CKD
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Here is a comprehensive, exam-focused overview of CKD — its definition, classification, and staging per current KDIGO guidelines.
Chronic Kidney Disease (CKD) — Overview, Classification & Staging
Definition
CKD is defined as abnormalities of kidney structure or function, present for >3 months, with implications for health. Two criteria can each independently satisfy the diagnosis:
| Criterion | Threshold |
|---|---|
| Decreased GFR | eGFR < 60 mL/min/1.73 m² |
| Markers of kidney damage | Albuminuria (ACR ≥30 mg/g), abnormal urine sediment, electrolyte abnormalities, structural abnormalities on imaging, history of kidney transplantation |
Key exam point: G1 or G2 with A1 (eGFR ≥60 and ACR <30 mg/g) does not meet CKD criteria unless there is additional evidence of kidney damage. The 3-month duration requirement distinguishes CKD from AKI.
— Brenner and Rector's The Kidney, Comprehensive Clinical Nephrology 7th Ed.
KDIGO CGA Classification System (2012)
The current system uses 3 dimensions: Cause + GFR category + Albuminuria category.
G Stages — GFR Categories
| Stage | Description | eGFR (mL/min/1.73 m²) |
|---|---|---|
| G1 | Normal or high | ≥90 |
| G2 | Mildly decreased | 60–89 |
| G3a | Mildly to moderately decreased | 45–59 |
| G3b | Moderately to severely decreased | 30–44 |
| G4 | Severely decreased | 15–29 |
| G5 | Kidney failure | <15 (or on KRT) |
A Stages — Albuminuria Categories (urine ACR)
| Stage | Description | ACR (mg/g) | ACR (mg/mmol) |
|---|---|---|---|
| A1 | Normal to mildly increased | <30 | <3 |
| A2 | Moderately increased | 30–300 | 3–30 |
| A3 | Severely increased | >300 | >30 |
KDIGO Heat Map — CGA Classification Diagram
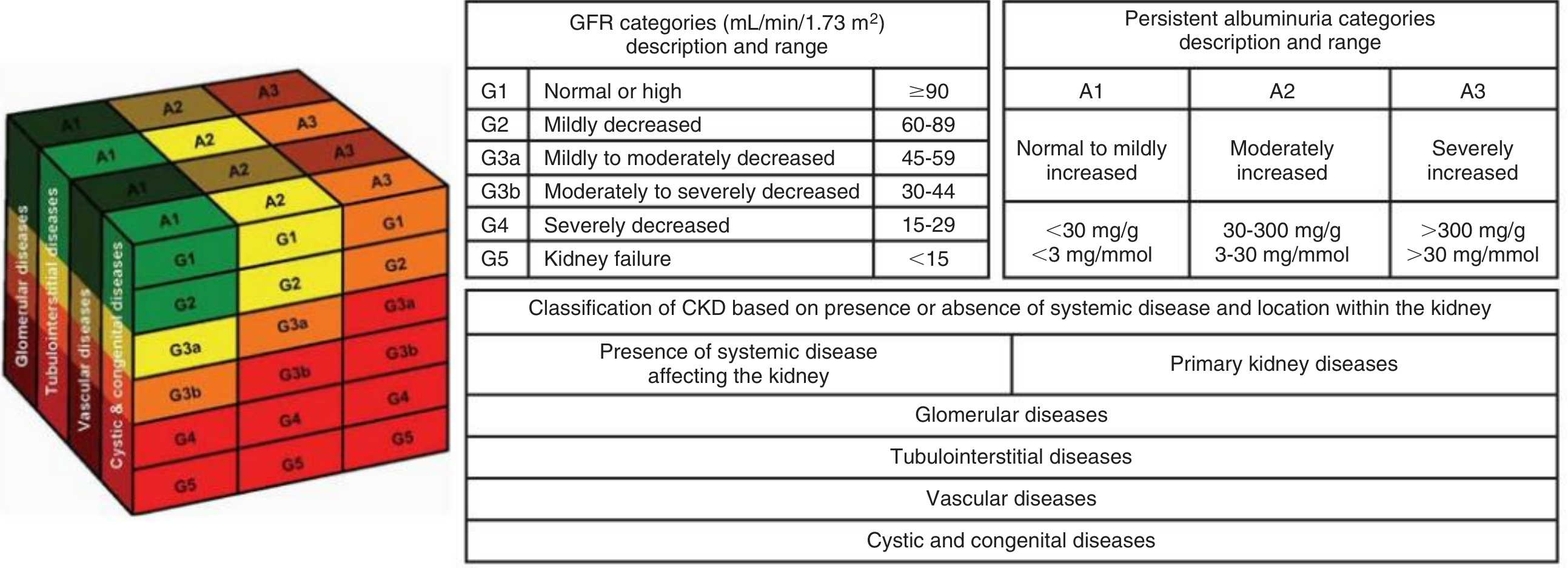
The color-coded cube (green → yellow → orange → red) reflects increasing risk of progression to kidney failure as GFR falls and albuminuria rises.
Monitoring Frequency by Stage
Numbers in the heat map below indicate recommended nephrology follow-up visits per year:
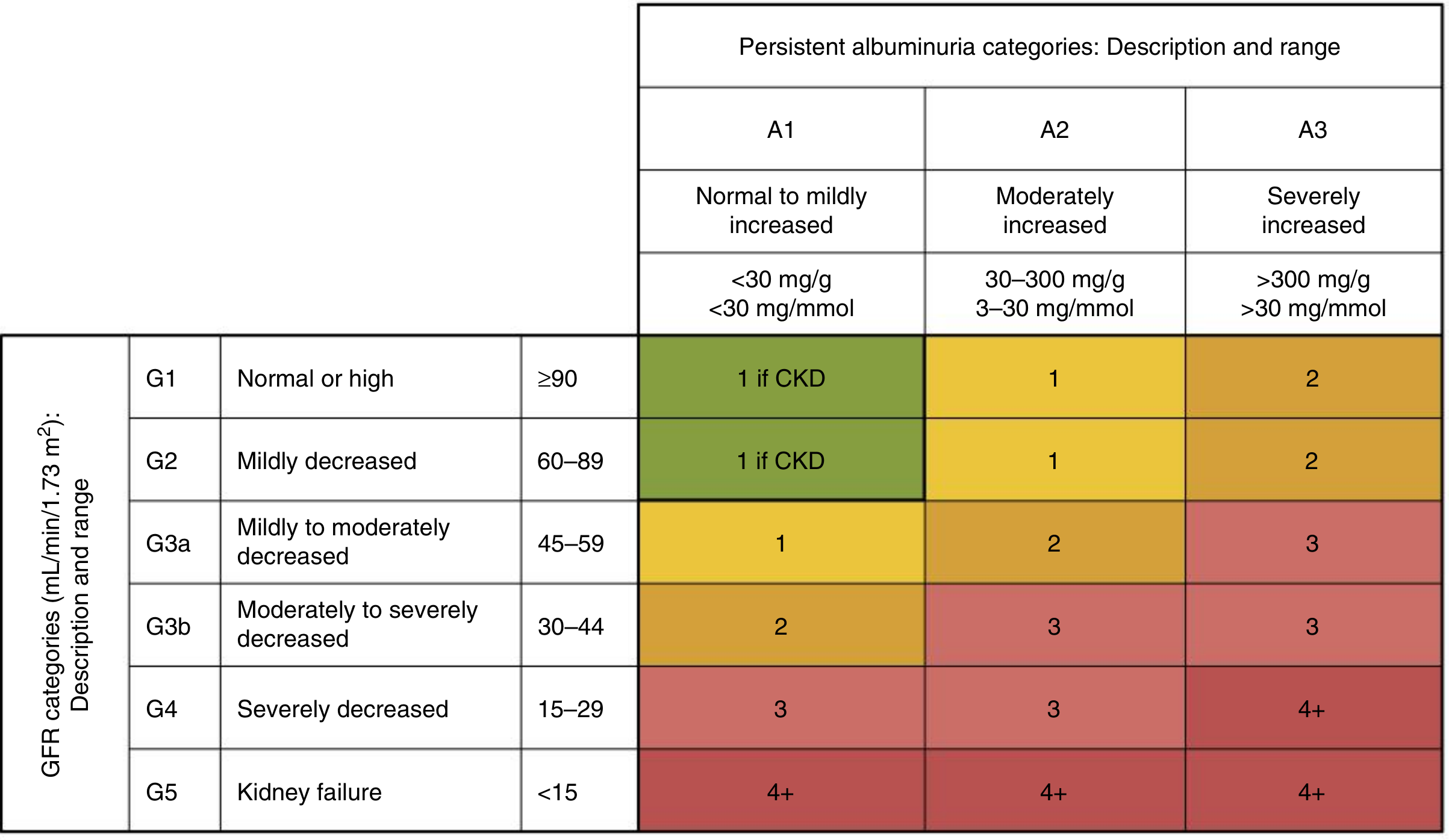
G5/A3 patients require 4+ visits per year. G1–G2/A1 with confirmed CKD require 1 visit/year.
GFR Estimation Equations
Two main equations to know for exams:
| Equation | Formula | Notes |
|---|---|---|
| CKD-EPI | Uses creatinine ± cystatin C, age, sex | Most accurate; preferred in North America |
| Cockcroft-Gault | (140 − Age) × Weight / (72 × SCr) × 0.85 (if female) | Estimates CrCl, not GFR; used for drug dosing |
| MDRD | 1.86 × (SCr)^−1.154 × (Age)^−0.203 | Older; underestimates at higher GFR values |
Cause Classification ("C" in CGA)
KDIGO categorizes cause by:
- Presence/absence of systemic disease (e.g., diabetes, lupus, amyloid)
- Location of pathologic abnormality within the kidney:
- Glomerular diseases
- Tubulointerstitial diseases
- Vascular diseases
- Cystic & congenital diseases
Most Common Causes (Adults)
- Diabetic nephropathy — #1 cause of ESKD worldwide
- Hypertensive nephrosclerosis — #2
- Glomerulonephritis (IgA nephropathy, FSGS, membranous, lupus nephritis)
- Polycystic kidney disease (ADPKD)
- Chronic obstruction / reflux nephropathy
Clinical Progression Notes
- Patients are typically asymptomatic until late G4–G5
- Complications (anemia, MBD, secondary hyperparathyroidism, hypertension) often begin at G3
- Dialysis planning should start at G4; initiation based solely on a target GFR has not shown mortality benefit — symptoms and metabolic/nutritional status guide timing
- Half of all Americans are expected to develop CKD during their lifetime
— Comprehensive Clinical Nephrology 7th Ed., Washington Manual of Medical Therapeutics, Brenner & Rector's The Kidney
High-yield exam summary:
CKD = ↓eGFR (<60) or kidney damage markers, for >3 months. Stage with G (1–5) + A (1–3). Cause is the "C." Most common cause = diabetes. Complications emerge at G3; dialysis planned at G4.
This is a shared conversation. Sign in to Orris to start your own chat.