification of Retinopathy of Prematurity Revisited (ICROP3). Ophthalmology. 2021;128(10):e51-e68.
-
Goldberg MF. Classification and pathogenesis of proliferative sickle retinopathy. Am J Ophthalmol. 1971;71(3):649-665.
-
Campochiaro PA, et al. ARCHWAY: Port Delivery System with Ranibizumab for nAMD. Ophthalmology. 2022;129(3):295-307.
COMPLETE SUMMARY OF ALL GAPS
| # | Location | Gap | Priority |
|---|---|---|---|
| 1 | Part 1.3 Classification Table | Missing Combined TRD-RRD as 4th row with teaching note | Critical |
| 2 | Part 2.3B - VKH | Missing formal diagnostic criteria, full imaging protocol, complete management with doses, biologics, monitoring | Critical |
| 3 | Part 2.3A - Melanoma | Missing TFSOM-DIM mnemonic, full step-by-step workup, genetic analysis, PAX8, LUMPO, surveillance schedule | Critical |
| 4 | Part 2.3B - Sympathetic Ophthalmia | Missing management, enucleation timing principle | Significant |
| 5 | Part 2.3C - Posterior Scleritis | Missing full investigation list, systemic associations, complete treatment | Significant |
| 6 | Part 3 - TRD | Missing entire dedicated subsection on Combined TRD-RRD (definition, mechanism, recognition, B-scan features, surgical steps, prognosis) | Critical |
| 7 | Part 3.3 - TRD Aetiology | Missing ICROP classification for ROP, Goldberg classification for sickle cell, management thresholds | Moderate |
| 8 | Part 3.4 - TRD Investigations | Missing rubeosis/gonioscopy assessment, ERG role, anterior segment pre-surgical evaluation | Moderate |
| 9 | Part 4 - Comparison Table | Missing Combined TRD-RRD as third column | Critical |
| 10 | Part 5 - Trials | Missing VKH trial evidence, COMS expanded data | Moderate |
| 11 | Part 6 - Advances | Missing PDS/Susvimo, intravitreal steroid implants, subretinal tPA, heads-up 3D surgery | Moderate |
| 12 | Part 7 - Prognosis | Missing Combined TRD-RRD prognosis subsection | Significant |
| 13 | Part 8 - Mnemonics | Missing RAPID (combined TRD-RRD), PUCC (VKH phases), TFSOM-DIM cross-reference | Moderate |
| 14 | References | Missing 8 new citations for added content | Minor |
Search for latest anti-VEGF crunch syndrome prevention strategies
anti-VEGF crunch syndrome tractional retinal detachment prevention
anti-VEGF crunch syndrome prevention tractional retinal detachment 2024 2025
bevacizumab preoperative vitrectomy timing diabetic tractional retinal detachment
anti-VEGF injection contraction fibrovascular membrane retinal detachment
"crunch phenomenon" OR "anti-VEGF crunch" bevacizumab fibrovascular contraction PDR vitrectomy timing 2024 2025
crunch syndrome prevention anti-VEGF timing fibrovascular membrane PVD PDR
fibrovascular membrane fibrosis anti-VEGF PDR posterior vitreous detachment
preoperative anti-VEGF diabetic vitrectomy complications systematic review
anti-VEGF TRD progression risk factors worsening injection PDR
preoperative bevacizumab vitrectomy PDR TRD worsening
anti-VEGF proliferative diabetic retinopathy contraction traction retinal detachment risk
Anti-VEGF Crunch Syndrome: Latest Prevention Strategies (2023-2026)
What is Crunch Syndrome?
Updated Understanding of the Timeline (2025-2026 Data)
Zhao et al. (Clin Ophthalmol 2026, PMID: 41835291) - Prospective real-world study, 165 treatment-naïve PDR patients
- FVM angio-fibrotic switch occurred in 43% of all patients following anti-VEGF
- Median time to fibrosis (without TRD progression): 12 weeks (IQR 8-12 weeks)
- Median time to Crunch syndrome (with TRD progression): 12 weeks (IQR 4-14 weeks)
- Complete FVM separation from retina: median 13 months (IQR 6.8-19.6 months)
- These timelines are far later than the ~13 days reported in earlier studies
Strategy 1: The Surgical Timing Window (Strongest Evidence)
| Injection-to-Surgery Interval | Outcome |
|---|---|
| 1-3 days | Higher intraoperative bleeding (insufficient vascular regression) |
| 4-7 days | Lowest overall postoperative recurrence (VH + TRD) - optimal window |
| 8-14 days | Acceptable but increasing fibrotic changes |
| >14 days | Highest risk of TRD - membrane contraction fully established |
Strategy 2: PVD-Status Risk Stratification Before Injecting
Zhao et al. (Clin Ophthalmol 2026, PMID: 41835291)
| PVD Status | FVM Fibrosis Pattern | Crunch Risk | Surgery-Free Survival |
|---|---|---|---|
| Complete PVD | Predominantly fibrosis - FVM retracts away from retina | Low - fibrosis protective (HR=0.023) | 28.3 months (longest) |
| Partial PVD | Moderate fibrosis with variable retinal attachment | Intermediate | Intermediate |
| No PVD | Vitreoschisis; FVM remains adherent to retina | Highest - contraction directly transmitted | 3.2 months (p<0.0001 vs complete PVD) |
Strategy 3: Cumulative Dose Awareness
Tan et al. Systematic Review (referenced in Zhao et al. 2026)
- Multiple anti-VEGF injections are a significant independent risk factor for crunch syndrome
- Higher cumulative doses accelerate the angio-fibrotic switch
- Prevention implication: In eyes with active dense FVMs, avoid repeated injections without surgical follow-through. Anti-VEGF in this context should be injection-then-operate, not injection-then-observe-then-inject-again
Strategy 4: Biomarker-Guided Risk Stratification (Emerging, 2026)
Huang et al. (Invest Ophthalmol Vis Sci 2026, PMID: 42149029) - Multi-omics study, aqueous humor proteomics before and 7 days after aflibercept in PDR
- GALNS is elevated in PDR relative to controls but depleted in VH + TRD eyes and further declines post-treatment
- GALNS knockdown in fibroblasts upregulated α-SMA (myofibroblast marker) and collagen I, accelerated migration, and enhanced contractility
- Low GALNS = pro-fibrotic, pro-crunch state
Strategy 5: Surgical Decision-Making Framework (Practical Algorithm)
PDR eye with FVMs requiring anti-VEGF before vitrectomy:
│
├── Step 1: Assess PVD status (OCT + B-scan)
│ ├── Complete PVD → Anti-VEGF injection → Vitrectomy at 4-7 days ✓
│ ├── Partial PVD → Anti-VEGF injection → Vitrectomy at 4-7 days (urgent)
│ └── No PVD + Dense FVM → Consider PRIMARY vitrectomy without injection
│ OR injection with MANDATORY surgery at 4-7 days, no exceptions
│
├── Step 2: Count prior injections
│ ├── 0-1 prior injections → Proceed with standard protocol
│ └── 2+ prior injections with active FVMs → Escalate to surgery;
│ avoid repeated injection-only approach
│
├── Step 3: If injection given, confirm surgery date AT TIME OF INJECTION
│ (Not "schedule soon" - book the theatre slot the same day)
│
└── Step 4: Monitor at week 4, 8, 12 post-injection if surgery delayed
Specific attention to weeks 8-12 for delayed crunch
Strategy 6: Intraoperative Crunch Prevention
- Pre-fill PFCL (perfluorocarbon liquid) ready before membrane dissection begins - if a break is created during peeling, PFCL immediately stabilises the retina
- Start membrane dissection at the least adherent areas (peripheral NVE before central NVD) to relieve tension progressively
- Triamcinolone staining of vitreous to identify all hyaloid attachments before any traction is applied
- Use high-speed cutters (10,000 cpm) to minimise iatrogenic traction per cut cycle
- Have silicone oil ready as tamponade of choice if a traction tear is encountered intraoperatively (does not require postioning; suitable for complex combined TRD-RRD that develops on the table)
Strategy 7: What NOT to Do (Updated Evidence-Informed Guidance)
| Practice | Why it increases crunch risk |
|---|---|
| Injecting anti-VEGF and scheduling surgery "when available" | Delays beyond 14 days = highest TRD risk (Zhan et al. 2026) |
| Repeated injections in eyes with dense, adherent FVMs and no PVD | Cumulative fibrosis acceleration (Tan et al. systematic review) |
| Treating all PDR FVMs identically regardless of PVD status | No PVD = 9x shorter surgery-free survival (Zhao et al. 2026) |
| Using anti-VEGF as a substitute for timely vitrectomy in advanced PDR | Anti-VEGF does not reduce TRD risk independently - only facilitates safer surgery (Zhan et al. 2026) |
Summary Evidence Table
| Study | Design | Year | Key Finding for Crunch Prevention |
|---|---|---|---|
| Zhan et al. (PMID 41475681) | Retrospective cohort, 608 eyes | 2026 | 4-7 days optimal window; >14 days = highest TRD risk |
| Zhao et al. (PMID 41835291) | Prospective real-world, 165 patients | 2026 | PVD status determines crunch risk; complete PVD = protective; no PVD = 3.2 month surgery-free survival |
| Huang et al. (PMID 42149029) | Multi-omics, aqueous humor | 2026 | GALNS depletion = pro-fibrotic state; first validated biomarker for post-anti-VEGF fibrosis risk |
| Mikhail et al. (PMID 42219076) | Systematic review & meta-analysis, 834,814 injections | 2026 | TRD risk in severe PDR = 3.6% per injection (1 in 28) - disease-specific fibrovascular contraction; far exceeds general RRD risk of 0.012% |
| Pei et al. (PMID 36972566) | Systematic review & meta-analysis, 10 RCTs | 2023 | Pre-op anti-VEGF reduces surgical time, intraoperative bleeding, iatrogenic breaks, early POVCH, and postoperative RD |
| Samanta et al. (PMID 41817572) | Narrative review | 2026 | Comprehensive perioperative protocol; TRD progression as a specific listed adverse effect of anti-VEGF requiring timing vigilance |
| Dervenis et al. (PMID 37260074) | Cochrane, 28 RCTs | 2023 | Level 1 evidence for 3-7 day window; beyond 14 days increases combined TRD-RRD |
for the word document, give me the source of images from where should i put
Image Sourcing Guide for ERD.docx
PART 1: FOUNDATIONS
1.3 Classification Table
- Source: Kanski's Clinical Ophthalmology 10th Ed., Fig. 16.34 (tractional) + Fig. 16.35 (exudative) - your institutional library copy
- Alternative free source: EyeWiki AAO - Retinal Detachment - schematic diagrams free to use with attribution
- Placement: After the classification table, before Part 2
PART 2: EXUDATIVE RD
2.1-2.2 Pathophysiology / BRB
- Best source: Kanski's Clinical Ophthalmology 10th Ed., Chapter 13 (Diabetic Retinopathy) - Fig. 13.1 shows the normal retinal capillary bed including pericytes and endothelial cells
- Alternative: Ryan's Retina 6th Ed., Chapter 1 (Retinal anatomy) - BRB schematic
- Free alternative: Search "blood retinal barrier diagram" on BioRender.com (requires free account; publishable with attribution for educational use)
- Placement: Section 2.2, after the iBRB/oBRB bullet points
2.3A - Choroidal Melanoma
- Best source: Kanski's Clinical Ophthalmology 10th Ed., Fig. 20.26A-F (multiple views: grey-brown dome, amelanotic, juxtapapillary, orange pigment, SRF, exudative RD)
- Wills Eye Manual 7th Ed., Fig. 11.36.2 - clear colour fundus photo
- Free source: AAO ONE Network Image Library - search "choroidal melanoma" - public domain educational images available
- Placement: Under "Choroidal Melanoma" heading, before the mantra quote
- Source: Kanski's 10th Ed., Fig. 20.27 / 20.28 - B-scan + A-scan showing choroidal melanoma
- Free alternative: EyeRounds.org (University of Iowa) - search "choroidal melanoma ultrasound" - free open-access ophthalmic image atlas
- Placement: After the B-scan USG investigation bullet
- Best source: Shields CL et al. JAMA Ophthalmol 2019 - the original TFSOM-DIM paper includes an illustrated table; PMID 31145419 - request reprint or use figure with citation
- Free source: Create a simple comparison table in the document itself (no image needed); or use MedPix (NIH) - search "choroidal nevus vs melanoma"
- Placement: After the TFSOM-DIM mnemonic bullets, as a visual summary
2.3A - Choroidal Haemangioma
- Source: Kanski's Clinical Ophthalmology 10th Ed., Chapter 20 (Intraocular tumours) - circumscribed choroidal haemangioma figures
- Free source: EyeRounds.org - search "choroidal hemangioma" - open-access atlas
- Placement: Under "Choroidal Haemangioma" in Section 2.3A
2.3A - Choroidal Metastases
- Source: Kanski's Clinical Ophthalmology 10th Ed., Chapter 20 - choroidal metastasis figures
- Free source: MedPix NIH - search "choroidal metastasis" - NIH public domain
- Placement: Under "Choroidal Metastases" heading
2.3B - VKH Disease
- Source: Kanski's Clinical Ophthalmology 10th Ed., Fig. 12.17A + Fig. 12.18A (multifocal exudative RD in acute uveitic phase) - these are already in the textbook library at
/textbooks/9780443110993/ - Image URL from library:
https://cdn.orris.care/cdss_images/1d09b9a41b71ce9219c59fc4cd348baed3e0485edf22faf45f7d50fe2d9249f2.png - Placement: After the Uveitic stage bullet
- Source: Kanski's 10th Ed., Fig. 12.17B - sunset glow fundus
- Image URL from library:
https://cdn.orris.care/cdss_images/95bf0afa4e8ebf3dfb72d73793b0ac61ba7a0cfa6e194815f26f3f32c93039d1.png - Placement: After the Convalescent stage bullet
- Source: Kanski's 10th Ed., Fig. 12.18E/F - OCT of VKH showing subretinal septae
- Image URL from library:
https://cdn.orris.care/cdss_images/7965fc28ae37163337c65edd0d7cc278651c2db4171f0f4bc16e6031c56ca59c.png - Placement: Under Investigations - OCT bullet
- Source: Kanski's 10th Ed., Fig. 12.18C and D
- Image URLs from library:
- FA venous phase:
https://cdn.orris.care/cdss_images/94123a72612b82677b4257fb34b5cc2a95027cec6b0ed139b2323ed4400d1139.png - FA late pooling:
https://cdn.orris.care/cdss_images/eb47444ac641143b9b0d7e2fb8ef649539eb8f9be7eccb0bfdbf090765662daa.png
- FA venous phase:
- Placement: Under Investigations - FA bullet
2.3B - Posterior Scleritis
- Source: Kanski's Clinical Ophthalmology 10th Ed., posterior scleritis B-scan figures
- Free source: EyeRounds.org - search "posterior scleritis T-sign" - open access
- Wills Eye Manual 7th Ed. also has a T-sign B-scan illustration
- Placement: Under the posterior scleritis description, B-scan USG bullet
2.4 - Clinical Signs of Exudative RD
- Source: Wills Eye Manual 7th Ed., Fig. 11.3.4 (Exudative retinal detachment)
- Image URL from library:
https://cdn.orris.care/cdss_images/b49f86fe5e9d41d6506a28be69d47e37bbee0542ed40abc0af8aec3258fa6ef0.png - Placement: Under "Signs" - Convex retinal configuration bullet
- Free source: DRCR Retina Network public case images, or EyeRounds.org OCT gallery
- Placement: Under Investigations - OCT description
2.3C - Coats Disease
- Free source: EyeRounds.org - search "Coats disease" - extensive open-access gallery with fundus photos, FA, and B-scan
- Placement: Under "Coats Disease" description
2.3C - CSC (Central Serous Chorioretinopathy)
- Free source: EyeRounds.org - search "central serous chorioretinopathy"
- Alternative: Retina Image Bank (American Society of Retina Specialists) - free searchable image database; search "central serous" - images available with attribution
- Placement: Under CSC description in Section 2.3C
PART 3: TRACTIONAL RD
3.2 Pathogenesis
- Best source: Kanski's Clinical Ophthalmology 10th Ed., Chapter 13 - multiple diabetic retinopathy pathogenesis figures
- Free creative option: BioRender.com - free for educational non-commercial use; create a custom pathway diagram
- Placement: After the Step 1-6 pathogenesis description at the start of Section 3.2
- Source: Kanski's 10th Ed., Chapter 16 - TRD traction vector illustrations
- Free alternative: Ryan's Retina textbook figures (available via institutional library access)
- Placement: After the 3-vector traction bullet list
3.3 TRD Aetiology
- Source: Kanski's 10th Ed., Fig. 16.34A (TRD secondary to preretinal fibrosis)
- Image URL from library:
https://cdn.orris.care/cdss_images/ea090507b252d5b7bc84e9ff01f5b9e2a75e83d3306107e9c516d78afd9aff23.png - Placement: Under "Proliferative Diabetic Retinopathy" heading
- Source: Kanski's 10th Ed., Fig. 16.34 - classic concave TRD appearance
- Image URL from library:
https://cdn.orris.care/cdss_images/4ca2aead2683c7e38a37415f49ce1ce627c24998c99bf049814dd0040be0d334.png - Placement: Under Section 3.4 Signs - "Concave retinal configuration" heading
- Free source: EyeRounds.org - search "retinopathy of prematurity" - extensive ROP image gallery including stages 1-5
- Alternative: International Classification of ROP (ICROP3) paper figures - freely available supplemental figures
- Placement: Under ROP in Section 3.3
3.4 TRD Investigations
- Source: Kanski's 10th Ed., Fig. 16.34B - B-scan of TRD
- Image URL from library:
https://cdn.orris.care/cdss_images/f366730740d3a1a53a882416b1d39b4d9b33c965110cf82d71f13deeba14dcc5.png - Placement: Under B-scan Ultrasonography in investigations
- Free source: Retina Image Bank ASRS - search "tractional retinal detachment OCT" - open access with attribution
- Placement: Under OCT / Swept-Source OCT in investigations
- Free source: Retina Image Bank ASRS - search "proliferative diabetic retinopathy fluorescein angiography"
- Placement: Under FA in investigations
3.5 Surgical Management
- Free source: EyeWiki AAO - Pars Plana Vitrectomy - surgical technique diagrams
- Placement: At the start of Section 3.5 surgical management
- Source: Ryan's Retina 6th Ed. - surgical technique chapters with illustrated dissection techniques; institutional library
- Alternative free source: Published surgical technique papers with open-access figures (e.g., Chang et al. IOVS - search "diabetic TRD delamination segmentation")
- Placement: Under "Fibrovascular membrane dissection" in Section 3.5
- Free source: EyeRounds.org - search "silicone oil tamponade" or "gas tamponade"
- Placement: Under retinal tamponade section
3.6 Combined TRD-RRD (New Section)
- Free source: EyeRounds.org - search "combined tractional rhegmatogenous retinal detachment"
- Alternative: Retina Image Bank ASRS - search "combined TRD RRD"
- Placement: Under B-scan in the investigation bullet of Section 3.6
PART 4: COMPARISON TABLE
- Best source: Kanski's 10th Ed. - the chapter opening pages of Chapter 16 contain classification diagrams
- Free source: EyeWiki AAO - Retinal Detachment has a comparison schematic
- Placement: After the comparison table as a visual summary
PART 5 & 6: TRIALS AND RECENT ADVANCES
- Source: Gross JG et al. JAMA 2015 - Fig. 1 (VA over 2 years); available in the published paper via your institutional JAMA access, or via PubMed Central (freely available)
- Placement: Under DRCR Protocol S in Part 5
- Free source: Published iOCT studies are often open-access; search PubMed for "intraoperative OCT vitrectomy TRD" - several papers have freely available figures showing the iOCT screen
- Placement: Under intraoperative OCT in Section 6.1
FREE IMAGE DATABASES - QUICK REFERENCE
| Source | URL | Content | License |
|---|---|---|---|
| EyeRounds.org | eyerounds.org | Fundus photos, OCT, B-scan, FA, clinical photos - ophthalmic atlas | Free, open-access with attribution (University of Iowa) |
| Retina Image Bank (ASRS) | imagebank.asrs.org | Retinal specialist-level fundus, OCT-A, FA, surgical images | Free with free membership; attribution required |
| AAO ONE Network Image Library | aao.org/image-library | Broad ophthalmology - anterior + posterior segment | Free for educational use with attribution |
| MedPix (NIH) | medpix.nlm.nih.gov | All specialties including ophthalmology | US Government - public domain, free |
| BioRender | biorender.com | Create custom diagrams and pathways | Free for educational/non-commercial; paid for publication |
| Wikimedia Commons | commons.wikimedia.org | Open licensed medical images including eye images | CC-BY or public domain - check each image |
| PubMed Central (PMC) | pmc.ncbi.nlm.nih.gov | Open-access paper figures (CC-BY licensed) | Free to use with citation of the paper |
TEXTBOOK FIGURES ALREADY IN THE LIBRARY
| Figure | Textbook | Chapter | Document Section |
|---|---|---|---|
| Fig. 12.17A/B | Kanski's 10th Ed. | Uveitis | VKH acute + convalescent |
| Fig. 12.18A-F | Kanski's 10th Ed. | Uveitis | VKH imaging (FAF, FA, OCT) |
| Fig. 13.1 | Kanski's 10th Ed. | Diabetic Retinopathy | BRB / capillary pathology |
| Fig. 16.34A/B | Kanski's 10th Ed. | Retinal Detachment | TRD signs + B-scan |
| Fig. 16.35A/B | Kanski's 10th Ed. | Retinal Detachment | Exudative RD shifting fluid |
| Fig. 20.25 A-C | Kanski's 10th Ed. | Intraocular Tumours | Melanoma histology |
| Fig. 20.26 A-F | Kanski's 10th Ed. | Intraocular Tumours | Melanoma fundus appearances |
| Fig. 20.28 A-D | Kanski's 10th Ed. | Intraocular Tumours | Melanoma investigations (FA, ICGA, US, MRI) |
| Fig. 11.36.1 | Wills Eye Manual 7th | Chapter 11 | Choroidal nevus |
| Fig. 11.36.2 | Wills Eye Manual 7th | Chapter 11 | Choroidal melanoma |
| Fig. 11.3.4 | Wills Eye Manual 7th | Chapter 11 | Exudative RD |
All Kanski's and Wills Eye Manual figures are available through institutional library access (Elsevier/Lippincott). For personal educational documents, figures can be used with the textbook citation noted beneath each image.
Create custom diagnostic pathway diagrams using BioRender for VKH stages and TRD pathogenesis
Diagram 1 - VKH Disease: Diagnostic Pathway and Clinical Stages
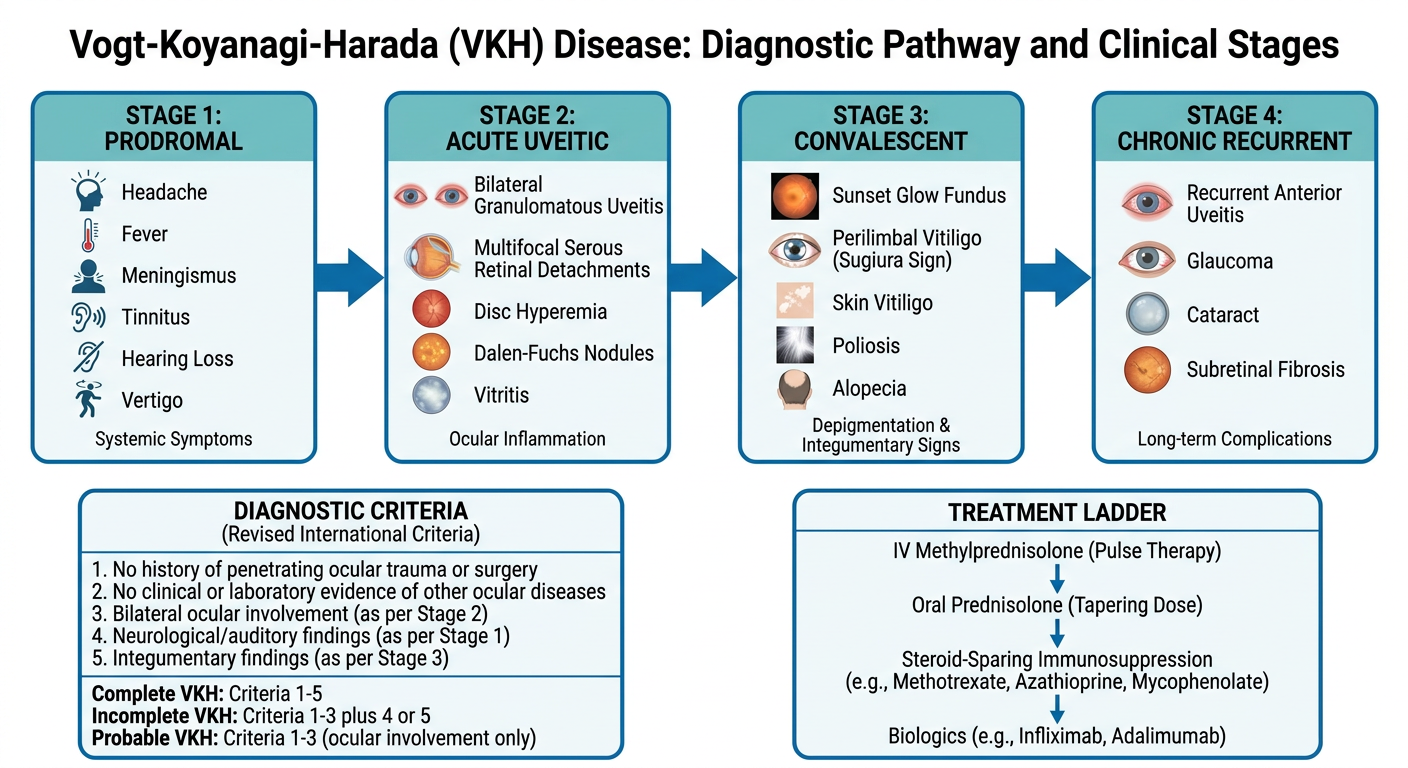
Diagram 2 - TRD Pathogenesis: 6-Step Cascade in PDR
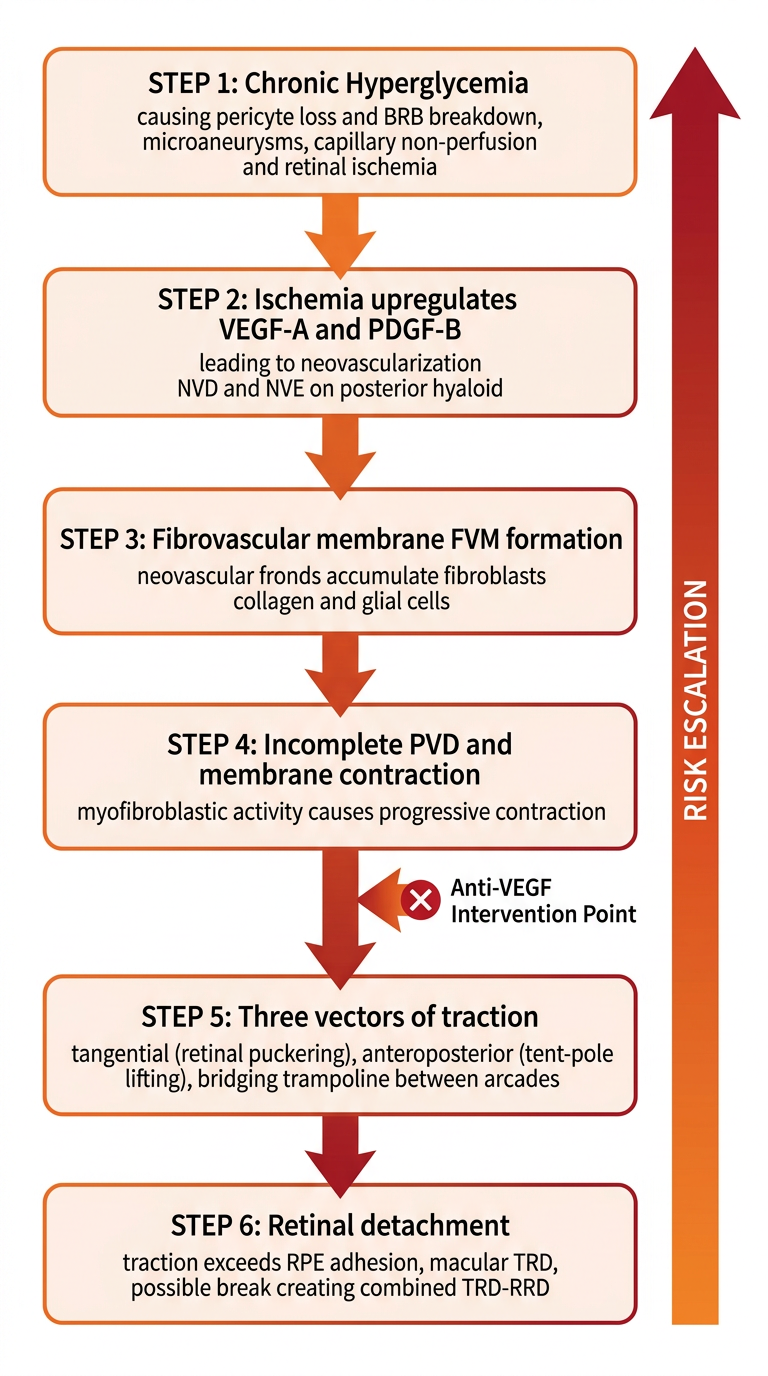
- Right-click each image above → Save image as
- In Word: Insert → Pictures → This Device → select the saved file
- Right-click the inserted image → Wrap Text → Top and Bottom (for clean positioning below headings)
- Add caption beneath each: "Figure X. [Title]. Created for educational purposes."