I am orthopaedics pg trainee. I have my university exams in two months, so what was the topic name? I am giving just try to go through the standard textbooks, recent articles and classic articles and make a proper notes which should include all the images, low chart tables and it should be easy to do revision. Feed this to your memory. So whenever I give this topic name you make me complete notes over it and end give me 10 MCQ’s questions on that topic so that I can prepare for my fellowship exam simultaneously. After preparing the whole notes, make a poster visual poster. Also, it should be like visual mind map, including all the details and important summary and also at the same time images.
Your Orthopaedics PG Study Protocol
| Component | Details |
|---|---|
| Notes | From standard textbooks (Campbell's, Apley's, Miller's, etc.) |
| Images | Anatomy diagrams, X-rays, MRI, classification tables, implant photos |
| Flowcharts | Decision algorithms, management protocols |
| Tables | Classifications, comparison tables, surgical approaches |
| Recent evidence | PubMed - last 2-3 years, meta-analyses, RCTs |
| Classic articles | Landmark papers that defined the topic |
| MCQs | 10 questions - mix of DNB/MS and Fellowship level |
| Visual Poster | Mind map with images, key points, and summary |
- "Tibial plateau fractures"
- "Rotator cuff tears"
- "Developmental dysplasia of hip"
- "Spine - lumbar disc prolapse"
Give me notes on my first ortho exam topic
ddh
"developmental dysplasia of the hip"[MeSH Terms]
DDH developmental dysplasia hip classic landmark articles Pavlik harness Salter osteotomy review
Graf classification DDH ultrasound alpha beta angle types table 2024
mkdir -p /home/daytona/workspace/ddh-notes && ls /home/daytona/workspace/ddh-not…
~/ddh-notes/create_ddh_notes.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
HeadingLevel, AlignmentType, BorderStyle, WidthType, ShadingType,
VerticalAlign, PageBreak, UnderlineType
} = require('docx');
const fs = require('fs');
// Helper: heading
const H1 = (text) => new Paragraph({
text, heading: HeadingLevel.HEADING_1,
spacing: { before: 360, after: 120 }
});
const H2 = (text) => new Paragraph({
text, heading: HeadingLevel.HEADING_2,
spacing: { before: 240, after: 80 }
});
const H3 = (text) => new Paragraph({
text, heading: HeadingLevel.HEADING_3,
spacing: { before: 180, after: 60 }
});
const P = (text, bold=false, color=undefined) => new Paragraph({
children: [new TextRun({ text, bold, color })],
spacing: { before: 60, after: 60 }
});
const bullet = (text, bold=false, level=0) => new Paragraph({
children: [new TextRun({ text, bold })],
bullet: { level },
spacing: { before: 40, after: 40 }
});
const divider = () => new Paragraph({
children: [new TextRun({ text: '─'.repeat(80), color: '999999' })],
spacing: { before: 120, after: 120 }
});
const pageBreak = () => new Paragraph({ children: [new PageBreak()] });
// Colored highlight para
const highlight = (text, color='FFD700') => new Paragraph({
children: [new TextRun({ text, bold: true })],
shading: { type: ShadingType.CLEAR, fill: color },
spacing: { before: 80, after: 80 },
indent: { left: 200 }
});
// Table builder
function makeTable(headers, rows, headerColor = '1F4E79') {
const headerRow = new TableRow({
children: headers.map(h => new TableCell({
children: [new Paragraph({ children: [new TextRun({ text: h, bold: true, color: 'FFFFFF' })], alignment: AlignmentType.CENTER })],
shading: { type: ShadingType.CLEAR, fill: headerColor },
verticalAlign: VerticalAlign.CENTER
}))
});
const dataRows = rows.map(row => new TableRow({
children: row.map((cell, i) => new TableCell({
children: [new Paragraph({ children: [new TextRun({ text: String(cell) })], alignment: AlignmentType.CENTER })],
shading: { type: ShadingType.CLEAR, fill: i === 0 ? 'D6E4F0' : 'FFFFFF' }
}))
}));
return new Table({
rows: [headerRow, ...dataRows],
width: { size: 100, type: WidthType.PERCENTAGE }
});
}
const doc = new Document({
title: 'DDH - Developmental Dysplasia of Hip - Comprehensive Notes',
sections: [{
children: [
// TITLE
new Paragraph({
children: [new TextRun({ text: 'DEVELOPMENTAL DYSPLASIA OF THE HIP (DDH)', bold: true, size: 48, color: '1F4E79' })],
alignment: AlignmentType.CENTER,
spacing: { before: 400, after: 200 }
}),
new Paragraph({
children: [new TextRun({ text: 'Comprehensive PG Orthopaedics Study Notes | DNB / MS / Fellowship Level', color: '7F7F7F', size: 24 })],
alignment: AlignmentType.CENTER,
spacing: { after: 100 }
}),
new Paragraph({
children: [new TextRun({ text: 'Sources: Campbell\'s Orthopaedics 15e 2026 | Miller\'s Review 9e | Bailey & Love 28e | Grainger Radiology | PubMed 2023–2026', color: '7F7F7F', size: 20 })],
alignment: AlignmentType.CENTER,
spacing: { after: 400 }
}),
divider(),
// ─────────────────────────────────────────────────────────
H1('1. DEFINITION & SPECTRUM'),
P('DDH describes a spectrum of hip abnormalities including acetabular dysplasia, subluxation (partial dislocation), and complete dislocation of the femoral head from the true acetabulum.', false),
H3('Spectrum (Miller\'s):'),
bullet('Dysplasia — shallow acetabulum only'),
bullet('Subluxation — partial loss of contact between femoral head and acetabulum'),
bullet('Dislocation — complete loss of contact'),
bullet('Teratologic — dislocated in utero; irreducible; associated with arthrogryposis, Larsen syndrome'),
bullet('Late/adolescent dysplasia'),
P('', false),
highlight('KEY POINT: In a newborn with DDH, the femoral head can be reduced and dislocated. In older children, the head remains dislocated with secondary bony changes.', 'E8F4FD'),
// ─────────────────────────────────────────────────────────
pageBreak(),
H1('2. EPIDEMIOLOGY'),
makeTable(
['Parameter', 'Value'],
[
['Incidence (clinical exam)', '1–3 per 1000 live births'],
['Incidence (ultrasound screening)', 'Up to 25 per 1000'],
['True DDH on repeat US', '~5 per 1000'],
['Female : Male ratio', '5:1 (girls >> boys)'],
['Left hip vs Right hip', 'Left 67%, Right 20%, Bilateral 13%'],
['Breech DDH (female + breech)', '2.8% incidence'],
['Family history risk', '~10%; if parent + sib affected: ~36%'],
['UK incidence', '~1 in 400 live births'],
]
),
P('', false),
H3('Risk Factors (MNEMONIC: "FFOBB"):'),
bullet('F - Female sex (5× more common)', true),
bullet('F - Family history (10% risk)', true),
bullet('O - Oligohydramnios', true),
bullet('B - Breech presentation (especially frank breech, >30 weeks)', true),
bullet('B - Born firstborn (less intrauterine space)', true),
P('', false),
highlight('BOX: Other risk factors — Congenital muscular torticollis (8% co-occurrence), Metatarsus adductus (10%), Oligohydramnios. NO association with clubfoot.', 'FFF9C4'),
P('', false),
P('Racial variation: Higher in Navajo Indians and Lapps; lower in Chinese and Black populations. Swaddling with hips in extension increases risk.', false),
// ─────────────────────────────────────────────────────────
pageBreak(),
H1('3. PATHOANATOMY'),
H2('A. Normal Hip Development'),
bullet('Acetabulum forms from 3 parts of os coxae meeting at triradiate cartilage'),
bullet('Femoral head and acetabulum develop together — each requires the other for normal development'),
bullet('Ossific nucleus appears at 4–6 months of age'),
P('', false),
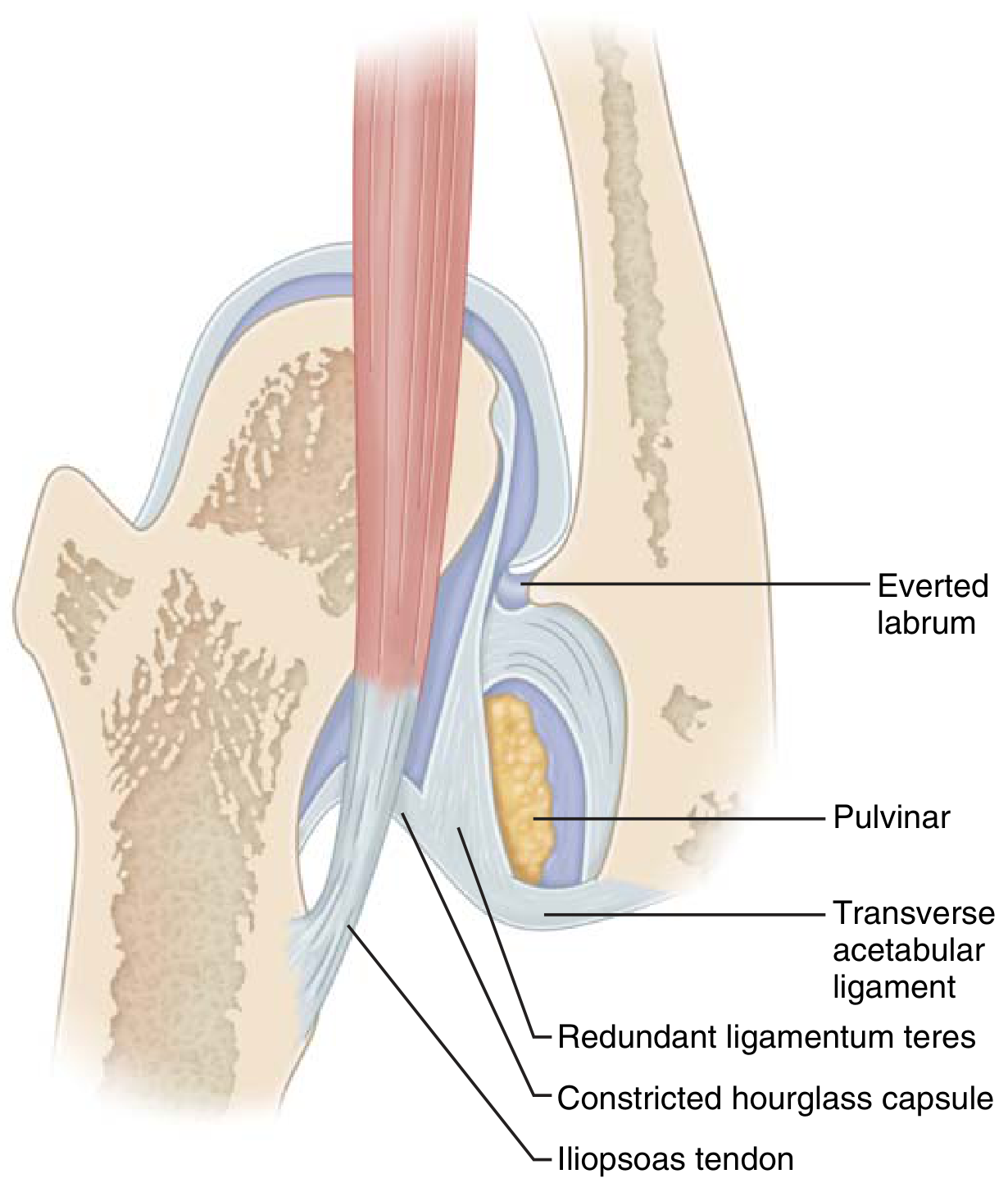
H2('B. Blocks to Reduction (CLASSIC LIST — HIGH YIELD!)'),
P('Image: Blocks to Reduction (Miller\'s Fig 3.4):', true),
makeTable(
['Block', 'Description'],
[
['Iliopsoas tendon', 'Constricts capsule in hourglass shape — most important block'],
['Pulvinar', 'Fibrofatty tissue filling the acetabulum'],
['Hypertrophied ligamentum teres', 'Takes up space in acetabulum'],
['Contracted inferomedial capsule', 'Hourglass constriction'],
['Transverse acetabular ligament', 'Narrows the acetabular opening'],
['Inverted/everted labrum', 'Limbus — inverted labrum blocks entry of femoral head'],
]
),
P('', false),
highlight('MNEMONIC for Blocks: "I PITCH" — Iliopsoas, Pulvinar, Inverted labrum, Transverse acetabular ligament, Capsule (hourglass), Hypertrophied ligamentum teres', 'E8F5E9'),
P('', false),
H2('C. Secondary Changes with Neglected DDH'),
bullet('Pseudoacetabulum forms superolaterally'),
bullet('True acetabulum remains underdeveloped and filled with pulvinar'),
bullet('Femoral neck: increased anteversion, coxa valga'),
bullet('Shortened limb, Trendelenburg gait, hyperlordosis'),
bullet('Adult: premature OA if untreated'),
// ─────────────────────────────────────────────────────────
pageBreak(),
H1('4. CLINICAL FEATURES BY AGE'),
H2('A. Neonatal Period (0–3 months)'),
makeTable(
['Test', 'How to Do It', 'What It Detects', 'Positive Finding'],
[
['Ortolani test', 'Flex hip 90°, abduct + lift greater trochanter anteriorly', 'Reduction of a dislocated hip', 'Palpable CLUNK of reduction (NOT a click)'],
['Barlow test', 'Flex hip 90°, adduct + push femoral head posteriorly', 'Dislocation of an unstable hip', 'Palpable CLUNK of dislocation'],
['Galeazzi sign', 'Flex both hips + knees, feet flat — compare knee heights', 'Shortened femur (proximal displacement)', 'Unequal knee heights (affected side lower)'],
['Restricted abduction', 'Compare abduction of both hips', 'Adductor contracture', '<45° or asymmetric'],
]
),
P('', false),
highlight('REMEMBER: Ortolani = "Out to In" (reduction). Barlow = "In to Out" (dislocation). Both become NEGATIVE as the hip stiffens with age.', 'FFE0E0'),
P('', false),
H2('B. 3–18 Months'),
bullet('Ortolani and Barlow become negative as contractures develop'),
bullet('Limited hip abduction — most reliable sign'),
bullet('Asymmetric skin folds — less reliable (normal children may have them)'),
bullet('Galeazzi sign positive (limb length discrepancy)'),
bullet('Delayed walking'),
P('', false),
H2('C. Walking Age (>18 months) and Older'),
bullet('Trendelenburg gait — abductor weakness on affected side'),
bullet('Hyperlordosis and pelvic tilt'),
bullet('Bilateral DDH: Waddling gait, hyperlordosis'),
bullet('Telescoping: ability to push femur in/out of pseudoacetabulum'),
bullet('Limb length discrepancy'),
// ─────────────────────────────────────────────────────────
pageBreak(),
H1('5. INVESTIGATIONS'),
H2('A. Ultrasound (Gold Standard <4–6 months)'),
P('Graf Method (Static Coronal View):'),
bullet('α (alpha) angle: measures BONY coverage of femoral head (bony acetabular roof)'),
bullet('β (beta) angle: measures CARTILAGINOUS coverage'),
P('', false),
makeTable(
['Graf Type', 'Alpha Angle', 'Beta Angle', 'Description', 'Treatment'],
[
['Type I', '≥ 60°', '< 55° (Ia) / >55° (Ib)', 'Normal mature hip', 'None needed'],
['Type IIa', '50–59°', '< 77°', 'Immature hip (<3 months) — physiological', 'Observe; Pavlik if not improving'],
['Type IIb', '50–59°', '< 77°', 'Immature hip (>3 months) — pathological', 'Pavlik harness'],
['Type IIc', '43–49°', '< 77°', 'Critically deficient bony roof; femoral head still centered', 'Pavlik harness'],
['Type D', '43–49°', '> 77°', 'Decentering — labrum displaced', 'Pavlik harness'],
['Type III', '< 43°', '> 77°', 'Eccentric/subluxated; labrum pressed upward', 'Pavlik / Closed reduction'],
['Type IV', '< 43°', 'Unmeasurable', 'Complete dislocation; labrum pressed downward', 'Closed/open reduction'],
]
),
P('', false),
highlight('KEY: α angle is the main determinant of type. β angle differentiates Ia/Ib and IIc/D. Normal α ≥ 60°.', 'E8F4FD'),
P('', false),
H2('B. Plain Radiography (>4 months when ossific nucleus appears)'),
makeTable(
['Radiological Line/Index', 'Description', 'Normal Value'],
[
['Hilgenreiner line (H-line)', 'Horizontal line through both triradiate cartilages', 'Reference line'],
['Perkin line (P-line)', 'Vertical line through lateral edge of acetabulum', 'Reference line'],
['Acetabular Index (AI)', 'Angle between H-line and acetabular roof line', '< 25° (varies with age)'],
['Shenton line', 'Curved line along inferior femoral neck and superior obturator foramen', 'Should be continuous arc'],
['Von Rosen line', 'X-ray with 45° abduction + medial rotation', 'Normal femoral line passes through acetabulum'],
['CE angle (Wiberg)', 'Center-edge angle — lateral coverage of femoral head', '> 25° (adult)'],
['Neck-shaft angle', 'Normal ~135°; DDH → coxa valga', 'Increased in DDH'],
]
),
P('', false),
P('In DDH: Femoral head ossific nucleus lies in OUTER LOWER quadrant (lateral to Perkin, below Hilgenreiner). Break in Shenton\'s line. Increased acetabular index.', false),
P('', false),
H2('C. CT / MRI'),
bullet('CT: Post-reduction assessment (especially in spica cast) — confirms concentricity'),
bullet('MRI: Best for pre- and post-operative assessment; no radiation'),
bullet('Arthrography: Intraoperatively — "thorn sign" = normal labral position; "rose thorn" = inverted labrum (abnormal)'),
// ─────────────────────────────────────────────────────────
pageBreak(),
H1('6. MANAGEMENT — AGE-BASED ALGORITHM'),
highlight('GOLDEN RULE: Earliest treatment = best outcome. Earlier diagnosis → simpler treatment.', 'E8F5E9'),
P('', false),
makeTable(
['Age Group', 'First-Line Treatment', 'If Fails / Alternative'],
[
['0–6 months', 'Pavlik Harness (success ~95% in dislocatable, ~80% in dislocated)', 'Abduction orthosis, then closed reduction'],
['6–18 months', 'Closed Reduction + Hip Spica Cast (under GA with arthrogram)', 'Open Reduction (anterior approach) + Spica'],
['18 months – 3 years', 'Open Reduction + Femoral Shortening ± Acetabular osteotomy', 'Femoral + pelvic combined procedure'],
['3–8 years', 'Open Reduction + Pelvic Osteotomy (Salter/Pemberton) + Femoral osteotomy', 'Salvage if congruence not achievable'],
['>8 years', 'Triple osteotomy (Steel/Tönnis) or Ganz PAO; controversial reduction', 'Chiari / shelf (salvage)'],
['Adult', 'Periacetabular osteotomy (Ganz PAO) if cartilage preserved', 'THA when OA develops'],
]
),
P('', false),
H2('A. Pavlik Harness (Detailed)'),
H3('Mechanism:'),
bullet('Maintains hip in ~100° flexion and MILD abduction ("human position" / "Salter position")'),
bullet('Prevents adduction and extension — these lead to dislocation'),
bullet('Hip must remain within Ramsey Safe Zone (between max adduction before redislocation and excessive abduction causing AVN)'),
P('', false),
H3('Protocol:'),
bullet('Worn 23 hours/day for at least 6 weeks after reduction achieved'),
bullet('Then part-time (nights + naps) for additional 6–8 weeks'),
bullet('Confirm reduction with ultrasound or X-ray after placement'),
P('', false),
H3('Risk factors for Pavlik Harness FAILURE:'),
bullet('Age >7 weeks at initiation of treatment'),
bullet('Bilateral dislocation'),
bullet('Absence of Ortolani sign (femoral head cannot be reduced)'),
P('', false),
H3('Complications:'),
bullet('"Pavlik Disease" — failed reduction attempts → erosion of posterior acetabular wall. If no reduction in 3 weeks, STOP harness.'),
bullet('AVN (Osteonecrosis) — from excessive abduction; posterosuperior retinacular branch of MFCA impinged'),
bullet('Femoral nerve palsy — from excessive flexion (>120°)'),
bullet('Skin pressure sores'),
P('', false),
highlight('CONTRAINDICATION: Pavlik harness is CONTRAINDICATED in Teratologic DDH.', 'FFE0E0'),
P('', false),
H2('B. Closed Reduction + Spica'),
bullet('Under GA: examination + arthrogram + reduction + hip spica cast'),
bullet('Arthrogram: "Thorn sign" = normal labrum (reduction adequate)'),
bullet('CT/MRI post-reduction to confirm concentricity'),
bullet('Safe zone of Ramsey must be verified'),
bullet('Pre-reduction traction: controversial; may decrease AVN risk'),
bullet('If narrow safe zone (<40°): adductor tenotomy before casting'),
P('', false),
H2('C. Open Reduction'),
makeTable(
['Approach', 'Age', 'Advantages', 'Disadvantages'],
[
['Medial (Ludloff)', '<12 months', 'Less blood loss; directly addresses obstacles; shorter scar', 'No capsulorrhaphy possible; higher AVN risk (near MFCA); no access for pelvic osteotomy'],
['Anterior (Smith-Peterson / bikini)', '>12 months (preferred)', 'Capsulorrhaphy possible; access for pelvic osteotomy; lower AVN risk', 'More dissection; longer scar'],
]
),
P('', false),
highlight('KEY: Anterior approach preferred >12 months (MFCA at risk with medial approach at older ages). Medial approach: up to 12 months only.', 'FFF9C4'),
P('', false),
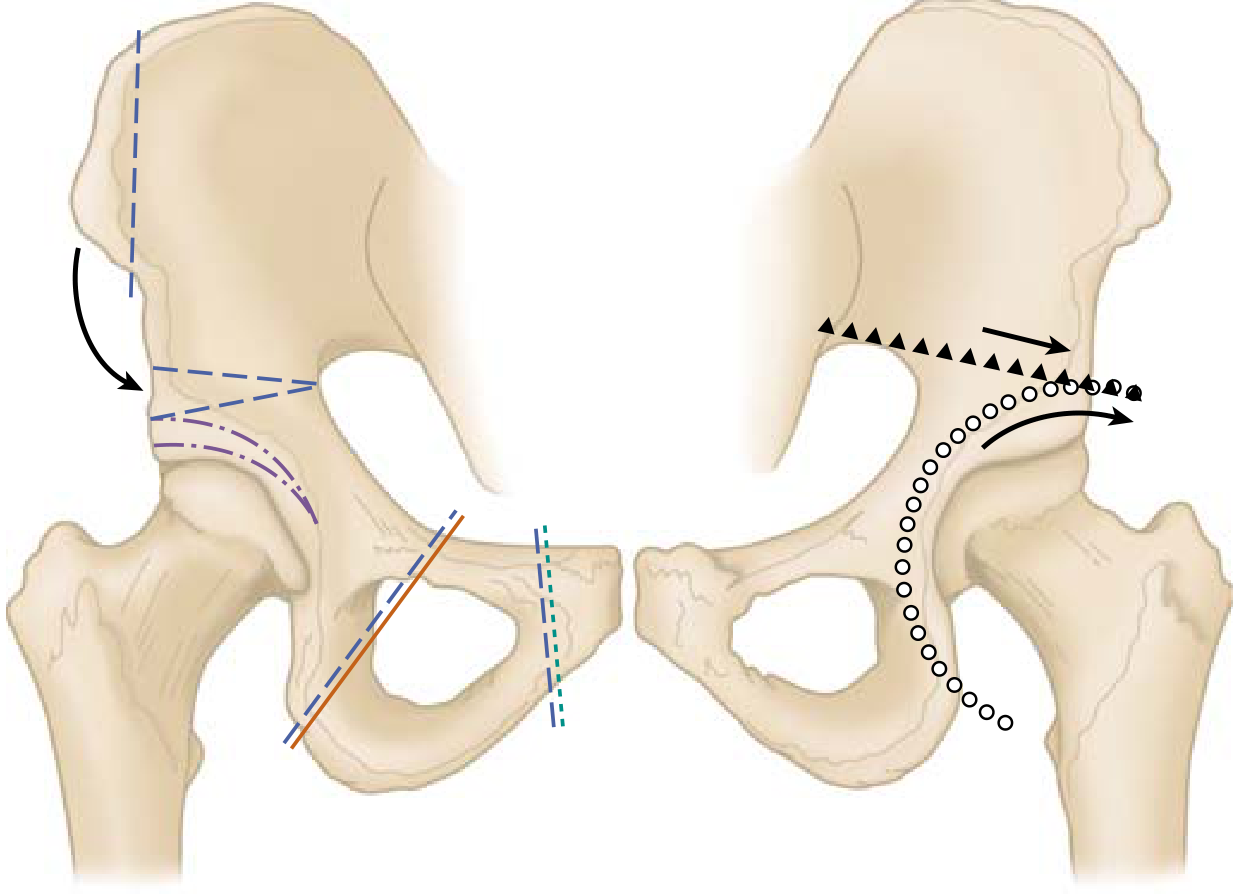
H2('D. Pelvic Osteotomies'),
makeTable(
['Osteotomy', 'Type', 'Age / Indication', 'Key Feature'],
[
['Salter Innominate', 'Redirectional (rotates acetabulum)', '<5–6 yrs, open triradiate; unilateral DDH', 'Redirects coverage anterolaterally; may lengthen limb 1 cm; iliac crest graft'],
['Pemberton', 'Reshaping (volume-reducing)', '<8 yrs, open triradiate', 'Hinges on triradiate cartilage; reduces acetabular volume; good for shallow acetabulum'],
['Dega', 'Reshaping/volume-reducing', 'Open triradiate; neuromuscular DDH', 'Posterior coverage; good for paralytic DDH'],
['Steel Triple', 'Redirectional (3 cuts)', 'Closed triradiate (>8 yrs)', 'Ischium + ilium + pubis cuts; full acetabular mobilization'],
['Sutherland Double', 'Redirectional', 'Older children', 'Salter cut + pubic osteotomy'],
['Tonnis Triple', 'Redirectional', 'Adolescents/adults', 'Alternative to Ganz; 3 cuts'],
['Ganz PAO', 'Periacetabular redirectional', 'Adults, closed triradiate; cartilage intact', '3D correction; preserves abductors; allows capsulotomy; immediate weight bearing possible'],
['Chiari', 'Salvage (medial displacement)', 'Any age; non-congruent joint', 'Medialization of femoral head; NOT reconstructive'],
['Shelf procedure', 'Salvage (adds bone to deficient roof)', 'Any age; non-congruent joint', 'Extra-articular; adds lateral coverage'],
]
),
P('', false),
H2('E. Femoral Osteotomy'),
bullet('Indicated when: marked anteversion, coxa valga, or to decompress after reduction'),
bullet('Femoral shortening (derotation varus osteotomy — DVRO): reduces tension on reduction; corrects anteversion + valgus'),
bullet('Especially required in older children (>18 months) to reduce pressure on femoral head'),
// ─────────────────────────────────────────────────────────
pageBreak(),
H1('7. COMPLICATIONS'),
makeTable(
['Complication', 'Mechanism', 'Prevention / Management'],
[
['Avascular Necrosis (AVN)', 'Most feared complication. Interruption of posterosuperior retinacular branch of MFCA. Causes: excessive abduction, forced reduction, vascular injury from medial approach', 'Stay within Ramsey safe zone; avoid extreme abduction; femoral shortening reduces tension; Kalamchi & MacEwen classification'],
['Residual Dysplasia', 'Acetabulum fails to remodel adequately after reduction', 'Acetabular index monitoring; pelvic osteotomy if AI >25° at age 2'],
['Redislocation', 'Inadequate soft tissue release; Inadequate capsulorrhaphy', 'Thorough obstacles release; capsulorrhaphy'],
['Stiffness / Limb shortening', 'Post-surgical fibrosis; premature growth arrest', 'Physiotherapy; monitoring'],
['Premature OA', 'Untreated or inadequately treated DDH', 'THA in adulthood'],
['"Pavlik Disease"', 'Erosion of posterior acetabular wall from failed Pavlik attempts', 'Stop harness if no reduction in 3 weeks'],
['Femoral nerve palsy', 'Excessive hip flexion in Pavlik (>120°)', 'Check flexion angle; usually transient'],
]
),
P('', false),
H3('Kalamchi & MacEwen Classification of AVN in DDH:'),
makeTable(
['Grade', 'Radiological Feature'],
[
['I (Most common)', 'Temporary growth irregularity of ossific nucleus; good prognosis'],
['II', 'Premature closure of lateral physis; progressive valgus deformity'],
['III', 'Premature closure of central physis; progressive valgus deformity'],
['IV (Most severe)', 'Total ischemic necrosis of femoral head; global collapse'],
]
),
P('', false),
// ─────────────────────────────────────────────────────────
pageBreak(),
H1('8. ADULT DDH'),
bullet('Untreated childhood DDH presents with early OA in 3rd–5th decade'),
bullet('Crowe classification used to grade severity of dislocation'),
P('', false),
makeTable(
['Crowe Class', 'Description', 'Proximal Femoral Head Migration'],
[
['I', 'Dysplastic hip; mild subluxation', '< 50% head diameter'],
['II', 'Subluxated', '50–75% head diameter'],
['III', 'Significantly subluxated', '75–100% head diameter'],
['IV', 'Completely dislocated', '> 100% — true dislocation'],
]
),
P('', false),
H3('THA in DDH — Key Considerations:'),
bullet('Small acetabular component (high-hip center vs. true acetabular center)'),
bullet('True acetabular center preferred (less stress, better biomechanics)'),
bullet('Femoral shortening osteotomy may be required for Crowe III/IV (risk of nerve palsy with lengthening)'),
bullet('Risk of dislocation increased in DDH THA — see recent meta-analysis (PMID: 37688602)'),
bullet('Nerve lengthening risk: sciatic nerve at risk if limb lengthened >4 cm'),
// ─────────────────────────────────────────────────────────
pageBreak(),
H1('9. RECENT EVIDENCE (2023–2026)'),
H3('Key Recent Studies:'),
makeTable(
['PMID', 'Study', 'Key Finding'],
[
['39853978', 'Tirta et al. JAMA Netw Open 2025 — Meta-analysis risk factors', 'Strongest pre-3-month risk factors: breech, female, family history (in that order)'],
['38053132', 'Huang et al. BMC Musculoskelet Disord 2023 — Environmental factors', 'Swaddling with hips in extension significantly increases DDH incidence'],
['37879719', 'Tao et al. BMJ Paediatrics Open 2023 — Prevalence meta-analysis', 'True prevalence 3.5/1000 by clinical exam; ultrasound detects much higher rates'],
['37688602', 'Shahbazi et al. Int Orthop 2023 — THA dislocation in DDH', 'Risk factors for THA dislocation in DDH: Crowe IV, smaller acetabular component, no dual-mobility cup'],
['39354451', 'Jacobsen et al. BMC 2024 — Genetics of DDH', 'GDF5, TGFB1, PAPPA2, and CX3CR1 genes implicated; polygenic inheritance'],
['41912496', 'Yoshino et al. Bone Res 2026 — Novel DDH genes', 'Novel genes including ALDH1A2 and BMP pathway genes identified'],
['40680148', 'Shanaa et al. JBJS Rev 2025 — Hip resurfacing in DDH', 'Hip resurfacing viable in selected DDH patients; higher complication rate vs standard THA'],
]
),
P('', false),
// ─────────────────────────────────────────────────────────
H1('10. CLASSIC LANDMARK ARTICLES'),
makeTable(
['Author / Year', 'Title / Contribution'],
[
['Ortolani (1937)', '"The Little-Known Hip Creak" — described the reduction click sign; basis for neonatal screening'],
['Barlow (1962)', 'Described the provocative dislocation test; British screening program basis'],
['Pavlik (1950, described; 1989 English)', 'Stirrups (Pavlik harness) method for functional reduction treatment of CDH'],
['Salter (1961)', 'Innominate osteotomy for DDH — redirectional pelvic osteotomy; landmark surgical technique'],
['Pemberton (1965)', 'Pericapsular osteotomy of ilium (Pemberton acetabuloplasty) — hinges on triradiate cartilage'],
['Wiberg (1939)', 'CE angle description — center-edge angle for measuring lateral acetabular coverage'],
['Graf (1980s)', 'Ultrasound classification system for infant hip — α and β angles; most widely used worldwide'],
['Ponseti & Frigerio (1950)', 'Natural history of CDH — importance of early treatment'],
['Thomas, Wedge, Salter (2007)', '45-year follow-up of open reduction + innominate osteotomy — excellent long-term outcomes'],
['Crowe et al.', 'Crowe classification of DDH for adult THA planning'],
['Kalamchi & MacEwen (1980)', 'Classification of avascular necrosis complicating treatment of DDH'],
]
),
P('', false),
// ─────────────────────────────────────────────────────────
pageBreak(),
H1('11. QUICK REVISION — HIGH-YIELD TABLES'),
H2('Summary Flowchart: Management by Age'),
makeTable(
['Age', 'Investigation', 'Treatment'],
[
['0–6 months', 'Ultrasound (Graf classification)', 'Pavlik harness (Graf IIb, IIc, D, III, IV)'],
['4–6 months', 'X-ray (when ossific nucleus appears)', 'Pavlik/abduction orthosis; closed reduction if failing'],
['6–18 months', 'X-ray + arthrogram (intraop)', 'Closed reduction + spica; open reduction if fails'],
['18 months – 3 yrs', 'X-ray + MRI', 'Open reduction (anterior) + femoral shortening ± pelvic osteotomy'],
['3–8 years', 'X-ray + CT/MRI', 'Open reduction + Salter/Pemberton + DVRO'],
['>8 years', 'X-ray + MRI', 'Triple osteotomy (Steel) or Ganz PAO; salvage (Chiari/shelf) if non-congruent'],
['Adult', 'X-ray + MRI', 'Ganz PAO (if cartilage intact); THA (when OA)'],
]
),
P('', false),
H2('Key Angle/Index Normal Values'),
makeTable(
['Parameter', 'Normal Value', 'Significance in DDH'],
[
['Acetabular Index (AI)', '< 25° at age 1', 'Increased AI = dysplasia; should normalize by age 2'],
['CE angle (Wiberg)', '> 25° (adult)', 'Decreased in lateral undercoverage'],
['Graf α angle', '≥ 60°', 'Normal bony coverage'],
['Graf β angle', '< 55° (type Ia)', 'Normal cartilaginous coverage'],
['Neck-shaft angle', '~135°', 'Increased in DDH (coxa valga)'],
['Anteversion', '~15–20° (normal)', 'Increased in DDH'],
['Acetabular anteversion', '~15–20° (normal)', 'May be abnormal in DDH'],
]
),
P('', false),
H2('Pelvic Osteotomy Memory Table'),
makeTable(
['Type', 'Procedure', 'Triradiate', 'Principle'],
[
['Redirectional', 'Salter, Steel, Tönnis, Ganz PAO', 'Open (Salter/Pemberton); Closed (Triple/Ganz)', 'Rotates/redirects acetabulum over femoral head'],
['Reshaping', 'Pemberton, Dega', 'Must be OPEN', 'Changes shape; reduces volume; hinges on triradiate'],
['Salvage', 'Chiari, Shelf', 'Any (even closed)', 'Does not create congruence; medialization/lateral shelf'],
]
),
P('', false),
// ─────────────────────────────────────────────────────────
pageBreak(),
H1('12. MCQ BANK — 10 QUESTIONS'),
H3('(Mixed DNB/MS Final + Fellowship Level)'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q1. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('In a 2-week-old female infant, Ortolani test is positive in the left hip. Which single most important risk factor was present in this child?'),
bullet('A. Congenital muscular torticollis'),
bullet('B. Oligohydramnios'),
bullet('C. Breech presentation in late trimester'),
bullet('D. Metatarsus adductus'),
highlight('Answer: C. Breech presentation is the single most important risk factor for DDH. The combination of female sex + breech gives a 2.8% incidence. (Mnemonic: FFOBB — Breech is #1 mechanical factor)', 'E8F5E9'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q2. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('A 3-month-old girl has limited left hip abduction. Ultrasound shows α angle of 46° and β angle of 72°. What is the Graf type?'),
bullet('A. Type IIa'),
bullet('B. Type IIc'),
bullet('C. Type D'),
bullet('D. Type III'),
highlight('Answer: B. Type IIc. α angle 43–49° with β angle <77° = Type IIc. If β were >77°, it would be Type D (decentering). Both need Pavlik harness.', 'E8F4FD'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q3. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('A Pavlik harness is applied to a 5-week-old with dislocated left hip (Ortolani positive). After 4 weeks, repeat ultrasound shows the hip remains dislocated. What is the next most appropriate step?'),
bullet('A. Continue Pavlik harness for another 4 weeks'),
bullet('B. Increase the abduction angle in the harness'),
bullet('C. STOP harness; plan closed reduction under GA'),
bullet('D. Apply rigid abduction brace'),
highlight('Answer: C. "Pavlik Disease" — if reduction not achieved in 3 weeks, harness should be discontinued. Continued attempts erode the posterior acetabular wall, making subsequent closed reduction more difficult. Next step: closed reduction under GA with arthrogram.', 'FFE0E0'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q4. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('During open reduction of DDH via an anterior approach, the surgeon finds the femoral head cannot reach the acetabulum despite releasing the contracted inferomedial capsule. The most likely remaining obstacle is:'),
bullet('A. Hypertrophied ligamentum teres'),
bullet('B. Iliopsoas tendon (hourglass capsular constriction)'),
bullet('C. Pulvinar'),
bullet('D. Transverse acetabular ligament'),
highlight('Answer: B. Iliopsoas tendon causes hourglass constriction of the capsule — the most important and commonly missed block. It must be divided/released to allow the femoral head to pass into the acetabulum.', 'FFF9C4'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q5. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('A 4-year-old child has persistent acetabular dysplasia (acetabular index 38°) after successful closed reduction of DDH at 8 months. The triradiate cartilage is open. What is the most appropriate pelvic osteotomy?'),
bullet('A. Ganz periacetabular osteotomy'),
bullet('B. Salter innominate osteotomy'),
bullet('C. Steel triple innominate osteotomy'),
bullet('D. Chiari pelvic osteotomy'),
highlight('Answer: B. Salter innominate osteotomy is the procedure of choice in children <5–6 years with open triradiate cartilage. Ganz PAO requires CLOSED triradiate. Steel requires closed triradiate (>8 yrs). Chiari is a salvage procedure.', 'E8F5E9'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q6. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('A 22-year-old woman presents with left hip pain. X-ray shows CE angle of 18°, AI of 28°, and no joint space narrowing. The triradiate cartilage is closed. What is the best surgical option?'),
bullet('A. Salter osteotomy'),
bullet('B. Pemberton acetabuloplasty'),
bullet('C. Ganz periacetabular osteotomy (PAO)'),
bullet('D. Chiari pelvic osteotomy'),
highlight('Answer: C. Ganz PAO is the gold standard for symptomatic acetabular dysplasia in young adults with a closed triradiate cartilage and preserved joint space. It provides best 3D correction, preserves abductors, and has excellent long-term outcomes.', 'E8F4FD'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q7. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('Avascular necrosis complicating DDH treatment is best classified by:'),
bullet('A. Ficat and Arlet classification'),
bullet('B. Kalamchi and MacEwen classification'),
bullet('C. Steinberg classification'),
bullet('D. Crowe classification'),
highlight('Answer: B. Kalamchi and MacEwen (1980) specifically classify AVN complicating DDH treatment into 4 grades based on growth plate and ossific nucleus involvement. Ficat/Steinberg are for adult AVN. Crowe classifies DDH severity in adults.', 'FFF9C4'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q8. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('A 30-year-old with Crowe Type IV DDH requires THA. Pre-operative X-ray shows the femoral head at 3 cm proximal to the true acetabulum. During THA, the surgeon plans to reconstruct at the true acetabular center. The maximum safe limb lengthening to avoid nerve palsy is approximately:'),
bullet('A. 2 cm'),
bullet('B. 4 cm'),
bullet('C. 6 cm'),
bullet('D. 8 cm'),
highlight('Answer: B. The safe limit for acute limb lengthening in DDH THA is approximately 4 cm. Beyond this, sciatic nerve palsy risk increases significantly. Femoral shortening osteotomy is performed if >4 cm lengthening is needed.', 'FFE0E0'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q9. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('On arthrogram during closed reduction of DDH, a "thorn sign" is noted at the superior aspect of the acetabulum. This indicates:'),
bullet('A. Inverted labrum blocking reduction — open reduction needed'),
bullet('B. Pulvinar in the acetabulum'),
bullet('C. Normal labral position — reduction is adequate'),
bullet('D. Torn transverse acetabular ligament'),
highlight('Answer: C. The "thorn sign" on arthrogram represents the NORMAL position of the labrum (acetabular limbus) pointing upward from the acetabular roof — this confirms adequate reduction. An absent or reversed thorn = inverted labrum = inadequate reduction.', 'E8F5E9'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q10. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('The Ramsey Safe Zone in DDH treatment refers to:'),
bullet('A. The range of hip abduction beyond which AVN risk is zero'),
bullet('B. The arc between maximum abduction before AVN and maximum adduction before redislocation'),
bullet('C. The range of hip flexion safe for Pavlik harness use'),
bullet('D. The acetabular sector angle within which reduction is stable'),
highlight('Answer: B. The Ramsey Safe Zone is the arc between: (1) maximum adduction at which dislocation occurs, and (2) maximum abduction at which AVN risk begins (due to excessive tension on the posterosuperior retinacular vessels from the MFCA). A safe zone of <20–40° is considered narrow and warrants adductor tenotomy.', 'E8F4FD'),
P('', false),
// ─────────────────────────────────────────────────────────
divider(),
new Paragraph({
children: [new TextRun({ text: 'END OF DDH NOTES | Prepared July 2026 | Sources: Campbell\'s 15e, Miller\'s 9e, Bailey & Love 28e, Grainger Radiology, PubMed 2023–2026', color: '7F7F7F', size: 18 })],
alignment: AlignmentType.CENTER,
spacing: { before: 200 }
}),
]
}]
});
Packer.toBuffer(doc).then(buffer => {
fs.writeFileSync('/home/daytona/workspace/ddh-notes/DDH_Ortho_PG_Notes.docx', buffer);
console.log('DOCX created successfully');
});
cd /home/daytona/workspace/ddh-notes && node create_ddh_notes.js 2>&1
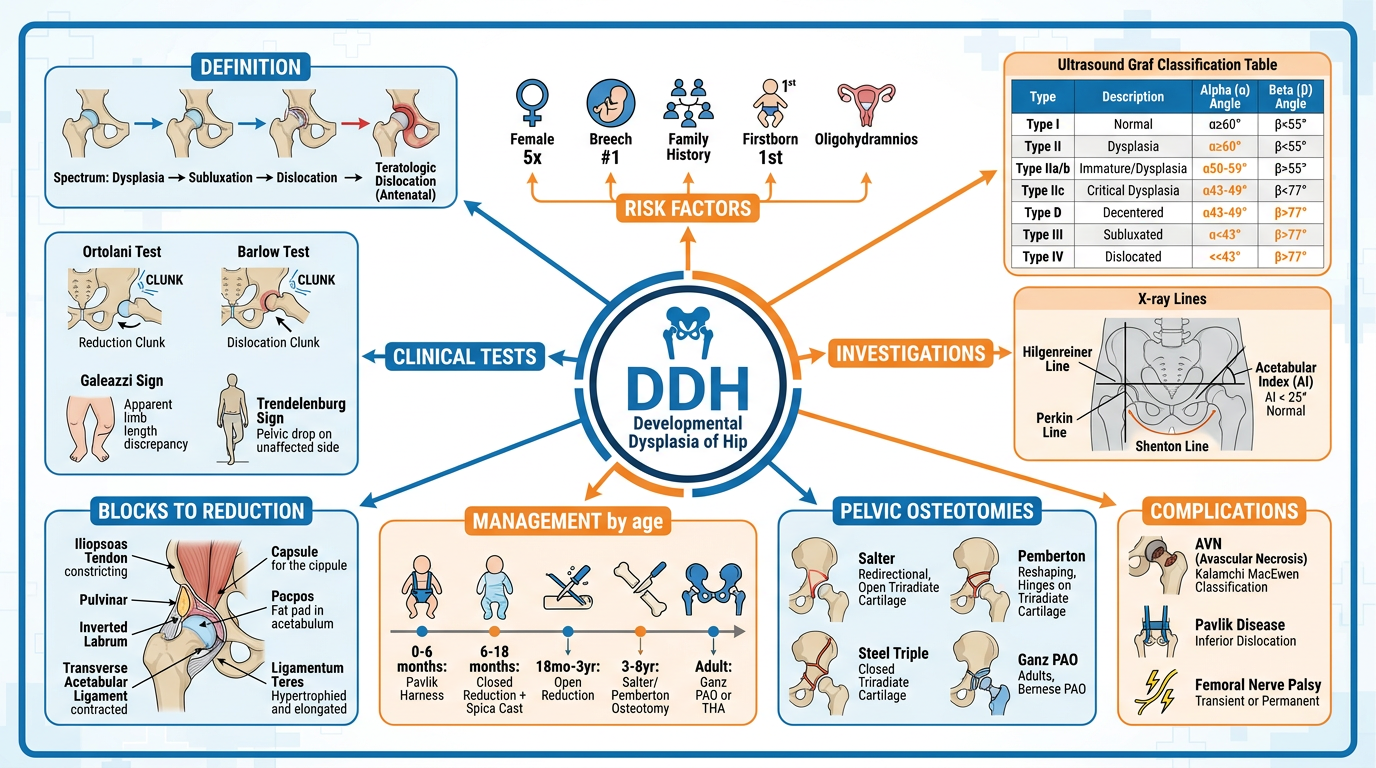
A comprehensive medical visual mind map poster for Developmental Dysplasia of Hip (DDH) for orthopaedic postgraduate exam revision. Central node: "DDH" with branches radiating outward. Include: 1) DEFINITION branch: spectrum from dysplasia to teratologic dislocation. 2) RISK FACTORS branch: Female 5x, Breech #1, Family history, Firstborn, Oligohydramnios. 3) CLINICAL TESTS branch: Ortolani test (reduction clunk), Barlow test (dislocation clunk), Galeazzi sign, Trendelenburg sign. 4) INVESTIGATIONS branch: Ultrasound Graf classification table (Type I normal α≥60°, Type IIa/b α50-59°, Type IIc α43-49° β less than 77°, Type D α43-49° β greater than 77°, Type III and IV α less than 43°), X-ray lines (Hilgenreiner, Perkin, Shenton, Acetabular index less than 25 degrees normal). 5) BLOCKS TO REDUCTION branch showing Iliopsoas tendon, Pulvinar, Inverted labrum, Transverse acetabular ligament, Ligamentum teres. 6) MANAGEMENT by age branch: 0-6 months Pavlik harness, 6-18 months Closed reduction + spica, 18mo-3yr Open reduction, 3-8yr Salter/Pemberton osteotomy, adult Ganz PAO or THA. 7) PELVIC OSTEOTOMIES: Salter (redirectional, open triradiate), Pemberton (reshaping, hinges on triradiate), Steel triple (closed triradiate), Ganz PAO (adults). 8) COMPLICATIONS: AVN (Kalamchi MacEwen classification), Pavlik disease, Femoral nerve palsy. Color-coded sections with anatomical hip diagrams, arrows, important angles highlighted. Clean professional medical infographic style with white background, blue and orange color scheme.
ls -lh /home/daytona/workspace/ddh-notes/ && python /home/daytona/skills/docx/sc…
python3 -c "import zipfile; z = zipfile.ZipFile('/home/daytona/workspace/ddh-not…
DEVELOPMENTAL DYSPLASIA OF THE HIP (DDH)
Complete PG Orthopaedics Notes | DNB / MS Final + Fellowship Level
📥 Downloads
DDH Ortho PG Notes
Word Document · DOCX
🗺️ Visual Mind Map Poster
1. DEFINITION & SPECTRUM
| Spectrum | Description |
|---|---|
| Dysplasia | Shallow acetabulum only; femoral head in joint |
| Subluxation | Partial loss of contact between femoral head and acetabulum |
| Dislocation | Complete loss of contact |
| Teratologic | Dislocated IN UTERO; irreducible; associated with arthrogryposis, Larsen syndrome |
| Late dysplasia | Adolescent/adult presentation |
Key: In a newborn, the femoral head CAN be reduced (Ortolani positive). In older children, it CANNOT be reduced (Ortolani negative - fixed dislocation).
2. EPIDEMIOLOGY
| Parameter | Value |
|---|---|
| Incidence (clinical exam) | 1–3 per 1,000 live births |
| Incidence (ultrasound) | Up to 25 per 1,000 |
| True DDH on repeat US | ~5 per 1,000 |
| Female : Male | 5 : 1 |
| Left : Right : Bilateral | 67% : 20% : 13% |
| Female + Breech | 2.8% |
| Family history | ~10% risk (if parent + sibling: ~36%) |
Risk Factors - Mnemonic "FFOBB"
- F - Female sex
- F - Family history
- O - Oligohydramnios
- B - Breech presentation (most important mechanical factor)
- B - Born first (reduced intrauterine space)
Also associated with: Congenital muscular torticollis (8% co-occurrence), Metatarsus adductus (10%). NO association with clubfoot.
3. PATHOANATOMY
Blocks to Reduction - Mnemonic "I PITCH"
| Block | Description |
|---|---|
| I - Iliopsoas tendon | Creates hourglass constriction of capsule - most important |
| P - Pulvinar | Fibrofatty tissue filling the acetabulum |
| I - Inverted labrum | Limbus inverted into acetabulum blocking reduction |
| T - Transverse acetabular ligament | Narrows acetabular opening inferiorly |
| C - Capsule (hourglass) | Contracted inferomedial capsule |
| H - Hypertrophied ligamentum teres | Takes up space in acetabulum |
4. CLINICAL FEATURES BY AGE
Neonatal (0–3 months)
| Test | Mechanism | Detects | Positive Sign |
|---|---|---|---|
| Ortolani | Abduct + lift greater trochanter anteriorly | Reduction of dislocated hip | Palpable CLUNK (not click) of reduction |
| Barlow | Adduct + posterior pressure on femoral head | Dislocation of unstable hip | Palpable CLUNK of dislocation |
| Galeazzi | Flex both hips + knees, compare knee heights | Foreshortened femur | Unequal knee heights (affected side lower) |
| Restricted abduction | Compare both sides | Adductor contracture | <45° or asymmetric |
Memory: Ortolani = "Out to In" (reduction). Barlow = "In to Out" (dislocation). Both go NEGATIVE as hip stiffens.
3–18 Months
- Limited hip abduction - most reliable sign
- Ortolani/Barlow become negative (stiffness)
- Galeazzi positive
- Asymmetric skin folds (less reliable)
Walking Age (>18 months)
- Trendelenburg gait (abductor weakness)
- Hyperlordosis + pelvic obliquity
- Bilateral DDH: Waddling gait
- Telescoping (proximal femur moveable in/out of pseudoacetabulum)
5. INVESTIGATIONS
A. Ultrasound - GOLD STANDARD (<4-6 months)
- α (alpha) angle = bony coverage of femoral head (key angle)
- β (beta) angle = cartilaginous coverage
| Graf Type | Alpha (α) | Beta (β) | Description | Treatment |
|---|---|---|---|---|
| Ia | ≥ 60° | < 55° | Normal, sharp bony rim | None |
| Ib | ≥ 60° | > 55° | Normal, blunt bony rim | None |
| IIa | 50–59° | < 77° | Immature <3 months (physiological) | Observe; Pavlik if persists |
| IIb | 50–59° | < 77° | Immature >3 months (pathological) | Pavlik harness |
| IIc | 43–49° | < 77° | Deficient bony roof; still centered | Pavlik harness |
| Type D | 43–49° | > 77° | Decentering; labrum displaced | Pavlik harness |
| Type III | < 43° | > 77° | Subluxated; labrum pressed up | Pavlik / Closed reduction |
| Type IV | < 43° | Unmeasurable | Dislocated; labrum inverted down | Closed/Open reduction |
Key rule: α angle determines the type. β angle only used to differentiate Ia/Ib AND IIc/D.
B. Plain Radiography (>4-6 months when ossific nucleus appears)
| Line/Index | Description | Normal |
|---|---|---|
| Hilgenreiner line (H-line) | Horizontal through both triradiate cartilages | Reference |
| Perkin line (P-line) | Vertical through lateral acetabular edge | Reference |
| Acetabular Index (AI) | Angle between H-line and acetabular roof | < 25° |
| Shenton's line | Continuous arc (femoral neck - obturator foramen) | Should be smooth |
| Von Rosen view | X-ray in 45° abduction + internal rotation | Femoral line passes through acetabulum |
| CE angle (Wiberg) | Lateral coverage of femoral head | > 25° (adult) |
In DDH: Ossific nucleus in OUTER-LOWER quadrant (lateral to Perkin, below Hilgenreiner). Shenton's line broken. Increased AI.
C. Arthrography (Intraoperative)
- Thorn sign = Normal labrum pointing up = adequate reduction ✓
- Absent/reversed thorn = Inverted labrum = inadequate reduction ✗
6. MANAGEMENT - AGE-BASED ALGORITHM
0–6 months ──→ Pavlik Harness (confirm with US)
│
├─ Success → Continue 6-8 weeks part time
└─ Fail at 3 weeks → STOP (risk Pavlik disease)
└──→ Closed Reduction + Spica
6–18 months ──→ Closed Reduction + Hip Spica (GA + arthrogram)
└─ Fail → Open Reduction (anterior approach)
18 months–3 yrs ──→ Open Reduction + Femoral Shortening
± Pelvic Osteotomy
3–8 years ──→ Open Reduction + Salter/Pemberton + DVRO
>8 years ──→ Triple osteotomy (Steel) or Ganz PAO
Salvage: Chiari / Shelf if non-congruent
Adult ──→ Ganz PAO (if cartilage intact) | THA (when OA)
A. Pavlik Harness (Detailed)
- Maintains hip at ~100° flexion + mild abduction ("human position" = Salter position)
- Worn 23 hours/day for at least 6 weeks after reduction
- Must keep hip within Ramsey Safe Zone (between redislocation and AVN zone)
- Confirm reduction with ultrasound after placement
- Age >7 weeks at start
- Bilateral dislocation
- Absence of Ortolani sign
B. Pelvic Osteotomies
| Procedure | Type | Triradiate Cartilage | Age | Key Feature |
|---|---|---|---|---|
| Salter | Redirectional | Must be OPEN | <5–6 years | Rotates acetabulum anterolaterally; iliac crest graft; may lengthen 1 cm |
| Pemberton | Reshaping (volume-reducing) | Must be OPEN | <8 years | Hinges on triradiate; reduces acetabular volume |
| Dega | Reshaping | Must be OPEN | Any (esp. paralytic) | Posterior coverage; favored in neuromuscular DDH |
| Steel Triple | Redirectional (3 cuts) | Must be CLOSED | >8 years | Ischium + pubis + ilium cuts |
| Tönnis Triple | Redirectional | Must be CLOSED | Adolescent | Close to acetabulum; more correction |
| Ganz PAO | Periacetabular redirectional | Must be CLOSED | Adults | Best 3D correction; preserves abductors; single incision; allows capsulotomy |
| Chiari | Salvage - medialization | Any | Any age (non-congruent) | Medialization only; NOT reconstructive |
| Shelf | Salvage - lateral bone graft | Any | Any age (non-congruent) | Extra-articular lateral coverage |
C. Open Reduction - Approach Choice
| Approach | Age | Advantages | Disadvantages |
|---|---|---|---|
| Medial (Ludloff) | <12 months | Less blood loss; directly addresses blocks | No capsulorrhaphy; higher AVN risk; no access for pelvic osteotomy |
| Anterior (Smith-Peterson) | >12 months (preferred) | Capsulorrhaphy possible; access for pelvic osteotomy; lower AVN | More dissection |
7. COMPLICATIONS
| Complication | Key Points |
|---|---|
| AVN (Osteonecrosis) - most feared | Kalamchi & MacEwen Grade I–IV; MFCA posterosuperior retinacular branch at risk; avoid excessive abduction |
| Pavlik Disease | Erosion of posterior acetabular wall; prevent by stopping harness at 3 weeks if no reduction |
| Residual Dysplasia | Monitor AI; pelvic osteotomy if AI >25° at age 2 |
| Redislocation | Inadequate soft tissue release or capsulorrhaphy |
| Femoral nerve palsy | Excessive flexion in Pavlik (>120°); usually transient |
| Premature OA | Long-term consequence of untreated/inadequately treated DDH |
Kalamchi & MacEwen AVN Classification:
| Grade | Feature | Prognosis |
|---|---|---|
| I | Temporary growth irregularity of ossific nucleus only | Good |
| II | Premature closure of LATERAL physis | Progressive valgus |
| III | Premature closure of CENTRAL physis | Progressive valgus |
| IV | Total ischemic necrosis of entire femoral head | Poor - global collapse |
8. ADULT DDH - Crowe Classification
| Class | Subluxation | Description |
|---|---|---|
| I | <50% head diameter | Mild; dysplastic only |
| II | 50–75% head diameter | Moderate subluxation |
| III | 75–100% head diameter | Significant subluxation |
| IV | >100% head diameter | Complete dislocation |
9. RECENT EVIDENCE (2023–2026)
| PMID | Study | Key Finding |
|---|---|---|
| 39853978 | Tirta et al., JAMA Netw Open 2025 | Strongest pre-3-month risk factors: breech > female > family history |
| 38053132 | Huang et al., BMC 2023 | Swaddling with hips in extension significantly increases DDH incidence |
| 37879719 | Tao et al., BMJ Paediatrics 2023 | True prevalence ~3.5/1000 by clinical exam |
| 37688602 | Shahbazi et al., Int Orthop 2023 | THA dislocation risk in DDH: Crowe IV, small acetabular component, no dual-mobility cup |
| 39354451 | Jacobsen et al., BMC 2024 | GDF5, TGFB1, CX3CR1 genes implicated in DDH |
10. CLASSIC LANDMARK ARTICLES
| Author / Year | Contribution |
|---|---|
| Ortolani (1937) | Described reduction "clunk" sign - basis of neonatal screening |
| Barlow (1962) | Provocative dislocation test - British screening basis |
| Pavlik (1950/1989) | Functional harness treatment for CDH |
| Salter (1961) | Innominate osteotomy - landmark redirectional pelvic osteotomy |
| Pemberton (1965) | Pericapsular acetabuloplasty hinged on triradiate cartilage |
| Wiberg (1939) | CE angle for measuring lateral acetabular coverage |
| Graf (1980s) | Ultrasound classification with α and β angles |
| Thomas, Wedge & Salter (2007) | 45-year follow-up of open reduction + innominate osteotomy - excellent long-term outcomes |
| Kalamchi & MacEwen (1980) | Classification of AVN complicating DDH treatment |
| Crowe et al. | Crowe classification for adult DDH/THA planning |
11. 10 MCQs - Mixed DNB/MS + Fellowship Level
- A. Congenital muscular torticollis
- B. Oligohydramnios
- C. Breech presentation in late trimester ✓
- D. Metatarsus adductus
Answer: C. Breech is the most important mechanical risk factor. Female + breech gives 2.8% incidence.
- A. Type IIa
- B. Type IIc ✓
- C. Type D
- D. Type III
Answer: B. α = 43–49° + β <77° = Type IIc. If β >77° it would be Type D. Both need Pavlik harness.
- A. Continue Pavlik for another 4 weeks
- B. Increase abduction angle in harness
- C. STOP harness; plan closed reduction under GA ✓
- D. Apply rigid abduction brace
Answer: C. "Pavlik Disease" - if reduction not achieved in 3 weeks, stop harness immediately. Continuing erodes the posterior acetabular wall. Next: closed reduction under GA with arthrogram.
- A. Hypertrophied ligamentum teres
- B. Iliopsoas tendon (hourglass capsule) ✓
- C. Pulvinar
- D. Transverse acetabular ligament
Answer: B. Iliopsoas tendon causes hourglass constriction - the most important block. Division is mandatory.
- A. Ganz PAO
- B. Salter innominate osteotomy ✓
- C. Steel triple innominate
- D. Chiari
Answer: B. Salter is for <5-6 years with open triradiate. Ganz PAO requires CLOSED triradiate. Steel requires closed triradiate (>8 years). Chiari is salvage only.
- A. Salter osteotomy
- B. Pemberton acetabuloplasty
- C. Ganz periacetabular osteotomy (PAO) ✓
- D. Chiari osteotomy
Answer: C. Ganz PAO is the gold standard for symptomatic dysplasia in young adults with closed triradiate and preserved joint space.
- A. Ficat and Arlet
- B. Kalamchi and MacEwen ✓
- C. Steinberg
- D. Crowe
Answer: B. Kalamchi & MacEwen (1980) specifically classify AVN in DDH treatment. Ficat/Steinberg are for adult AVN; Crowe classifies DDH severity in adults.
- A. 2 cm
- B. 4 cm ✓
- C. 6 cm
- D. 8 cm
Answer: B. Safe limit is ~4 cm. Beyond this, sciatic nerve palsy risk increases sharply. Femoral shortening osteotomy is performed if >4 cm lengthening is needed.
- A. Inverted labrum - open reduction needed
- B. Pulvinar in acetabulum
- C. Normal labral position - reduction is adequate ✓
- D. Torn transverse acetabular ligament
Answer: C. Thorn sign = normal labrum pointing superiorly from the acetabular roof = adequate concentric reduction confirmed.
- A. Abduction range beyond which AVN risk is zero
- B. The arc between maximum adduction before dislocation and maximum abduction before AVN ✓
- C. Safe range of hip flexion in Pavlik harness
- D. Sector angle within which reduction is stable
Answer: B. Ramsey Safe Zone = between (1) max adduction at which dislocation occurs AND (2) max abduction at which AVN begins (from MFCA compression). Safe zone <20-40° = narrow; consider adductor tenotomy before casting.
Key Mnemonics Summary
| Mnemonic | Stands For |
|---|---|
| FFOBB | Risk factors: Female, Family history, Oligohydramnios, Breech, Born first |
| I PITCH | Blocks to reduction: Iliopsoas, Pulvinar, Inverted labrum, Transverse acetabular lig, Capsule, Hypertrophied ligamentum teres |
| "Out to In" | Ortolani = reduces the hip |
| "In to Out" | Barlow = dislocates the hip |
| "3 weeks, STOP" | Pavlik disease prevention rule |
- Campbell's Operative Orthopaedics 15th Ed 2026, Ch. 32
- Miller's Review of Orthopaedics 9th Ed, Ch. 3
- Bailey & Love's Short Practice of Surgery 28th Ed, Ch. 5
- Grainger & Allison's Diagnostic Radiology, Ch. 73
- PubMed meta-analyses 2023–2026 (PMIDs: 39853978, 38053132, 37879719, 37688602, 39354451)
ctev
"clubfoot"[MeSH Terms] AND "Ponseti"
CTEV clubfoot Ponseti method Dimeglio classification Pirani score classic articles landmark 2024
"talipes equinovarus"[MeSH Terms] AND "treatment outcome"[MeSH Terms]
Pirani score CTEV 6 signs hindfoot midfoot scoring system Dimeglio 4 grades table
~/ddh-notes/create_ctev_notes.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
HeadingLevel, AlignmentType, BorderStyle, WidthType, ShadingType,
VerticalAlign, PageBreak, UnderlineType
} = require('docx');
const fs = require('fs');
const H1 = (text) => new Paragraph({ text, heading: HeadingLevel.HEADING_1, spacing: { before: 360, after: 120 } });
const H2 = (text) => new Paragraph({ text, heading: HeadingLevel.HEADING_2, spacing: { before: 240, after: 80 } });
const H3 = (text) => new Paragraph({ text, heading: HeadingLevel.HEADING_3, spacing: { before: 180, after: 60 } });
const P = (text, bold=false, color=undefined) => new Paragraph({ children: [new TextRun({ text, bold, color })], spacing: { before: 60, after: 60 } });
const bullet = (text, bold=false, level=0) => new Paragraph({ children: [new TextRun({ text, bold })], bullet: { level }, spacing: { before: 40, after: 40 } });
const divider = () => new Paragraph({ children: [new TextRun({ text: '─'.repeat(80), color: '999999' })], spacing: { before: 120, after: 120 } });
const pageBreak = () => new Paragraph({ children: [new PageBreak()] });
const highlight = (text, color='FFD700') => new Paragraph({ children: [new TextRun({ text, bold: true })], shading: { type: ShadingType.CLEAR, fill: color }, spacing: { before: 80, after: 80 }, indent: { left: 200 } });
function makeTable(headers, rows, headerColor = '1F4E79') {
const headerRow = new TableRow({
children: headers.map(h => new TableCell({
children: [new Paragraph({ children: [new TextRun({ text: h, bold: true, color: 'FFFFFF' })], alignment: AlignmentType.CENTER })],
shading: { type: ShadingType.CLEAR, fill: headerColor }, verticalAlign: VerticalAlign.CENTER
}))
});
const dataRows = rows.map(row => new TableRow({
children: row.map((cell, i) => new TableCell({
children: [new Paragraph({ children: [new TextRun({ text: String(cell) })], alignment: AlignmentType.CENTER })],
shading: { type: ShadingType.CLEAR, fill: i === 0 ? 'D6E4F0' : 'FFFFFF' }
}))
}));
return new Table({ rows: [headerRow, ...dataRows], width: { size: 100, type: WidthType.PERCENTAGE } });
}
const doc = new Document({
title: 'CTEV - Congenital Talipes Equinovarus - Comprehensive Notes',
sections: [{
children: [
// TITLE
new Paragraph({ children: [new TextRun({ text: 'CONGENITAL TALIPES EQUINOVARUS (CTEV)', bold: true, size: 48, color: '1F4E79' })], alignment: AlignmentType.CENTER, spacing: { before: 400, after: 200 } }),
new Paragraph({ children: [new TextRun({ text: 'Clubfoot | Comprehensive PG Orthopaedics Study Notes | DNB / MS / Fellowship Level', color: '7F7F7F', size: 24 })], alignment: AlignmentType.CENTER, spacing: { after: 100 } }),
new Paragraph({ children: [new TextRun({ text: "Sources: Campbell's 15e 2026 | Miller's Review 9e | Bailey & Love 28e | PubMed 2023–2026", color: '7F7F7F', size: 20 })], alignment: AlignmentType.CENTER, spacing: { after: 400 } }),
divider(),
// ─── 1. DEFINITION
H1('1. DEFINITION'),
P('Congenital Talipes Equinovarus (CTEV) is a three-dimensional complex foot deformity present at birth, characterized by four components remembered by the mnemonic CAVE.'),
P('', false),
makeTable(
['Component', 'Deformity', 'Key Structure Involved'],
[
['C — Cavus', 'Elevated longitudinal arch; pronation of forefoot relative to hindfoot', 'Plantar fascia, intrinsic muscles'],
['A — Adductus', 'Forefoot adduction at midtarsal joint; medial deviation', 'Talonavicular joint subluxation'],
['V — Varus', 'Hindfoot varus; calcaneum inverted', 'Subtalar joint, calcaneofibular ligament'],
['E — Equinus', 'Plantarflexion of hindfoot; cannot dorsiflex', 'Tendo-Achilles shortening, posterior capsule'],
]
),
P('', false),
highlight('MNEMONIC — CAVE: Cavus → Adductus → Varus → Equinus. This is ALSO the ORDER of Ponseti correction (correct in reverse: C first, then A, V, then E last).', 'E8F5E9'),
P('', false),
H3('CAVE vs. ORDER OF CORRECTION:'),
bullet('Deformity: C-A-V-E (Cavus, Adductus, Varus, Equinus)'),
bullet('Ponseti correction sequence: C → A+V simultaneously → E (after tenotomy)'),
bullet('KEY: Equinus corrected LAST (by percutaneous Achilles tenotomy in 90% of cases)'),
// ─── 2. EPIDEMIOLOGY
pageBreak(),
H1('2. EPIDEMIOLOGY'),
makeTable(
['Parameter', 'Value'],
[
['Incidence', '1–6 per 1,000 live births (varies ethnically)'],
['Sex ratio', 'Boys : Girls = 2 : 1 (Boys TWICE as common)'],
['Bilateral', '50% of cases'],
['Unilateral', '50%; right and left equally affected'],
['Family history', 'Multifactorial; first-degree relative increases risk 10–30x'],
['Associated with spina bifida', 'Neuromuscular CTEV — harder to treat'],
]
),
P('', false),
H3('Types of CTEV:'),
makeTable(
['Type', 'Characteristics', 'Treatment Response'],
[
['Postural (positional)', 'Flexible; corrects with passive dorsiflexion; normal heel; NOT TRUE CTEV', 'Physiotherapy stretches; normal by 3 months'],
['Idiopathic (structural)', 'Fixed; tight heel cord; "empty heel"; deep medial + posterior creases; MOST COMMON', 'Ponseti method — 95% success'],
['Neuromuscular', 'Associated with spina bifida, arthrogryposis, CP; more rigid', 'Ponseti possible but higher relapse; surgery often needed'],
['Syndromic/Teratologic', 'Associated with trisomy 18, diastrophic dwarfism, amniotic band syndrome', 'Often surgical; poor prognosis'],
]
),
P('', false),
// ─── 3. ETIOLOGY & PATHOLOGY
H1('3. ETIOLOGY & PATHOLOGY'),
H2('A. Etiology'),
bullet('Majority: IDIOPATHIC — multifactorial genetic basis'),
bullet('Genetic: PITX1-TBX4 transcriptional pathway implicated (Miller\'s)'),
bullet('Associated syndromes: Arthrogryposis (most common neuromuscular cause), Myelomeningocele, Larsen syndrome, Diastrophic dysplasia, Trisomy 18, Amniotic band syndrome, Streeter dysplasia, Prune-belly syndrome, Tibial hemimelia'),
bullet('Environmental: Intrauterine compression, oligohydramnios, first pregnancy'),
P('', false),
H2('B. Pathology — Structural Changes'),
bullet('PRIMARY BONY CHANGE: Talar neck deformity — medial and plantar deviation of talar neck'),
bullet('Navicular displaced medially on talar head (talonavicular subluxation)'),
bullet('Calcaneus: Medially rotated, inverted under talus; "parallelism" of talus and calcaneus on X-ray'),
bullet('Soft tissue: Shortened Achilles tendon, tibialis posterior, FHL, FDL, plantar fascia, posterior capsule, calcaneofibular ligament'),
bullet('Muscles: Gastrocsoleus and tibialis posterior smaller than normal; increased connective tissue; reduced myofibrils'),
bullet('Vascular: Anterior tibial artery may be absent or diminutive; dorsalis pedis may be diminished'),
P('', false),
highlight('KEY: The talus is the KEY BONE in CTEV. The talar neck is deviated medially and plantarward. ALL correction maneuvers use the head of the talus as a FULCRUM.', 'FFE0E0'),
// ─── 4. CLINICAL FEATURES
pageBreak(),
H1('4. CLINICAL FEATURES'),
H2('A. Inspection'),
bullet('Foot in equinus, varus, adduction and cavus position'),
bullet('"Empty heel" — calcaneus pulled up; heel appears empty on palpation'),
bullet('Deep medial crease (at talonavicular joint level)'),
bullet('Deep posterior crease (at ankle level — indicates equinus)'),
bullet('Single posterior crease = equinus; medial crease = varus/adductus'),
bullet('Small calf and foot (tibial shortening may develop with growth)'),
bullet('Skin creases on dorsum of foot (from chronic dorsiflexion attempt)'),
P('', false),
H2('B. Distinguishing Postural vs. Structural CTEV'),
makeTable(
['Feature', 'Postural Clubfoot', 'Structural CTEV'],
[
['Passively correctable', 'YES — foot reaches neutral or beyond', 'NO — fixed deformity'],
['Heel', 'Normal heel pad present', '"Empty heel" — calcaneus pulled up'],
['Creases', 'Absent or mild', 'Deep medial + posterior creases'],
['Treatment', 'Stretching only', 'Ponseti casting required'],
['Resolution', 'Normal by 3 months', 'Requires treatment'],
]
),
P('', false),
H2('C. Associated Features'),
bullet('Small calf and short foot (ipsilateral)'),
bullet('Tibial internal torsion (often accompanies clubfoot)'),
bullet('Check for: Neural tube defect (sacral dimple, hairy patch), hip instability (DDH co-occurrence), limb abnormalities'),
// ─── 5. CLASSIFICATION
pageBreak(),
H1('5. CLASSIFICATION / SCORING SYSTEMS'),
H2('A. Pirani Scoring System (MOST COMMONLY USED)'),
P('Assesses 6 clinical signs in the position of MAXIMAL PASSIVE CORRECTION. Each sign scored 0 (none), 0.5 (moderate), or 1 (severe). Total = 0–6.'),
P('', false),
makeTable(
['Zone', 'Sign', 'Score 0', 'Score 0.5', 'Score 1'],
[
['MIDFOOT (3 signs)', 'Curvature of lateral border', 'Straight/mildly curved', 'Curved', 'Severely curved (bean-shaped)'],
['MIDFOOT', 'Lateral head of talus palpable', 'Not palpable', 'Partially covered', 'Fully exposed/prominent'],
['MIDFOOT', 'Medial crease', 'Absent', 'Single shallow crease', 'Deep crease altering arch contour'],
['HINDFOOT (3 signs)', 'Posterior crease', 'Multiple fine creases', 'One or two deep creases', 'Deep crease changing foot contour'],
['HINDFOOT', 'Empty heel', 'Heel pad full', 'Partially empty', 'Completely empty'],
['HINDFOOT', 'Rigid equinus', 'Dorsiflexion >0°', 'Dorsiflexion 0° to –15°', 'Rigid equinus <–15°'],
]
),
P('', false),
highlight('Pirani Score Interpretation: 0–1 = mild; 1–3 = moderate; 4–6 = severe. Score >3.5 = Achilles tenotomy very likely needed. Score at bracing predictive of relapse risk.', 'E8F4FD'),
P('', false),
H2('B. Dimeglio Classification System (20-point scale)'),
P('Assesses 4 positional parameters (each 0–4 based on reducibility = 16 points) + 4 pejorative signs (1 point each = 4 points). Total = 0–20.'),
makeTable(
['Dimeglio Grade', 'Score', 'Description', '% of Cases'],
[
['Grade I — Benign/Soft', '≤ 5', 'Soft, easily correctable; postural', '20%'],
['Grade II — Moderate', '6–10', 'Partially reducible; standard idiopathic', '33%'],
['Grade III — Severe', '11–15', 'Stiff, resistant; partially reducible', '35%'],
['Grade IV — Very Severe', '16–20', 'Rigid, irreducible; teratologic', '12%'],
]
),
P('', false),
H3('4 Positional Parameters (each 0–4 based on degrees of reducibility):'),
bullet('1. Equinus (sagittal plane)'),
bullet('2. Hindfoot varus (frontal plane)'),
bullet('3. Derotation of calcaneo-forefoot block (horizontal plane)'),
bullet('4. Forefoot adduction (horizontal plane)'),
H3('4 Pejorative signs (1 point each):'),
bullet('Deep posterior crease'),
bullet('Deep medial crease'),
bullet('Cavus'),
bullet('Muscle abnormalities (poor calf)'),
P('', false),
highlight('REMEMBER: Pirani = 6-point (simpler, more widely used). Dimeglio = 20-point (more detailed, more work). Both assess severity and predict treatment response.', 'FFF9C4'),
// ─── 6. INVESTIGATIONS
pageBreak(),
H1('6. INVESTIGATIONS'),
H2('A. Clinical Diagnosis — No X-rays Needed in Neonates'),
bullet('Diagnosis is CLINICAL in infants'),
bullet('Minimal ossification in neonatal foot — X-rays unreliable initially'),
P('', false),
H2('B. Prenatal Ultrasound'),
bullet('Detectable on antenatal US from ~16–20 weeks gestation'),
bullet('Sensitivity higher for bilateral cases'),
bullet('Important for counseling; associated syndromes must be ruled out'),
P('', false),
H2('C. Plain X-rays (when used)'),
P('Used in older children, after ossification, and for operative planning.'),
makeTable(
['X-ray View', 'Measurement', 'Normal', 'CTEV Finding'],
[
['AP view', 'Talocalcaneal (Kite) angle', '20–40°', '< 20° (parallel; may be 0–5°)'],
['AP view', 'Talo-1st MT angle', '0–20° (positive)', 'NEGATIVE (medial deviation)'],
['Lateral (Turco) dorsiflexion view', 'Talocalcaneal angle', '35–50°', '< 35° (parallel)'],
['Lateral view', 'Talo-calcaneal parallelism', 'Divergent bones', '"Parallelism" = both parallel'],
['Lateral view', 'Calcaneal pitch', 'Normal height', 'Decreased (equinus)'],
]
),
P('', false),
highlight('KEY X-RAY FINDING: "Parallelism" of talus and calcaneus on BOTH AP and lateral views. Talocalcaneal angle (Kite angle) < 20° on AP = diagnostic. (Normal: 20–40°)', 'E8F4FD'),
P('', false),
H2('D. MRI'),
bullet('Not routine; used for operative planning in resistant/recurrent cases'),
bullet('Shows talar neck deformity, cartilaginous anatomy, soft tissue contracts'),
// ─── 7. TREATMENT
pageBreak(),
H1('7. TREATMENT'),
highlight('GOLDEN RULE: Treatment starts within DAYS of birth. Earlier = better outcome. Ponseti method is standard of care worldwide.', 'E8F5E9'),
P('', false),
H2('A. PONSETI METHOD — Gold Standard (95% success)'),
P('Developed by Ignacio Ponseti (University of Iowa, 1950s). Published in English 1963. Described serial manipulation + casting using the talar head as a fulcrum.'),
P('', false),
H3('PHASE 1: Serial Casting (Weeks 0–8)'),
makeTable(
['Step', 'Cast Number', 'What Is Corrected', 'Manipulation Technique'],
[
['STEP 1: Correct CAVUS first', 'Cast 1', 'Cavus — elevate first ray to pronate forefoot relative to hindfoot', 'Supinate forefoot (NOT TWIST); dorsiflex 1st ray; DO NOT abduct yet'],
['STEP 2: Correct ADDUCTUS + VARUS', 'Casts 2–4', 'Simultaneous correction of adductus and varus', 'Counter-pressure on LATERAL TALAR HEAD as fulcrum; abduct forefoot to 60–70° external rotation'],
['STEP 3: Correct EQUINUS', 'Last cast (after tenotomy)', 'Equinus — foot dorsiflexed to 10–15°', 'After percutaneous Achilles tenotomy; cast in 60–70° abduction + dorsiflexion'],
]
),
P('', false),
highlight('CRITICAL: The fulcrum of correction is the HEAD OF THE TALUS. Counter-pressure is applied over the LATERAL talar head while abducting. NEVER on the calcaneocuboid joint (causes rocker-bottom).', 'FFE0E0'),
P('', false),
H3('PHASE 2: Achilles Tenotomy'),
bullet('Required in ~90% of idiopathic clubfeet'),
bullet('Percutaneous tenotomy under local anesthesia (clinic setting)'),
bullet('Performed when residual equinus after adequate abduction correction'),
bullet('Post-tenotomy: Final cast in 70° abduction, 10–15° dorsiflexion for 3 WEEKS'),
bullet('Achilles tendon heals/regenerates in 3 weeks under cast'),
P('', false),
H3('PHASE 3: Foot Abduction Orthosis (FAO) / Denis Browne Brace'),
bullet('MOST IMPORTANT phase — non-compliance is the #1 cause of relapse'),
bullet('FAO holds feet in 60–70° external rotation bilaterally (15° on normal side if bilateral)'),
bullet('Full-time (23 hours/day) for first 3 months after correction'),
bullet('Then: Night-and-nap-time use for 3–4 YEARS total'),
bullet('Brace compliance: If worn as prescribed, relapse rate <10%. Non-compliance: relapse up to 80%'),
P('', false),
highlight('REMEMBER: Brace must be worn for a MINIMUM of 3 years (full time 3 months + night-and-nap 3 years). NON-COMPLIANCE = #1 cause of relapse. Not the surgery!', 'FFF9C4'),
P('', false),
H2('B. Number of Casts Required'),
bullet('Average: 5 casts for idiopathic clubfoot (range 4–8)'),
bullet('Higher Pirani score → more casts needed'),
bullet('Syndromic/neuromuscular → more casts, higher failure rate'),
P('', false),
H2('C. FRENCH FUNCTIONAL METHOD (Dimeglio/Bensahel)'),
bullet('Daily physiotherapy manipulation + taping by trained physiotherapist'),
bullet('More labor-intensive; used mainly in France'),
bullet('Similar outcomes to Ponseti in compliant patients'),
bullet('Not widely used outside France'),
P('', false),
// ─── 8. SURGICAL TREATMENT
pageBreak(),
H1('8. SURGICAL TREATMENT'),
H2('Indications for Surgery'),
bullet('Failed Ponseti method (only ~5% of idiopathic feet)'),
bullet('Neuromuscular/syndromic clubfoot where Ponseti fails'),
bullet('Recurrent/relapsed clubfoot (after >2 courses of casting + tibialis anterior tendon transfer fails)'),
bullet('Neglected clubfoot presenting late (>2–3 years)'),
P('', false),
H2('A. Posteromedial Release (McKay / Turco / Cincinnati)'),
P('The "comprehensive" soft tissue release for failed Ponseti, ideally performed before walking age (6–12 months).'),
makeTable(
['Incision', 'Description', 'Advantage'],
[
['Turco (medial)', 'Single medial incision', 'Good access to medial structures'],
['McKay (posteromedial)', 'Posterior + medial', 'Full posterior access'],
['Cincinnati', 'Circumferential incision (posterior + medial)', 'Best exposure; heals by secondary intention; most commonly used'],
]
),
P('', false),
H3('Structures Released:'),
bullet('Tendo-Achilles — Z-plasty lengthening'),
bullet('Tibialis posterior tendon sheath + lengthening'),
bullet('FHL, FDL lengthening'),
bullet('Posterior capsule of ankle and subtalar joints'),
bullet('Talonavicular joint capsule (medial)'),
bullet('Calcaneofibular ligament'),
bullet('Plantar fascia (if cavus component)'),
bullet('Transverse acetabular ligament (inferior to talus)'),
P('', false),
highlight('CAUTION: The POSTERIOR TIBIAL ARTERY must be protected during posteromedial release (often the dominant blood supply as dorsalis pedis may be diminished in CTEV).', 'FFE0E0'),
P('', false),
P('K-wire fixation of talonavicular joint after reduction in the correct position. Post-op: Long leg cast for 6–8 weeks.'),
P('', false),
H2('B. Tibialis Anterior Tendon Transfer (TATT)'),
bullet('Indication: Dynamic supination/recurrence in child aged 2.5–4 years (ambulatory child); after skeletal maturation of cuneiform'),
bullet('Transfer: Tibialis anterior moved from 1st cuneiform to LATERAL cuneiform (3rd cuneiform) or cuboid'),
bullet('Corrects overpull of tibialis anterior causing supination relapse'),
bullet('Often combined with re-casting before transfer'),
P('', false),
H2('C. Bony Procedures for Older Children/Neglected Cases'),
makeTable(
['Procedure', 'Age', 'Indication'],
[
['Medial opening-wedge osteotomy', '3–10 years', 'Residual adductus at medial cuneiform'],
['Lateral column shortening (Lichtblau)', '3–10 years', 'Residual forefoot adductus; cuboid decancellation'],
['Evans calcaneal osteotomy', '5+ years', 'Lateral column lengthening for residual adductus'],
['Dwyer calcaneal osteotomy', 'Older children', 'Residual hindfoot varus; lateral closing wedge osteotomy'],
['Triple arthrodesis', '>10–12 years', 'Neglected CTEV; rigid deformity; stiffens foot permanently'],
['Ilizarov/Taylor spatial frame', 'Any age', 'Complex recurrent/resistant CTEV; gradual distraction'],
]
),
P('', false),
highlight('TRIPLE ARTHRODESIS: Last resort for neglected/rigid adult CTEV. Fuses subtalar, talonavicular, calcaneocuboid joints. Contraindicated in young children (growth disturbance).', 'E8F4FD'),
P('', false),
// ─── 9. COMPLICATIONS
pageBreak(),
H1('9. COMPLICATIONS OF TREATMENT'),
makeTable(
['Complication', 'Mechanism', 'Management'],
[
['RELAPSE (most common)', 'Non-compliance with FAO brace — #1 cause. Also: inadequate initial correction, syndromic CTEV', 'Recasting; TATT if dynamic supination; revision PMR if severe'],
['Rocker-bottom deformity (iatrogenic)', 'Dorsiflexing the forefoot (midfoot) BEFORE correcting hindfoot varus → creates midfoot break', 'PREVENTION: Always correct varus before equinus. Never force equinus correction with varus uncorrected'],
['Flat-top talus (pes planus deformity)', 'Aggressive forced dorsiflexion → pressure on talar dome → flattening/avascular necrosis of talar dome', 'Prevention: Never forcefully dorsiflex; use Achilles tenotomy'],
['Overcorrection (pes valgus)', 'Excessive abduction/casting; peroneal overcorrection in PMR', 'Rare with Ponseti; requires corrective osteotomy if severe'],
['Dorsal bunion', 'Strong tibialis anterior + weak flexors after surgery; iatrogenic if peroneus longus divided', 'Capsulotomy + FHL lengthening + FHB transfer'],
['Dynamic supination', '15–20% after treatment; tibialis anterior overpull ± weak peroneus longus', 'TATT (tibialis anterior tendon transfer to lateral cuneiform)'],
['Wound dehiscence', 'Cincinnati incision; extensive soft tissue dissection', 'Secondary intention healing — usually heals well'],
['Skin necrosis', 'Poor incision placement over tight skin', 'Surgical planning with plastic surgery if needed'],
['AVN of talus', 'Vascular injury (anterior tibial artery) or excessive correction', 'Prevention; conservative if mild'],
['Leg length discrepancy', 'Small foot and calf permanent; tibial shortening over time', 'Monitor; shoe raise if significant'],
]
),
P('', false),
highlight('KEY: Rocker-bottom = Forcing dorsiflexion of FOREFOOT (midfoot break) before correcting hindfoot. This is the CLASSIC iatrogenic complication of incorrect casting technique.', 'FFE0E0'),
// ─── 10. RECURRENCE / RELAPSE
pageBreak(),
H1('10. RELAPSE MANAGEMENT'),
H2('Definition of Relapse:'),
bullet('Re-emergence of CTEV deformity after initial successful correction'),
bullet('Most relapses occur within first 2 years of life'),
bullet('Brace non-compliance = most common cause'),
P('', false),
H2('Management of Relapse:'),
makeTable(
['Age at Relapse', 'Dynamic Supination Only', 'Fixed Deformity (Equinus/Varus)'],
[
['<2 years', 'Recasting + FAO', 'Recasting series'],
['2–4 years', 'Recasting + TATT at ~2.5–4 yrs', 'Recasting + consider TATT'],
['>4 years', 'TATT (if ossification adequate)', 'Soft tissue + bony procedures'],
['>8–10 years', 'Bony procedures (Evans, Dwyer, cuboid)', 'Triple arthrodesis if very rigid'],
]
),
P('', false),
// ─── 11. RECENT EVIDENCE
H1('11. RECENT EVIDENCE (2023–2026)'),
makeTable(
['PMID', 'Study', 'Key Finding'],
[
['38015923', 'Wang et al. JBJS Am 2024 — Network meta-analysis of RCTs', 'Ponseti method superior to all other conservative and surgical methods; first-line recommendation confirmed'],
['37401473', 'Ghanem et al. J Pediatr Orthop B 2024 — RCT', 'Earlier Achilles tenotomy (earlier in casting) gives better early outcomes; "better early than late"'],
['39365806', 'Ferreira dos Santos et al. PLoS One 2024 — Systematic review', 'Ponseti works in myelodysplastic clubfoot but with higher relapse rates; adjunct bracing critical'],
['41272751', 'Shan et al. J Orthop Surg Res 2025 — Meta-analysis', 'Ponseti effective for neurogenic clubfoot; 70-75% correction rate vs. 95% in idiopathic'],
['40888800', 'Cosentino & Berger. J Pediatr Orthop B 2026 — Meta-analysis', 'Plaster of Paris and semirigid fibreglass casts equivalent in Ponseti method outcomes'],
['39134994', 'Moreira et al. BMC Musculoskelet Disord 2024 — Systematic review', 'Tibialis anterior tendon transfer pull-out fixation vs. other methods — comparable outcomes; no significant difference in fixation type'],
]
),
P('', false),
// ─── 12. CLASSIC LANDMARK ARTICLES
H1('12. CLASSIC LANDMARK ARTICLES'),
makeTable(
['Author / Year', 'Title / Contribution'],
[
['Ponseti & Smoley (1963)', '"Congenital Club Foot: The Results of Treatment" JBJS — described the serial casting method, talar head as fulcrum, Achilles tenotomy; basis of Ponseti method'],
['Kite (1930–1950s)', 'Earlier conservative method; applied force on calcaneocuboid joint (WRONG FULCRUM) — led to rocker-bottom deformity; Ponseti method corrected this error'],
['Turco (1971)', 'Single-stage posteromedial release via medial incision — defined surgical anatomy of clubfoot release'],
['McKay (1982)', 'Complete subtalar release through Cincinnati incision — comprehensive surgical release'],
['Carroll (1988)', 'Cincinnati incision for clubfoot — circumferential approach providing excellent exposure'],
['Dimeglio et al. (1995)', 'Classification system for CTEV — 20-point scoring; Grade I–IV; predictive of treatment'],
['Pirani et al. (2008)', 'Pirani scoring system — 6-sign, 0–6 scale; simple, reliable, predictive of Achilles tenotomy need'],
['Dobbs et al. (2004)', 'Long-term follow-up of Ponseti method — excellent outcomes at 30-year follow-up; confirmed Ponseti superiority'],
['Zionts et al.', 'Studies on brace compliance and its association with relapse — confirmed non-compliance as #1 relapse factor'],
['Simons (1977)', 'Analytical radiology of clubfoot — described talocalcaneal parallelism and radiographic measurements'],
]
),
P('', false),
// ─── 13. QUICK REVISION TABLES
pageBreak(),
H1('13. QUICK REVISION — HIGH-YIELD TABLES'),
H2('CTEV vs. Vertical Talus vs. Metatarsus Adductus — Differential'),
makeTable(
['Feature', 'CTEV', 'Congenital Vertical Talus', 'Metatarsus Adductus'],
[
['Heel position', 'Equinus + varus', 'Calcaneus + valgus (rocker-bottom)', 'Normal'],
['Forefoot', 'Adducted', 'Abducted (convex sole)', 'Adducted only'],
['Sole shape', 'Bean-shaped (concave lateral)', 'Convex (rocker-bottom)', 'C-shaped (medial concave)'],
['X-ray', 'Talocalcaneal parallelism; neg. talus-1st MT angle', 'Talocalcaneal angle INCREASED; talus vertical', 'Normal talocalcaneal; adducted forefoot'],
['Treatment', 'Ponseti casting', 'Reverse Ponseti/surgical', 'Stretching/casting; usually resolves'],
]
),
P('', false),
H2('Radiological Angles — Summary'),
makeTable(
['Measurement', 'View', 'Normal', 'CTEV Value'],
[
['Talocalcaneal (Kite) angle', 'AP', '20–40°', '< 20° (often 0–5°)'],
['Talocalcaneal angle', 'Lateral (DF view, Turco)', '35–50°', '< 35°'],
['Talo-1st MT angle', 'AP', '0 to +20°', 'Negative (< 0°)'],
['Calcaneal-1st MT angle', 'AP', 'Normal divergence', 'Parallel/convergent'],
]
),
P('', false),
H2('Ponseti Method Summary'),
makeTable(
['Phase', 'Duration', 'Key Detail'],
[
['Serial casting', '~5 casts weekly', 'Fulcrum = lateral talar head; CAVE → correct C, then AV, then E'],
['Achilles tenotomy', 'When needed (~90%)', 'Percutaneous; under LA; when <15° dorsiflexion remains'],
['Post-tenotomy cast', '3 weeks', '70° abduction + 10–15° dorsiflexion'],
['FAO full time', '3 months', '60–70° external rotation bilaterally'],
['FAO night-and-nap', '3–4 years', 'Compliance is mandatory — prevents relapse'],
]
),
P('', false),
// ─── 14. MCQs
pageBreak(),
H1('14. MCQ BANK — 10 QUESTIONS'),
H3('(Mixed DNB/MS Final + Fellowship Level)'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q1. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('A 3-day-old male infant has a right clubfoot. The correct order of deformity components in the Ponseti method of casting is:'),
bullet('A. Equinus → Varus → Adductus → Cavus'),
bullet('B. Cavus → Adductus + Varus → Equinus'),
bullet('C. Adductus → Varus → Cavus → Equinus'),
bullet('D. Equinus → Cavus → Adductus → Varus'),
highlight('Answer: B. Ponseti correction sequence: Cavus first (elevate 1st ray) → then Adductus + Varus simultaneously (using talar head as fulcrum) → then Equinus LAST (by percutaneous Achilles tenotomy). Mnemonic: "C-AV-E". Equinus is always corrected LAST.', 'E8F5E9'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q2. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('In Ponseti casting for CTEV, the fulcrum of correction is applied to:'),
bullet('A. Medial cuneiform'),
bullet('B. Calcaneocuboid joint'),
bullet('C. Lateral head of the talus'),
bullet('D. Navicular tuberosity'),
highlight('Answer: C. The head of the talus (specifically the LATERAL aspect) is the fulcrum. Counter-pressure is applied here while abducting the forefoot. Applying force over the calcaneocuboid joint (Kite\'s method) causes rocker-bottom deformity.', 'E8F4FD'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q3. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('After completing 5 Ponseti casts, a 6-week-old infant has 0° of dorsiflexion. The abduction has been corrected to 60°. What is the next step?'),
bullet('A. Continue casting for 2 more weeks hoping for spontaneous improvement'),
bullet('B. Apply the final cast in maximum dorsiflexion'),
bullet('C. Perform percutaneous Achilles tenotomy under local anesthesia'),
bullet('D. Proceed to posteromedial surgical release'),
highlight('Answer: C. When residual equinus (<15° dorsiflexion) persists after adequate abduction correction, percutaneous Achilles tenotomy is performed (~90% of cases). The tendon is divided percutaneously under LA in clinic. A final cast is then placed for 3 weeks in 70° abduction and 10–15° dorsiflexion.', 'FFF9C4'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q4. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('The most common cause of relapse in clubfoot treated by the Ponseti method is:'),
bullet('A. Inadequate number of casts'),
bullet('B. Non-compliance with foot abduction orthosis (brace)'),
bullet('C. Incorrect fulcrum during casting'),
bullet('D. Failure to perform Achilles tenotomy'),
highlight('Answer: B. Non-compliance with the Foot Abduction Orthosis (FAO/Denis Browne brace) is the SINGLE MOST COMMON cause of relapse. With good compliance, relapse is <10%. Without brace use, relapse can reach 80%.', 'FFE0E0'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q5. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('A 3-year-old child treated with Ponseti casting as a neonate now presents with dynamic supination of the right foot (foot supinates on walking). Examination shows a flexible foot with no fixed deformity. The most appropriate surgical treatment is:'),
bullet('A. Posterior medial soft tissue release'),
bullet('B. Tibialis anterior tendon transfer to the 3rd cuneiform/cuboid'),
bullet('C. Calcaneal osteotomy'),
bullet('D. Triple arthrodesis'),
highlight('Answer: B. Tibialis anterior tendon transfer (TATT) is the treatment of choice for dynamic supination relapse in children aged 2.5–4 years. The tibialis anterior is transferred from the 1st cuneiform to the 3rd cuneiform (or cuboid) to rebalance the foot. This is effective and avoids formal release.', 'E8F5E9'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q6. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('The Pirani scoring system in CTEV evaluates 6 clinical signs. Which of the following is NOT part of the Pirani score?'),
bullet('A. Lateral curvature of the foot border'),
bullet('B. Empty heel sign'),
bullet('C. Tibial torsion'),
bullet('D. Posterior heel crease'),
highlight('Answer: C. Tibial torsion is NOT part of the Pirani score. The 6 signs are: (Midfoot) 1. Curvature of lateral border, 2. Lateral head of talus, 3. Medial crease. (Hindfoot) 4. Posterior crease, 5. Empty heel, 6. Rigid equinus.', 'E8F4FD'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q7. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('"Rocker-bottom deformity" as a complication of CTEV casting is caused by:'),
bullet('A. Applying pressure over the lateral talar head'),
bullet('B. Using the calcaneocuboid joint as a fulcrum during correction'),
bullet('C. Performing Achilles tenotomy too early'),
bullet('D. Over-abducting the foot beyond 70 degrees'),
highlight('Answer: B. This is the CLASSIC error of Kite\'s method — applying counter-pressure over the calcaneocuboid joint acts as a fulcrum that dorsifleXes the FOREFOOT (midfoot break) while leaving hindfoot equinus uncorrected. This creates a rocker-bottom/flatfoot deformity. Ponseti corrected this by using the TALAR HEAD as the fulcrum.', 'FFF9C4'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q8. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('On AP X-ray of a clubfoot, which radiological finding is PATHOGNOMONIC?'),
bullet('A. Increased talocalcaneal angle > 50°'),
bullet('B. Positive talus-1st metatarsal angle > 20°'),
bullet('C. Parallelism of talus and calcaneus (talocalcaneal angle < 20°) + negative talo-1st metatarsal angle'),
bullet('D. Calcaneal pitch > 30°'),
highlight('Answer: C. The hallmark X-ray finding is PARALLELISM of the talus and calcaneus with Kite angle (talocalcaneal angle) < 20° on AP view (normal 20–40°), AND a NEGATIVE talo-1st metatarsal angle (normally 0–+20°). Parallelism is seen on BOTH AP and lateral views.', 'E8F4FD'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q9. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('In the Dimeglio classification for CTEV, a foot scoring Grade IV (16–20 points) is best described as:'),
bullet('A. Soft, benign; easily correctable by manipulation'),
bullet('B. Moderate; partially reducible; responds to Ponseti'),
bullet('C. Stiff, partially reducible; some resistance to correction'),
bullet('D. Rigid, irreducible; teratologic type; requires surgery'),
highlight('Answer: D. Dimeglio Grade IV (score 16–20) = "very severe" = rigid, irreducible = teratologic clubfoot. Accounts for ~12% of cases. These typically require surgical treatment. Grade I = benign/soft (20%). Grade II = moderate (33%). Grade III = severe/stiff (35%).', 'E8F5E9'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q10. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('A 9-year-old with neglected bilateral CTEV presents with rigid deformity and difficulty walking. The MOST appropriate surgical management is:'),
bullet('A. Ponseti casting + Achilles tenotomy'),
bullet('B. Tibialis anterior tendon transfer'),
bullet('C. Posteromedial soft tissue release (McKay/Cincinnati)'),
bullet('D. Triple arthrodesis or Ilizarov frame correction'),
highlight('Answer: D. In a neglected CTEV at age 9 with RIGID deformity, soft tissue procedures are inadequate (foot too stiff). Triple arthrodesis (fusing subtalar + talonavicular + calcaneocuboid joints) is the definitive procedure for rigid CTEV in late-presenting older children/adults. Ilizarov/Taylor spatial frame correction is an alternative allowing gradual correction without arthrodesis.', 'FFE0E0'),
P('', false),
divider(),
new Paragraph({ children: [new TextRun({ text: "END OF CTEV NOTES | Prepared July 2026 | Sources: Miller's Review 9e, Bailey & Love 28e, Campbell's 15e, PubMed 2023–2026", color: '7F7F7F', size: 18 })], alignment: AlignmentType.CENTER, spacing: { before: 200 } }),
]
}]
});
Packer.toBuffer(doc).then(buffer => {
fs.writeFileSync('/home/daytona/workspace/ddh-notes/CTEV_Ortho_PG_Notes.docx', buffer);
console.log('CTEV DOCX created successfully');
});
A comprehensive medical visual mind map poster for CTEV (Congenital Talipes Equinovarus / Clubfoot) for orthopaedic postgraduate exam revision. Central node "CTEV / CLUBFOOT" with clearly labeled branches: 1) DEFORMITY branch showing CAVE mnemonic diagram: Cavus (elevated arch), Adductus (forefoot medial), Varus (hindfoot inverted), Equinus (plantarflexed) with foot silhouette showing all components. 2) EPIDEMIOLOGY: Boys 2x more, 50% bilateral, 1-6 per 1000 live births. 3) PATHOLOGY: Talar neck medial deviation, navicular subluxed medially, talocalcaneal parallelism, anterior tibial artery absent. 4) CLASSIFICATION branch: Pirani score 0-6 (3 midfoot + 3 hindfoot signs), Dimeglio Grade I-IV (0-20 points). 5) PONSETI METHOD central box with flowchart: Cast 1 (Cavus) → Casts 2-4 (Adductus+Varus using lateral talar head as fulcrum) → Achilles tenotomy 90% → Final cast 70° abduction → FAO brace 3-4 years. Include "FULCRUM = LATERAL TALAR HEAD" highlighted. 6) COMPLICATIONS: Rocker-bottom (from calcaneocuboid fulcrum = Kite's mistake), Flat-top talus, Dynamic supination (treat with TATT), Relapse (FAO non-compliance #1 cause). 7) SURGERY when needed: Posteromedial release (Cincinnati incision), TATT for relapse, Triple arthrodesis for neglected. 8) X-RAY box showing AP Kite angle less than 20 degrees (normal 20-40), Lateral talocalcaneal angle less than 35 degrees, negative talo-1st MT angle. Color coded with red for equinus/warnings, green for normal values, blue for treatment, orange for key landmarks. Professional medical infographic style, white background, anatomical foot diagrams included.
cd /home/daytona/workspace/ddh-notes && node create_ctev_notes.js 2>&1
ls -lh /home/daytona/workspace/ddh-notes/ && python3 -c "import zipfile; z = zip…
CONGENITAL TALIPES EQUINOVARUS (CTEV) — CLUBFOOT
Complete PG Orthopaedics Notes | DNB / MS Final + Fellowship Level
📥 Downloads
CTEV Ortho PG Notes
Word Document · DOCX
🗺️ Visual Mind Map Poster
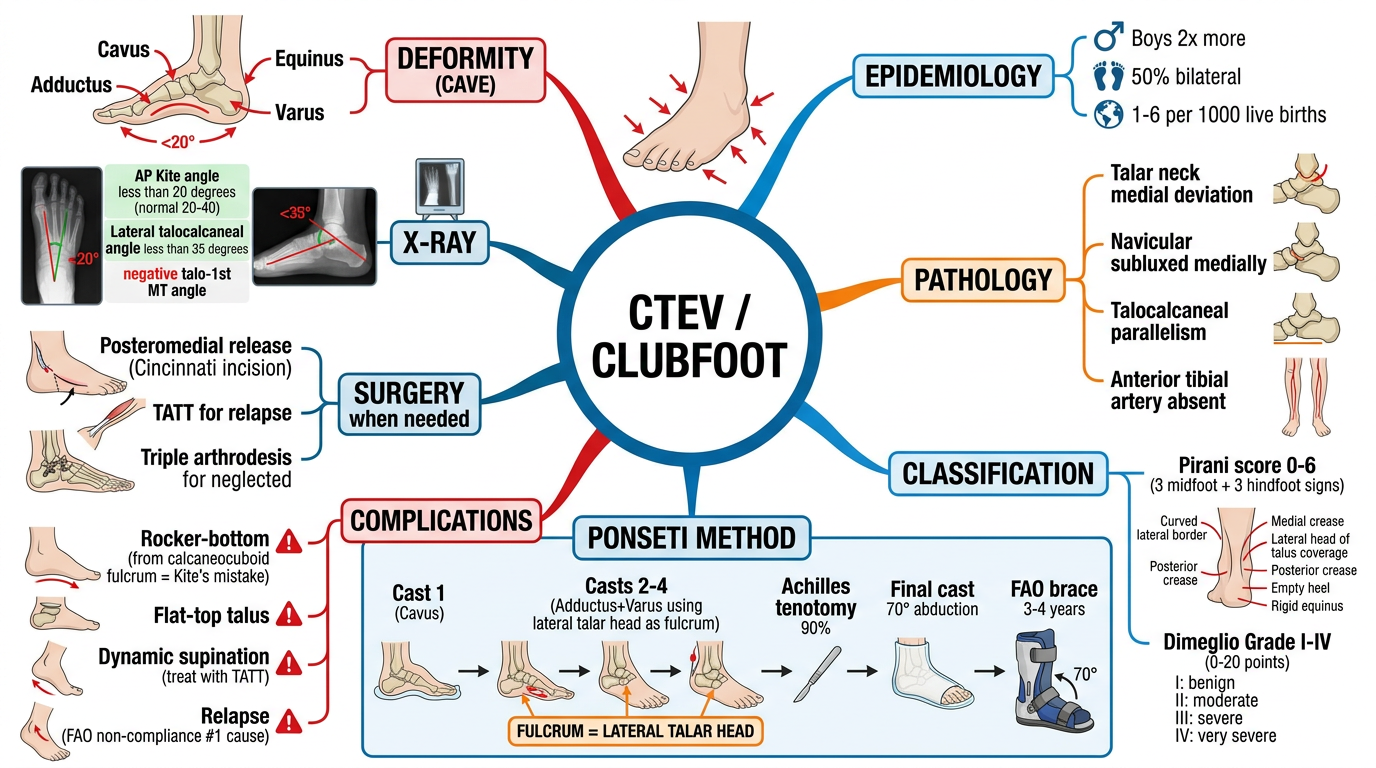
1. DEFINITION — The CAVE Deformity
| Component | Deformity | Structure Involved |
|---|---|---|
| C — Cavus | Elevated longitudinal arch; pronation of forefoot relative to hindfoot | Plantar fascia, intrinsic muscles |
| A — Adductus | Forefoot adduction at midtarsal joint | Talonavicular joint subluxation |
| V — Varus | Hindfoot inverted; calcaneus in varus | Subtalar joint; calcaneofibular ligament |
| E — Equinus | Plantarflexion of hindfoot; cannot dorsiflex | Shortened Achilles tendon; posterior capsule |
MNEMONIC — CAVE (deformity) and CAVE order of correction (C first → A+V together → E last by tenotomy)
2. EPIDEMIOLOGY
| Parameter | Value |
|---|---|
| Incidence | 1–6 per 1,000 live births |
| Sex ratio | Boys : Girls = 2:1 |
| Bilateral | 50% of cases |
| Family history | Multifactorial; increases risk 10–30x |
| Associated with spina bifida | Neuromuscular CTEV — harder to treat |
Types of CTEV:
| Type | Description | Treatment |
|---|---|---|
| Postural | Flexible; passively correctable to neutral; NOT true CTEV | Physiotherapy only; normal by 3 months |
| Idiopathic (structural) | Fixed; empty heel; deep creases; MOST COMMON | Ponseti — 95% success |
| Neuromuscular | Spina bifida, arthrogryposis; stiffer | Ponseti with higher relapse; often surgery |
| Syndromic/Teratologic | Trisomy 18, diastrophic dwarfism, amniotic band | Surgical; poor prognosis |
3. ETIOLOGY & PATHOLOGY
PRIMARY Bony Change:
- Talar neck is deviated medially and plantarward — the KEY bony abnormality
- Navicular displaced medially on talar head (talonavicular subluxation)
- Calcaneus: medially rotated, inverted, "parallel" to talus under talus
Soft Tissue Changes:
- Shortened: Achilles tendon, tibialis posterior, FHL, FDL, plantar fascia, posterior capsule, calcaneofibular ligament
- Muscles: Gastrocsoleus + tibialis posterior smaller than normal, increased connective tissue
Vascular:
- Anterior tibial artery absent or diminutive in many cases
- Dorsalis pedis may be diminished — protect posterior tibial artery during surgery
"All roads lead to the talus" — talar neck deformity is the primary defect; ALL Ponseti corrections use the HEAD OF THE TALUS as fulcrum
4. CLINICAL FEATURES
The "Empty Heel" Sign — PATHOGNOMONIC
- Heel appears and feels empty on palpation — calcaneus pulled upward by tight Achilles
- Deep posterior crease = equinus
- Deep medial crease = varus/adductus at talonavicular level
- Small calf + small foot on affected side
Postural vs. Structural:
| Feature | Postural | Structural CTEV |
|---|---|---|
| Passively correctable | YES | NO — fixed |
| Empty heel | No | Yes |
| Deep creases | Absent | Present |
| Treatment | Stretching | Ponseti casting |
5. SCORING SYSTEMS
A. Pirani Score (0–6) — MOST WIDELY USED
| Zone | Sign |
|---|---|
| MIDFOOT (3) | 1. Curvature of lateral border |
| 2. Lateral head of talus prominence | |
| 3. Medial crease depth | |
| HINDFOOT (3) | 4. Posterior crease depth |
| 5. Empty heel sign | |
| 6. Rigid equinus |
Pirani > 3.5 = Achilles tenotomy very likely needed. Higher score = more casts needed. Score at time of bracing predicts relapse risk.
B. Dimeglio Classification (0–20)
| Grade | Score | Description | % Cases |
|---|---|---|---|
| I — Benign | ≤ 5 | Soft; easily correctable | 20% |
| II — Moderate | 6–10 | Partially reducible | 33% |
| III — Severe | 11–15 | Stiff; partially reducible | 35% |
| IV — Very Severe | 16–20 | Rigid; irreducible; teratologic | 12% |
6. INVESTIGATIONS
Radiography (used after ossification / operative planning)
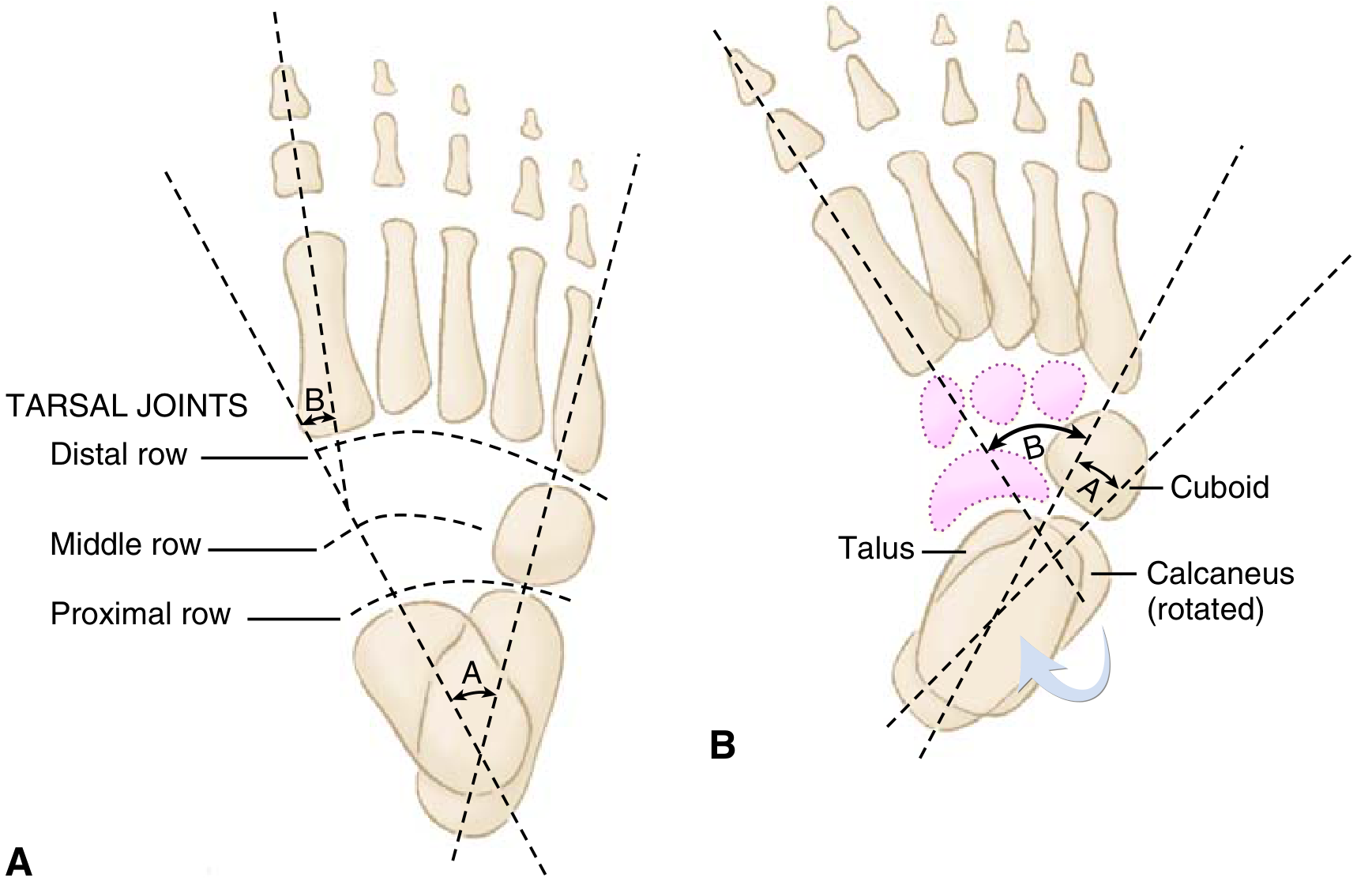
| Measurement | View | Normal | CTEV |
|---|---|---|---|
| Talocalcaneal (Kite) angle | AP | 20–40° | < 20° (often 0–5°) |
| Talo-1st metatarsal angle | AP | 0 to +20° | NEGATIVE (< 0°) |
| Talocalcaneal angle (Turco view) | Lateral dorsiflexion | 35–50° | < 35° |
| Talocalcaneal parallelism | Both views | Divergent | Parallel on both views |
KEY X-RAY SIGN: Parallelism of talus and calcaneus on BOTH AP and lateral views + negative talo-1st MT angle = diagnostic
7. TREATMENT

PONSETI METHOD — Gold Standard (95% success in idiopathic CTEV)
PHASE 1: SERIAL CASTING (~5 casts, weekly)
─────────────────────────────────────────
Cast 1: Correct CAVUS
→ Supinate forefoot; elevate 1st ray
→ Do NOT abduct yet
Casts 2–4: Correct ADDUCTUS + VARUS simultaneously
→ Counter-pressure on LATERAL TALAR HEAD (fulcrum)
→ Abduct forefoot 60–70° external rotation
→ Knee at 90° (long-leg cast)
⚠️ NEVER apply force on calcaneocuboid joint
(that's Kite's method → causes rocker-bottom!)
PHASE 2: ACHILLES TENOTOMY (~90% of cases)
─────────────────────────────────────────
→ When <15° dorsiflexion after adequate abduction
→ Percutaneous; under LOCAL ANESTHESIA in clinic
→ Final cast: 70° abduction + 10–15° dorsiflexion × 3 WEEKS
→ Tendon regenerates in cast in 3 weeks
PHASE 3: FOOT ABDUCTION ORTHOSIS (Denis Browne / FAO)
─────────────────────────────────────────────────────
→ 60–70° external rotation bilaterally
→ Full time (23 hrs/day) × 3 MONTHS
→ Night + nap time × 3–4 YEARS total
→ NON-COMPLIANCE = #1 cause of RELAPSE
8. SURGICAL TREATMENT
A. Posteromedial Release (PMR)
- Indication: Failed Ponseti (~5% idiopathic); neuromuscular CTEV; before walking age
- Incisions: Cincinnati (best exposure) > McKay > Turco
- Structures released: Achilles (Z-plasty), tibialis posterior, FHL, FDL, posterior capsule, talonavicular capsule, calcaneofibular ligament
- Protect posterior tibial artery — dominant supply in CTEV
B. Tibialis Anterior Tendon Transfer (TATT)
- Indication: Dynamic supination relapse at age 2.5–4 years
- Transfer: 1st cuneiform → 3rd cuneiform or cuboid
- Rebalances foot; prevents supination
C. Bony Procedures (Older Children/Neglected)
| Procedure | Age | Indication |
|---|---|---|
| Cuboid decancellation / Lateral column shortening | 3–10 yrs | Residual forefoot adductus |
| Evans calcaneal osteotomy | 5+ yrs | Lateral column lengthening |
| Dwyer calcaneal osteotomy | Older | Residual hindfoot varus |
| Triple arthrodesis | >10–12 yrs | Neglected rigid CTEV |
| Ilizarov frame | Any age | Complex recurrent/resistant cases |
9. COMPLICATIONS
| Complication | Cause | Prevention/Treatment |
|---|---|---|
| Relapse (most common) | FAO non-compliance | Recasting + TATT |
| Rocker-bottom (iatrogenic) | Force on calcaneocuboid joint (Kite's error); dorsiflexing forefoot before correcting varus | Use talar head as fulcrum ALWAYS |
| Flat-top talus | Forceful dorsiflexion → talar dome pressure | Use Achilles tenotomy; avoid force |
| Dynamic supination | 15–20%; tibialis anterior overpull | TATT at 2.5–4 years |
| Dorsal bunion | Post-surgical; iatrogenic peroneus longus division | Capsulotomy + FHL lengthening |
| Overcorrection (pes valgus) | Excessive abduction/surgery | Rare with Ponseti |
| Wound dehiscence | Cincinnati incision | Secondary healing — usually fine |
| AVN of talus | Vascular injury; forced correction | Prevention; conservative |
Classic Exam Trap: "Rocker-bottom caused by applying pressure over calcaneocuboid joint" = Kite's MISTAKE that Ponseti corrected by shifting the fulcrum to the talar head.
10. DIFFERENTIAL DIAGNOSIS
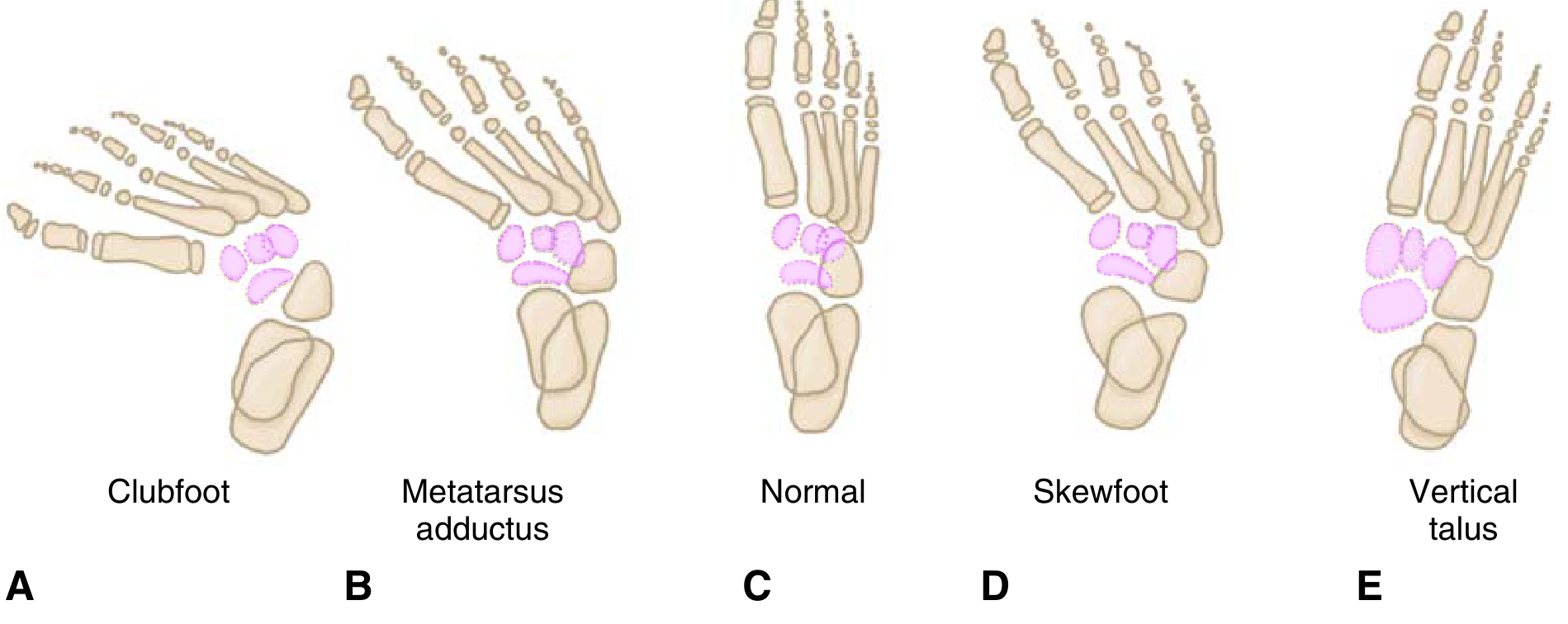
| Feature | CTEV | Vertical Talus | Metatarsus Adductus |
|---|---|---|---|
| Heel | Equinus + varus | Calcaneus + valgus | Normal |
| Foot appearance | Bean-shaped; concave lateral | Convex (rocker-bottom) | C-shaped |
| Correctability | Fixed | Fixed | Often flexible |
| X-ray | Talocalcaneal parallelism; negative talo-MT angle | Talus vertical; increased TC angle | Normal TC angle; adducted forefoot |
| Treatment | Ponseti casting | Reverse Ponseti/surgery | Stretching/serial casting |
11. RECENT EVIDENCE (2023–2026)
| PMID | Study | Key Finding |
|---|---|---|
| 38015923 | Wang et al. JBJS 2024 — Network meta-analysis | Ponseti method superior to all alternatives; confirmed as standard of care |
| 37401473 | Ghanem et al. 2024 — RCT | Achilles tenotomy earlier in casting process gives better early outcomes |
| 39365806 | Ferreira dos Santos 2024 — Systematic review | Ponseti effective in myelodysplastic CTEV; higher relapse rate than idiopathic |
| 41272751 | Shan et al. 2025 — Meta-analysis | Ponseti for neurogenic clubfoot: 70–75% success vs. 95% idiopathic |
| 40888800 | Cosentino & Berger 2026 — Meta-analysis | POP and semirigid fiberglass casts equivalent for Ponseti casting |
12. CLASSIC LANDMARK ARTICLES
| Author / Year | Contribution |
|---|---|
| Ponseti & Smoley (1963) | Classic JBJS paper — serial casting with talar head as fulcrum; foundation of Ponseti method |
| Kite (1930s–1950s) | Older casting using calcaneocuboid as fulcrum — caused rocker-bottom; Ponseti corrected this error |
| Turco (1971) | Single-stage PMR via medial incision — defined surgical anatomy |
| McKay (1982) | Complete subtalar release — comprehensive surgical technique |
| Carroll (1988) | Cincinnati incision — circumferential approach with best exposure |
| Dimeglio et al. (1995) | 20-point classification — Grade I–IV; widely used worldwide |
| Pirani et al. (2008) | 6-sign scoring system — simple, reliable, predictive of tenotomy |
| Dobbs et al. (2004) | 30-year follow-up of Ponseti — confirmed excellent long-term outcomes; superiority over surgery |
| Simons (1977) | Analytical radiology of clubfoot — talocalcaneal parallelism measurements |
| Zionts et al. | Brace compliance research — non-compliance = #1 relapse predictor |
13. KEY MNEMONICS
| Mnemonic | Meaning |
|---|---|
| CAVE | Deformity components: Cavus, Adductus, Varus, Equinus |
| "C first, AV together, E last" | Ponseti correction order |
| Fulcrum = TALAR HEAD | NEVER calcaneocuboid (= rocker-bottom) |
| "3 weeks — 3 months — 3 years" | Post-tenotomy cast: 3 wks; FAO full time: 3 months; FAO night: 3 yrs |
| Non-compliance = Relapse | #1 cause of recurrence is brace non-compliance |
| 90% need tenotomy | ~90% of idiopathic CTEV require Achilles tenotomy |
14. 10 MCQs — Mixed DNB/MS + Fellowship Level
osteomyelitis
"osteomyelitis"[MeSH Terms] AND "diagnosis"[MeSH Terms]
osteomyelitis Cierny-Mader classification Waldvogel classification landmark articles chronic osteomyelitis management 2024
"osteomyelitis"[MeSH Terms] AND "antibiotic"[All Fields]
Cierny Mader staging osteomyelitis type 1 2 3 4 host class A B C surgical treatment algorithm
~/ddh-notes/create_osteo_notes.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
HeadingLevel, AlignmentType, WidthType, ShadingType, VerticalAlign, PageBreak
} = require('docx');
const fs = require('fs');
const H1 = t => new Paragraph({ text: t, heading: HeadingLevel.HEADING_1, spacing: { before: 360, after: 120 } });
const H2 = t => new Paragraph({ text: t, heading: HeadingLevel.HEADING_2, spacing: { before: 240, after: 80 } });
const H3 = t => new Paragraph({ text: t, heading: HeadingLevel.HEADING_3, spacing: { before: 180, after: 60 } });
const P = (t, bold=false) => new Paragraph({ children: [new TextRun({ text: t, bold })], spacing: { before: 60, after: 60 } });
const bullet = (t, bold=false, level=0) => new Paragraph({ children: [new TextRun({ text: t, bold })], bullet: { level }, spacing: { before: 40, after: 40 } });
const divider = () => new Paragraph({ children: [new TextRun({ text: '─'.repeat(80), color: '999999' })], spacing: { before: 120, after: 120 } });
const PB = () => new Paragraph({ children: [new PageBreak()] });
const HL = (t, c='E8F5E9') => new Paragraph({ children: [new TextRun({ text: t, bold: true })], shading: { type: ShadingType.CLEAR, fill: c }, spacing: { before: 80, after: 80 }, indent: { left: 200 } });
const makeTable = (headers, rows, hColor='1F4E79') => {
const hr = new TableRow({ children: headers.map(h => new TableCell({ children: [new Paragraph({ children: [new TextRun({ text: h, bold: true, color: 'FFFFFF' })], alignment: AlignmentType.CENTER })], shading: { type: ShadingType.CLEAR, fill: hColor }, verticalAlign: VerticalAlign.CENTER })) });
const dr = rows.map(row => new TableRow({ children: row.map((c, i) => new TableCell({ children: [new Paragraph({ children: [new TextRun({ text: String(c) })], alignment: AlignmentType.CENTER })], shading: { type: ShadingType.CLEAR, fill: i === 0 ? 'D6E4F0' : 'FFFFFF' } })) }));
return new Table({ rows: [hr, ...dr], width: { size: 100, type: WidthType.PERCENTAGE } });
};
const doc = new Document({
title: 'Osteomyelitis - Comprehensive PG Orthopaedics Notes',
sections: [{ children: [
new Paragraph({ children: [new TextRun({ text: 'OSTEOMYELITIS', bold: true, size: 48, color: '1F4E79' })], alignment: AlignmentType.CENTER, spacing: { before: 400, after: 200 } }),
new Paragraph({ children: [new TextRun({ text: 'Comprehensive PG Orthopaedics Study Notes | DNB / MS / Fellowship Level', color: '7F7F7F', size: 24 })], alignment: AlignmentType.CENTER }),
new Paragraph({ children: [new TextRun({ text: "Sources: Campbell's 15e 2026 | Robbins & Kumar Pathology | Bailey & Love 28e | PubMed 2023–2026", color: '7F7F7F', size: 20 })], alignment: AlignmentType.CENTER, spacing: { after: 400 } }),
divider(),
H1('1. DEFINITION'),
P('Osteomyelitis is inflammation of bone and bone marrow, virtually always caused by infection. It may arise by hematogenous spread, extension from a contiguous focus, or direct inoculation (open fracture, surgery).'),
P('', false),
HL('KEY: Staphylococcus aureus causes 80–90% of culture-positive pyogenic osteomyelitis. S. aureus cell wall proteins bind to bone matrix collagen, facilitating adherence.', 'E8F4FD'),
PB(),
H1('2. CLASSIFICATION'),
H2('A. Waldvogel Classification (1970) — MOST WIDELY USED clinically'),
makeTable(
['Category', 'Sub-type', 'Description'],
[
['By Pathogenesis', 'Hematogenous', 'Bacteremia → metaphyseal seeding; mainly children; single organism'],
['', 'Contiguous focus (without vascular insufficiency)', 'Post-trauma, post-surgery, soft tissue spread; mixed organisms; adults'],
['', 'Contiguous focus (with vascular insufficiency)', 'Diabetic foot, PVD; polymicrobial; poor healing; elderly'],
['By Duration', 'Acute', 'Onset to presentation <2 weeks (some: <6 weeks)'],
['', 'Subacute', '2 weeks to 3 months; Brodie abscess'],
['', 'Chronic', '>3 months; sequestrum + involucrum present'],
]
),
P('', false),
H2('B. Cierny-Mader Classification (1985) — BEST for surgical planning of CHRONIC osteomyelitis'),
H3('Part 1 — Anatomic Staging:'),
makeTable(
['Stage', 'Type', 'Bone Involvement', 'Example'],
[
['Stage I', 'Medullary', 'Infection confined to medullary canal', 'Hematogenous OM; infected IM nail'],
['Stage II', 'Superficial', 'Cortical surface only; no medullary involvement', 'Contiguous spread; post-radiation'],
['Stage III', 'Localized', 'Full-thickness cortical + medullary but stable (sequestrum does NOT compromise stability)', 'Localized chronic OM'],
['Stage IV', 'Diffuse', 'Involves entire bone circumference; UNSTABLE (removal of bone = instability)', 'Infected nonunion; diffuse chronic OM'],
]
),
P('', false),
H3('Part 2 — Host Physiologic Classification:'),
makeTable(
['Host Class', 'Description', 'Systemic Factors (Bs)', 'Local Factors (Bl)'],
[
['A-Host', 'Normal — no compromise; standard treatment', '—', '—'],
['B-Host (Bs)', 'Systemic compromise', 'Malnutrition, DM, CRF, immune suppression, malignancy, HIV, extremes of age', '—'],
['B-Host (Bl)', 'Local compromise', '—', 'Chronic lymphedema, venous stasis, vascular disease, scarring, radiation fibrosis, neuropathy, tobacco abuse'],
['B-Host (Bls)', 'Both systemic + local', 'Combined', 'Combined'],
['C-Host', 'Treatment is WORSE than the disease; no cure attempted', 'Treatment morbidity > disease morbidity', 'Suppressive therapy only'],
]
),
P('', false),
HL('CIERNY-MADER TREATMENT PRINCIPLE: Stage I & II → Often antibiotics ± limited surgery. Stage III & IV → Aggressive surgical debridement + 4–6 weeks antibiotics. Class C Host → Suppressive therapy only (no curative surgery).', 'FFF9C4'),
P('', false),
H2('C. By Age / Special Types'),
makeTable(
['Type', 'Key Feature'],
[
['Neonatal (0–1 month)', 'Metaphyseal vessels cross growth plate → epiphysis + joint infected simultaneously → septic arthritis common; Group B Strep + E. coli + S. aureus'],
['Childhood (1–16 years)', 'Metaphyseal vessels loop without crossing growth plate → metaphysis only; S. aureus #1'],
['Adult', 'Growth plate closure → anastomosis of metaphyseal + epiphyseal vessels → subchondral + epiphyseal involved; contiguous/post-surgical more common'],
['Diabetic foot osteomyelitis', 'Contiguous from ulcer; polymicrobial; calcaneus most common; "probe to bone" test positive'],
['Vertebral (spondylodiscitis)', 'Adults >50; L4-L5 most common; S. aureus or TB (Pott\'s disease); MRI gold standard'],
['Brodie Abscess', 'Subacute; walled-off metaphyseal abscess; children; X-ray: lytic lesion + sclerotic rim + periosteal reaction; mimics tumour'],
['Garre Sclerosing OM', 'Chronic; non-suppurative; diffuse sclerosis + periosteal thickening; mandible most common; Actinomyces'],
['Post-traumatic / Implant', 'Contiguous; mixed organisms; biofilm on implant; very difficult to treat'],
]
),
P('', false),
PB(),
H1('3. PATHOPHYSIOLOGY & PATHOLOGY'),
H2('A. Why Metaphysis?'),
bullet('Slow blood flow through looped metaphyseal sinusoidal vessels → bacterial seeding during bacteremia'),
bullet('Microtrauma facilitates lodgment of bacteria at metaphysis'),
bullet('Lack of phagocytes in metaphyseal sinusoids → bacteria multiply unopposed'),
P('', false),
H2('B. Sequence of Events — Acute Hematogenous Osteomyelitis'),
makeTable(
['Timeline', 'Pathological Event'],
[
['Hour 0', 'Bacteremia → bacteria seed metaphyseal sinusoidal vessels → bacterial colonies form'],
['0–48 hours', 'Neutrophilic infiltrate; bone cell necrosis; pus forms under pressure in medullary canal'],
['48–72 hours', 'Pus tracks through Haversian canals → subperiosteal space → periosteal elevation → cortical bone becomes avascular'],
['Day 3–7', 'Periosteal lifting → cortical AVN → SEQUESTRUM formation (dead cortical bone devoid of blood supply)'],
['Week 2+', 'Reactive new bone formation from periosteum = INVOLUCRUM (shell of new living bone surrounding dead bone)'],
['Chronic phase', 'INVOLUCRUM = outer shell; SEQUESTRUM = inner dead bone; CLOACA = opening/hole in involucrum through which pus drains; SINUS TRACT = track to skin'],
]
),
P('', false),
HL('KEY TERMS — MUST KNOW:\n• SEQUESTRUM = dead devascularized necrotic cortical bone (avascular; no antibiotic penetration)\n• INVOLUCRUM = reactive new periosteal bone shell around sequestrum\n• CLOACA = opening in involucrum through which pus/sequestrum may discharge\n• SINUS TRACT = track from cloaca to skin surface', 'FFE0E0'),
P('', false),
H2('C. Why Antibiotics Fail in Chronic Osteomyelitis'),
bullet('Sequestrum is avascular — antibiotics cannot penetrate dead bone'),
bullet('Biofilm formation on dead bone and implants — bacteria in biofilm resist antibiotics'),
bullet('Host tissue fibrosis impairs immune cell delivery'),
bullet('Polymicrobial infection in contiguous/diabetic OM'),
P('', false),
PB(),
H1('4. MICROBIOLOGY BY CLINICAL SETTING'),
makeTable(
['Clinical Setting', 'Most Common Organism(s)', 'Key Notes'],
[
['Healthy child (all ages)', 'S. aureus (#1 always)', '80–90% of culture-positive cases'],
['Neonate (0–1 month)', 'Group B Strep, E. coli, S. aureus', 'Multiple joints often involved'],
['Sickle cell disease', 'Salmonella (#1 in SCD) > S. aureus', 'Loss of splenic function + bone infarcts'],
['IV drug user', 'Pseudomonas aeruginosa, Candida, S. aureus', 'Vertebral; sternoclavicular; pubic symphysis'],
['Immunocompromised / HIV', 'S. aureus, Candida, Aspergillus, mycobacteria', 'Unusual organisms possible'],
['Post-surgical / implant', 'S. epidermidis (coagulase-negative), S. aureus, mixed', 'Biofilm formers; difficult to eradicate'],
['Diabetic foot osteomyelitis', 'Polymicrobial: S. aureus, Streptococcus, gram-neg, anaerobes', 'Probe-to-bone test + MRI key for diagnosis'],
['Vertebral OM (developed world)', 'S. aureus, gram-negatives', 'Via Batson venous plexus'],
['Vertebral OM (developing world)', 'M. tuberculosis (Pott\'s disease)', 'L1-L2 most common; anterior vertebral body'],
['Puncture wound (foot)', 'Pseudomonas aeruginosa', 'Through rubber-soled shoe'],
['Cat/dog bite', 'Pasteurella multocida', 'Rapidly progressive'],
['Human bite / fight bite', 'Eikenella corrodens + mixed oral flora', 'Metacarpal head; very destructive'],
['Open fracture', 'Mixed: S. aureus, Pseudomonas, Enterobacter', 'Contamination-based'],
]
),
HL('EXAM TRAP: Sickle cell disease → Salmonella is the CLASSIC answer (though S. aureus is still actually more common in SCD too — but Salmonella is what exams test!)', 'FFE0E0'),
P('', false),
PB(),
H1('5. CLINICAL FEATURES'),
H2('A. Acute Hematogenous Osteomyelitis (Children)'),
bullet('Acute onset fever, malaise, rigors (systemic sepsis signs)'),
bullet('Intense throbbing pain over metaphysis'),
bullet('Tenderness, warmth, swelling over metaphysis'),
bullet('Pseudoparalysis — refusal to use the limb (especially in infants)'),
bullet('Limb held in semi-flexion'),
bullet('Local lymphadenopathy'),
P('', false),
H2('B. Subacute Osteomyelitis (Brodie Abscess)'),
bullet('Milder; insidious onset; localized bone pain'),
bullet('No systemic sepsis signs usually'),
bullet('X-ray: lytic lesion with sclerotic rim at metaphysis'),
bullet('Classified by Roberts et al. (Types I–VI based on X-ray appearance)'),
P('', false),
H2('C. Chronic Osteomyelitis'),
bullet('Long history; intermittent flares; sinus tract with discharge'),
bullet('"Quiet intervals" between acute exacerbations'),
bullet('Thickened, tender bone on palpation'),
bullet('Sinus tract / discharging wound'),
bullet('Limb shortening, deformity from growth arrest'),
bullet('Malignant change in sinus tract (squamous cell carcinoma / Marjolin\'s ulcer) — rare, long-standing'),
P('', false),
H2('D. Diabetic Foot Osteomyelitis'),
bullet('"Probe to bone" test — positive if bone felt with metal probe through ulcer (90% PPV for OM)'),
bullet('Painless due to neuropathy; usually overlying ulcer'),
bullet('Calcaneus and metatarsals most commonly affected'),
P('', false),
PB(),
H1('6. INVESTIGATIONS'),
H2('A. Blood Tests'),
makeTable(
['Test', 'Sensitivity / Specificity', 'Notes'],
[
['WBC', 'Low sensitivity in chronic OM', 'Raised in acute hematogenous OM'],
['ESR', 'Raised in 90%', 'Lags — takes weeks to normalise; useful for monitoring'],
['CRP', 'Raised early; normalises in 7–10 days with treatment', 'BEST for monitoring treatment response'],
['Procalcitonin (PCT)', 'Good (meta-analysis PMID 36421016: high Se/Sp in children)', 'Better than CRP for bacterial vs. non-bacterial'],
['Blood cultures', '+ve in 50% of acute hematogenous', 'Before antibiotics; guides treatment'],
]
),
P('', false),
H2('B. Microbiology'),
bullet('Blood cultures BEFORE antibiotics — positive in 50% acute hematogenous'),
bullet('Bone biopsy / aspiration for culture — definitive; guided by imaging'),
bullet('Sinus tract culture — UNRELIABLE; does NOT correlate with bone pathogen (except S. aureus)'),
bullet('16S rRNA PCR — identifies organisms in culture-negative cases'),
P('', false),
H2('C. Imaging'),
makeTable(
['Modality', 'Timing of Positivity', 'Findings in OM', 'Best Use'],
[
['Plain X-ray (first-line)', 'Positive in 10–21 days (need 30–50% bone loss)', 'Lucency, periosteal reaction, sequestrum, sclerosis, Codman triangle in acute', 'Initial assessment; follow-up; chronic OM'],
['MRI (GOLD STANDARD)', 'Positive in 3–5 days', 'T1: ↓ signal (marrow replacement); T2/STIR: ↑ signal; enhances with gadolinium; shows extent', 'Best overall; especially for spinal/diabetic foot OM'],
['Technetium-99m bone scan', 'Positive in 24–72 hours', 'Three-phase positive (blood flow, blood pool, delayed)', 'Good sensitivity; poor specificity; false-negative in neonate/early OM; used when MRI not available'],
['Gallium-67 scan', 'Positive', 'Differentiates active infection from healing', 'Combined with Tc99m for better specificity'],
['Indium-111 WBC scan', 'Positive', 'Labels WBCs; more specific for infection', 'Chronic OM; diabetic foot'],
['CT scan', 'Anytime', 'Best for sequestrum identification, cortical destruction, abscess', 'Pre-operative planning; sequestrum localization'],
['Ultrasound', 'Early', 'Subperiosteal abscess, soft tissue collection, periosteal elevation', 'Neonates and children; guides aspiration'],
]
),
HL('IMAGING MNEMONIC: "X-ray first, MRI best, Bone scan early, CT for sequestrum." Plain X-ray: 10–21 days. MRI: 3–5 days. Bone scan: 24–72 hours.', 'E8F4FD'),
P('', false),
H2('D. Kocher Criteria — for distinguishing septic arthritis vs. transient synovitis of hip (Fellowship HIGH YIELD)'),
makeTable(
['Criterion', 'Value suggesting Septic Arthritis'],
[
['1. Fever', '> 38.5°C'],
['2. Non-weight-bearing', 'Complete refusal'],
['3. ESR', '> 40 mm/hr'],
['4. WBC', '> 12,000/mm³'],
['5. CRP (Caird addition)', '> 2.0 mg/dL'],
]
),
P('Probability: 0 criteria = 0.2%; 1 criterion = 3%; 2 criteria = 40%; 3 criteria = 93%; 4 criteria = 99.6%; All 5 = near 100%'),
P('', false),
PB(),
H1('7. MANAGEMENT'),
H2('A. General Principles'),
bullet('START antibiotics only AFTER cultures taken (blood ± bone aspiration)'),
bullet('IV antibiotics initially, then step-down to oral once clinically responding'),
bullet('Duration: 4–6 weeks total (2–4 weeks IV + oral, or early oral if sensitive pathogen)'),
bullet('Monitor response with CRP (should halve by day 3–4; normalize by day 7–10 in acute)'),
P('', false),
H2('B. Antibiotic Selection'),
makeTable(
['Organism / Setting', 'First-Line Antibiotic', 'Alternatives / Notes'],
[
['S. aureus (MSSA)', 'Flucloxacillin (IV) / Cloxacillin', 'Oral step-down: Flucloxacillin, cefalexin'],
['MRSA', 'Vancomycin IV', 'Teicoplanin, linezolid, daptomycin, oritavancin'],
['Gram-negative (Pseudomonas)', 'Ceftazidime / Piperacillin-tazobactam', 'Ciprofloxacin oral (excellent bone penetration)'],
['Salmonella (SCD)', 'Ciprofloxacin / 3rd gen cephalosporin', 'Ampicillin historically'],
['Anaerobes / mixed (diabetic foot)', 'Piperacillin-tazobactam ± metronidazole', 'Clindamycin for MRSA + anaerobes'],
['TB (Pott\'s disease)', '2HRZE / 4HR (WHO protocol)', 'RHEZ × 2 months + RH × 4 months minimum'],
['Empirical (child, unknown)', 'Anti-staphylococcal penicillin ± aminoglycoside', 'Adjust on culture'],
]
),
HL('CIPROFLOXACIN has EXCELLENT bone penetration — one of the few oral agents achieving good bone levels. Useful for gram-negative osteomyelitis and Salmonella.', 'E8F5E9'),
P('', false),
H2('C. Surgical Management'),
makeTable(
['Indication', 'Procedure', 'Key Detail'],
[
['Acute OM with subperiosteal abscess or no response to 48h antibiotics', 'Surgical drainage + decompression (drilling)', 'Drill cortex to decompress medullary pus; specimens for culture'],
['Chronic OM with sequestrum', 'Sequestrectomy', 'Remove dead bone; essential — antibiotics cannot penetrate sequestrum'],
['Dead space after debridement', 'Dead space management', 'Antibiotic beads (PMMA + gentamicin); Masquelet technique; muscle flap'],
['Sinus tract excision', 'Tract excision', 'Complete excision required; biopsy for SCC if long-standing'],
['Infected non-union / implant OM', 'Implant removal + debridement + fixation', 'External fixator (Ilizarov) often; two-stage reconstruction'],
['Diabetic foot OM', 'Debridement ± ray amputation ± BKA', 'Conservative if adequate blood supply; aggressive if not'],
['Instability (Stage IV Cierny-Mader)', 'External fixation (Ilizarov / Taylor Spatial Frame)', 'Maintains stability while infection treated'],
['Bone gap after debridement', 'Bone transport (Ilizarov) / Masquelet technique / bone graft', 'After dead space fully controlled'],
]
),
P('', false),
H2('D. Masquelet Technique (Induced Membrane / 2-Stage)'),
bullet('STAGE 1: Radical debridement + cement spacer (PMMA with antibiotics) placement in defect → forms "induced membrane" in 6–8 weeks'),
bullet('STAGE 2: Remove cement spacer → fill defect with autologous bone graft (protected by induced membrane which secretes growth factors)'),
bullet('Best for large segmental bone defects after chronic OM debridement'),
P('', false),
PB(),
H1('8. SPECIAL TYPES'),
H2('A. Brodie Abscess (Subacute Osteomyelitis)'),
bullet('Walled-off intraosseous abscess; usually distal tibia/proximal tibia metaphysis in children'),
bullet('Organism: S. aureus (low virulence)'),
bullet('X-ray: Lytic lesion with dense sclerotic margin; periosteal reaction; may cross physis'),
bullet('Tongue-like extension toward growth plate on MRI — virtually pathognomonic'),
bullet('Roberts Classification (Type I–VI): Type Ia = punched out metaphyseal lucency; Type Ib = same + sclerotic rim; Type II = metaphyseal with expansion; Type III = diaphyseal; Type IV = layered periosteal; Type V = epiphyseal; Type VI = spinal'),
bullet('Treatment: Curettage + antibiotics; not drainage alone (wall must be broken)'),
P('', false),
H2('B. Sclerosing Osteomyelitis of Garre'),
bullet('Chronic non-suppurative osteomyelitis; no pus, no sinus tract'),
bullet('Dense cortical sclerosis + periosteal thickening on X-ray'),
bullet('Most common in mandible; also tibia'),
bullet('Organism: Actinomyces (mandible), low-virulence S. aureus'),
P('', false),
H2('C. Pott\'s Disease (Spinal TB)'),
bullet('Commonest site: Lower thoracic-upper lumbar junction (T10–L2)'),
bullet('Infection starts at ANTERIOR PART of vertebral body (paradiscal infection)'),
bullet('Spreads to adjacent disc → anterior wedging → kyphosis (Pott\'s kyphosis/gibbus)'),
bullet('Psoas abscess: "cold abscess" tracking along psoas sheath → iliac fossa → lesser trochanter (Petit\'s triangle)'),
bullet('Neurological complications: Pott\'s paraplegia (early = active disease; late = healed disease + scar)'),
bullet('MRI gold standard; X-ray shows: vertebral collapse, disc involvement, paradiscal erosion'),
P('', false),
H2('D. Salmonella Osteomyelitis in Sickle Cell Disease'),
bullet('Sickle cells occlude metaphyseal vessels → bone infarcts → nidus for Salmonella seeding'),
bullet('Loss of splenic function → impaired Salmonella clearance'),
bullet('Often diaphyseal (unlike typical metaphyseal OM)'),
bullet('Multiple sites (polyostotic) possible'),
bullet('Treatment: Ciprofloxacin or 3rd generation cephalosporin'),
P('', false),
PB(),
H1('9. COMPLICATIONS'),
makeTable(
['Complication', 'Notes'],
[
['Chronic osteomyelitis', 'Most common complication of acute OM; 5–25% progress to chronic'],
['Septic arthritis', 'Especially in neonates (metaphysis intracapsular); hip, knee, shoulder at risk'],
['Growth disturbance', 'Physeal damage → leg length discrepancy; angular deformity'],
['Pathologic fracture', 'Through weakened/necrotic bone'],
['Avascular necrosis', 'Periosteal stripping + vascular compromise'],
['Marjolin\'s ulcer (SCC)', 'Squamous cell carcinoma in chronic sinus tract — develops after 20–30 years'],
['Amyloidosis', 'Secondary (reactive) amyloidosis in long-standing chronic OM'],
['Sarcomatous change', 'Rare; fibrosarcoma or other sarcoma in chronically infected bone'],
['Septicaemia', 'Bacteremia from hematogenous spread; especially in immunocompromised'],
['Endocarditis', 'Seeding of heart valves from bacteremia'],
['Non-union', 'In post-fracture osteomyelitis; infection prevents union'],
]
),
HL('EXAM: Chronic sinus tract → Squamous Cell Carcinoma (Marjolin\'s ulcer) developing after 20–30 years. MUST mention in any chronic OM complication question.', 'FFE0E0'),
P('', false),
PB(),
H1('10. RECENT EVIDENCE (2023–2026)'),
makeTable(
['PMID', 'Study', 'Key Finding'],
[
['36421016', 'Zhang et al. J Pediatr Orthop B 2023 — Meta-analysis', 'Procalcitonin (PCT) has high sensitivity AND specificity for osteomyelitis/septic arthritis in children; better than WBC for diagnosing bacterial infections'],
['39722225', 'Edelbach et al. Spine 2025 — Network meta-analysis', 'Optimal antibiotic duration for spondylodiscitis: 6 weeks minimum; oral step-down safe if clinically improving'],
['41224240', 'Krsak et al. Pharmacotherapy 2025 — Meta-analysis', 'Oritavancin (long-acting lipoglycopeptide) effective for MRSA osteomyelitis; once-weekly dosing feasible; good option for outpatient treatment'],
['40982761', 'Sood et al. Adv Skin Wound Care 2025 — Systematic review', 'Oral antibiotics (especially fluoroquinolones + rifampicin combo) effective for diabetic foot osteomyelitis; non-inferior to IV in many cases'],
['38566503', 'Ansert et al. Wound Repair Regen 2024 — Meta-analysis', 'ESR, CRP, and WBC all have limited utility for diagnosing diabetic foot osteomyelitis; MRI remains gold standard'],
]
),
P('', false),
H1('11. CLASSIC LANDMARK ARTICLES'),
makeTable(
['Author / Year', 'Contribution'],
[
['Waldvogel, Medoff & Swartz (1970)', '"Osteomyelitis: a review of clinical features, therapeutic considerations, and unusual aspects" — NEJM. First comprehensive classification by pathogenesis and duration; still most widely used clinically'],
['Cierny & Mader (1985)', 'Cierny-Mader staging system — anatomic type + host physiology; guides surgical treatment decision-making for chronic OM'],
['Lew & Waldvogel (1997, 2004)', 'Lancet review of osteomyelitis — comprehensive update; established modern management principles; antibiotic duration guidelines'],
['Pott (1779)', 'First described vertebral osteomyelitis (Pott\'s disease) — classic description of TB spine, kyphosis, paraplegia'],
['Roberts et al. (1982)', 'Classification of Brodie abscess into Types I–VI based on radiographic appearance'],
['Caird et al. (2006)', 'Addition of CRP to Kocher criteria (5th criterion) — improved prediction of septic arthritis vs. transient synovitis'],
['Kocher et al. (1999)', 'Original Kocher criteria for distinguishing septic arthritis from transient synovitis of hip'],
['Masquelet & Begue (2010)', 'Induced membrane technique (Masquelet) for reconstruction of large bone defects after chronic OM debridement'],
]
),
P('', false),
PB(),
H1('12. QUICK REVISION TABLES'),
H2('Organisms by Special Setting — HIGH-YIELD EXAM TABLE'),
makeTable(
['Setting', 'Organism'],
[
['All cases (#1 overall)', 'S. aureus'],
['Sickle cell disease (CLASSIC EXAM)', 'Salmonella spp.'],
['IV drug user', 'Pseudomonas aeruginosa'],
['Neonates', 'Group B Streptococcus + E. coli'],
['Puncture wound through rubber sole', 'Pseudomonas aeruginosa'],
['Dog/cat bite', 'Pasteurella multocida'],
['Human fight bite', 'Eikenella corrodens'],
['Diabetic foot', 'Polymicrobial (S. aureus + gram-neg + anaerobes)'],
['TB spine (Pott\'s)', 'Mycobacterium tuberculosis'],
['Post-surgery / implant', 'Coagulase-negative Staph (S. epidermidis)'],
]
),
P('', false),
H2('X-ray Changes Timeline'),
makeTable(
['Timeframe', 'X-ray Finding'],
[
['0–10 days', 'Normal X-ray (too early); soft tissue swelling only'],
['10–21 days', 'Lytic area (lucency) in metaphysis; periosteal reaction begins'],
['3–4 weeks', 'Periosteal new bone; cortical destruction; Codman triangle possible'],
['6+ weeks (chronic)', 'Involucrum; sequestrum; sclerosis; Cloaca; sinus tracts'],
['MRI', 'Positive within 3–5 days of onset — preferred for early diagnosis'],
]
),
P('', false),
PB(),
H1('13. MCQ BANK — 10 QUESTIONS'),
H3('(Mixed DNB/MS Final + Fellowship Level)'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q1. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('A 7-year-old boy presents with fever and point tenderness over the distal femoral metaphysis. Blood cultures are negative. The MOST LIKELY causative organism is:'),
bullet('A. Salmonella typhi'), bullet('B. Group B Streptococcus'), bullet('C. Staphylococcus aureus'), bullet('D. Pseudomonas aeruginosa'),
HL('Answer: C. S. aureus accounts for 80–90% of culture-positive pyogenic osteomyelitis across ALL age groups. S. aureus cell wall proteins bind bone matrix collagen, facilitating adherence. Group B Strep is for neonates; Salmonella is for sickle cell disease; Pseudomonas is for IV drug users/puncture wounds.', 'E8F5E9'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q2. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('In a child with sickle cell disease who develops osteomyelitis, which organism is the CLASSIC examination answer for the causative agent?'),
bullet('A. Staphylococcus aureus'), bullet('B. Salmonella species'), bullet('C. Pseudomonas aeruginosa'), bullet('D. Streptococcus pneumoniae'),
HL('Answer: B. Salmonella is the CLASSIC exam answer for osteomyelitis in sickle cell disease. The mechanism: bone infarcts from sickling create a nidus; lost splenic function impairs Salmonella clearance. (Note: S. aureus is actually statistically more common, but Salmonella is the high-yield exam answer.)', 'E8F4FD'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q3. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('Why does hematogenous osteomyelitis preferentially affect the METAPHYSIS of long bones in children?'),
bullet('A. Metaphysis has the highest blood flow velocity'), bullet('B. Metaphysis lacks periosteum'), bullet('C. Slow blood flow in looped sinusoidal vessels + microtrauma facilitates bacterial seeding'), bullet('D. Metaphyseal bone is less mineralized'),
HL('Answer: C. Metaphyseal sinusoidal vessels loop and slow blood flow markedly (almost stagnant). This, combined with microtrauma, allows bacteria to settle and multiply. The vessels also lack phagocytic lining cells (unlike the arterioles).', 'FFF9C4'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q4. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('In a 30-year-old with chronic osteomyelitis of the tibia, X-ray shows a dense shell of new bone surrounding a fragment of necrotic bone, with a small hole in the new bone shell. The correct anatomical terms are (outer shell → inner dead bone → hole in shell):'),
bullet('A. Involucrum → Cloaca → Sequestrum'), bullet('B. Sequestrum → Involucrum → Cloaca'), bullet('C. Involucrum → Sequestrum → Cloaca'), bullet('D. Cloaca → Sequestrum → Involucrum'),
HL('Answer: C. INVOLUCRUM (outer reactive new periosteal bone shell) surrounds the SEQUESTRUM (inner dead avascular bone). The CLOACA is the opening/hole in the involucrum through which pus and fragments may discharge. The sinus tract is the track from the cloaca to the skin surface.', 'E8F4FD'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q5. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('In Cierny-Mader classification, a patient with osteomyelitis of the tibia where the infection involves the entire bone circumference and removal of infected bone would render the limb unstable is classified as:'),
bullet('A. Stage I — Medullary'), bullet('B. Stage II — Superficial'), bullet('C. Stage III — Localized'), bullet('D. Stage IV — Diffuse'),
HL('Answer: D. Stage IV = Diffuse osteomyelitis — full-thickness circumferential involvement where debridement of all infected bone would result in mechanical instability. This is the most severe stage and requires stabilization (Ilizarov/external fixation) during treatment.', 'E8F5E9'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q6. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('The earliest imaging modality to demonstrate osteomyelitis (positive within 24–72 hours of onset) is:'),
bullet('A. Plain X-ray'), bullet('B. CT scan'), bullet('C. Technetium-99m 3-phase bone scan'), bullet('D. Ultrasound'),
HL('Answer: C. Tc-99m three-phase bone scan becomes positive within 24–72 hours. Plain X-ray takes 10–21 days. MRI is positive in 3–5 days (and is the GOLD STANDARD overall). Ultrasound can detect subperiosteal abscess early but doesn\'t show bone changes.', 'FFF9C4'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q7. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('A 45-year-old diabetic presents with a plantar foot ulcer and can feel hard bone at the base of the wound on probing with a metal probe. The "probe-to-bone" test is positive. This finding suggests:'),
bullet('A. Tendon exposure only'), bullet('B. Diabetic neuropathy'), bullet('C. Osteomyelitis (positive predictive value ~90%)'), bullet('D. Charcot arthropathy'),
HL('Answer: C. The "probe-to-bone" test: a positive result (hard, gritty bone felt with metal probe through an ulcer) has approximately 90% positive predictive value for underlying osteomyelitis in the diabetic foot. It is a simple, cheap bedside test that should prompt MRI confirmation.', 'E8F4FD'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q8. (DNB Level)', bold: true, color: '1F4E79' })], spacing: { before: 120 } }),
P('A 12-year-old presents with 6 weeks of localized tibial pain. X-ray shows a lytic metaphyseal lesion with a dense sclerotic rim and periosteal reaction. No fever. The MOST LIKELY diagnosis is:'),
bullet('A. Ewing sarcoma'), bullet('B. Brodie abscess (subacute osteomyelitis)'), bullet('C. Osteoid osteoma'), bullet('D. Osteosarcoma'),
HL('Answer: B. Brodie abscess is a walled-off subacute osteomyelitis — lytic metaphyseal lesion with sclerotic rim + periosteal reaction in a child/adolescent with subacute bone pain and NO systemic sepsis. It MIMICS tumour. RULE: Always send tissue for culture at any bone biopsy to rule out infection. MRI shows tongue-like extension toward physis.', 'E8F5E9'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q9. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('In Pott\'s disease, which part of the vertebra is FIRST affected?'),
bullet('A. Posterior neural arch'), bullet('B. Pedicle'), bullet('C. Anterior vertebral body (paradiscal, subchondral)'), bullet('D. Spinous process'),
HL('Answer: C. TB spine (Pott\'s disease) characteristically begins in the ANTERIOR part of the vertebral body (paradiscal, subchondral region). It spreads to the adjacent disc (disc avascular — resistance lower) and then to adjacent vertebra. Posterior elements are spared early. This gives the typical anterior wedging/gibbus deformity. Disc involvement distinguishes TB from mets (mets spare disc).', 'FFF9C4'),
P('', false),
new Paragraph({ children: [new TextRun({ text: 'Q10. (Fellowship Level)', bold: true, color: '7B1FA2' })], spacing: { before: 120 } }),
P('A 50-year-old patient with chronic discharging sinus of the lower leg for 25 years develops a raised, indurated, everted edge around the sinus. The biopsy shows squamous cell carcinoma. This is:'),
bullet('A. Garre\'s sclerosing osteomyelitis'), bullet('B. Primary bone sarcoma'), bullet('C. Marjolin\'s ulcer (SCC in chronic sinus tract of osteomyelitis)'), bullet('D. Basal cell carcinoma'),
HL('Answer: C. Marjolin\'s ulcer — squamous cell carcinoma developing in a chronic sinus tract of long-standing osteomyelitis (typically after 20–30 years). Key features: everted indurated edge, bleeding, fungating growth at sinus tract. HIGH GRADE malignancy. Treatment: wide excision, often amputation. Metastasizes to regional lymph nodes. ALWAYS warn in chronic OM that this complication can occur.', 'FFE0E0'),
P('', false),
divider(),
new Paragraph({ children: [new TextRun({ text: "END OF OSTEOMYELITIS NOTES | Prepared July 2026 | Sources: Campbell's 15e, Robbins & Kumar Pathology, Bailey & Love 28e, PubMed 2023–2026", color: '7F7F7F', size: 18 })], alignment: AlignmentType.CENTER }),
]}]
});
Packer.toBuffer(doc).then(buf => {
fs.writeFileSync('/home/daytona/workspace/ddh-notes/Osteomyelitis_Ortho_PG_Notes.docx', buf);
console.log('Osteomyelitis DOCX done');
});
A comprehensive medical visual mind map poster for Osteomyelitis for orthopaedic postgraduate exam revision. Central node "OSTEOMYELITIS" with clearly labeled color-coded branches: 1) CLASSIFICATION branch showing Waldvogel (Hematogenous, Contiguous without/with vascular insufficiency, Acute/Subacute/Chronic) and Cierny-Mader (Stage I Medullary, II Superficial, III Localized, IV Diffuse + Host A Normal, B Compromised, C Treatment worse than disease). 2) PATHOLOGY SEQUENCE flowchart: Bacteremia → Metaphyseal seeding (slow sinusoidal flow) → Neutrophil infiltrate → Bone necrosis 48hrs → Pus under pressure → Periosteal elevation → Cortical AVN → SEQUESTRUM (dead bone) → INVOLUCRUM (new periosteal bone) → CLOACA (hole in involucrum) → SINUS TRACT. Include labeled anatomical cross-section diagram of bone showing sequestrum inside involucrum with cloaca. 3) ORGANISMS by setting: S. aureus all cases, Salmonella sickle cell, Pseudomonas IV drugs and puncture wound, Group B Strep neonates, Polymicrobial diabetic foot, TB spine (Pott's). 4) INVESTIGATIONS: X-ray (10-21 days), MRI Gold Standard (3-5 days), Bone scan (24-72 hours), CT for sequestrum. Kocher criteria table. 5) TREATMENT: IV antibiotics 4-6 weeks, Sequestrectomy for chronic, Masquelet technique for defects, Ilizarov for instability. 6) COMPLICATIONS: Chronic OM, Septic arthritis, Marjolin ulcer (SCC in sinus), Pathologic fracture, Amyloidosis. 7) SPECIAL TYPES: Brodie abscess (subacute, sclerotic rim, metaphysis), Pott's disease (anterior vertebral body, disc involvement, psoas abscess, paraplegia), Garre's sclerosing. Professional medical infographic, color-coded sections, white background, anatomical diagrams, exam-focused key points highlighted.
cd /home/daytona/workspace/ddh-notes && node create_osteo_notes.js 2>&1 && ls -l…
OSTEOMYELITIS
Complete PG Orthopaedics Notes | DNB / MS Final + Fellowship Level
📥 Download
Osteomyelitis Ortho PG Notes
Word Document · DOCX
🗺️ Visual Mind Map Poster
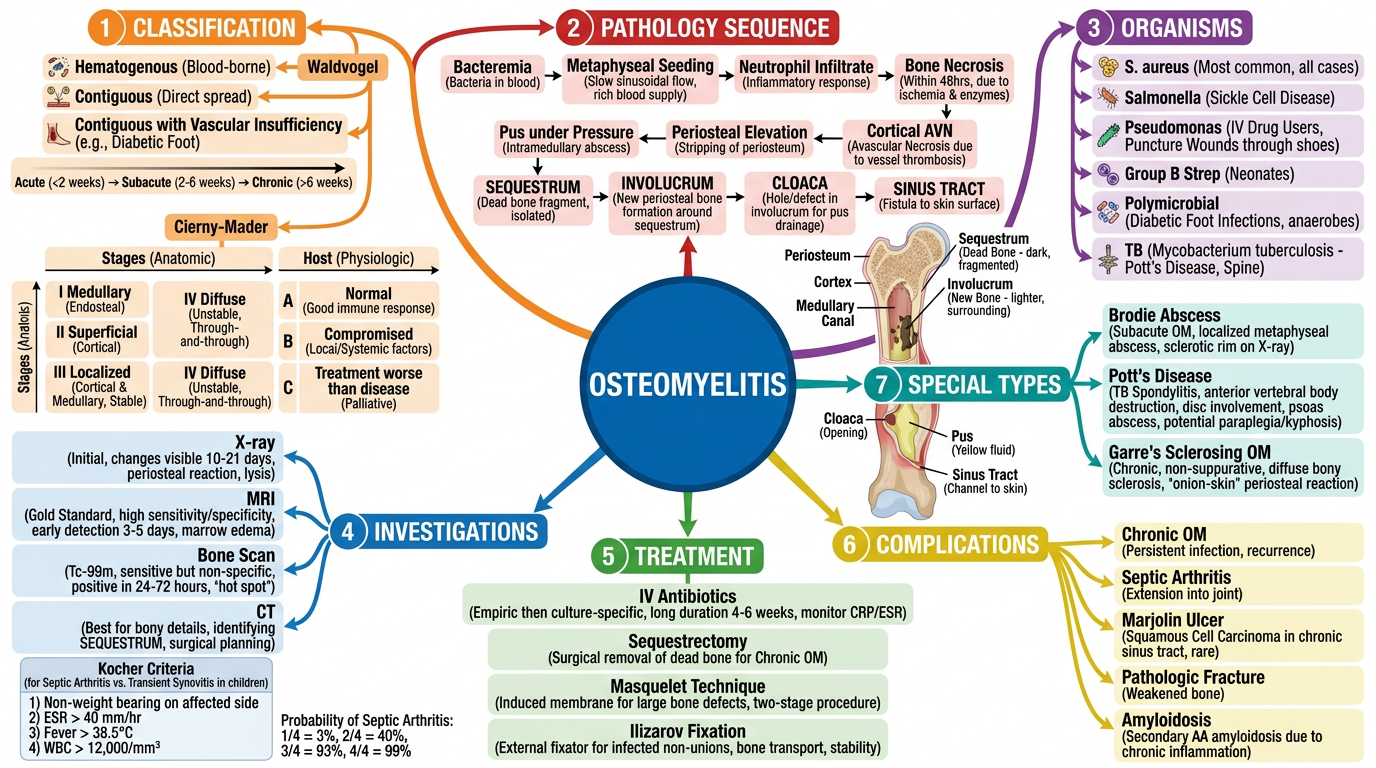
1. DEFINITION
- Hematogenous spread (blood-borne; most common in children)
- Contiguous focus (spread from adjacent soft tissue; post-trauma/surgery; adults)
- Direct inoculation (open fracture, surgical procedures)
S. aureus causes 80–90% of culture-positive pyogenic osteomyelitis — its cell wall proteins bind to bone matrix collagen, facilitating adherence.
2. CLASSIFICATION
A. Waldvogel Classification (1970) — Clinically most widely used
| Category | Type | Key Features |
|---|---|---|
| By Pathogenesis | Hematogenous | Children, single organism, metaphyseal, bacteremia |
| Contiguous (no vascular insufficiency) | Post-trauma/surgery, mixed organisms, adults | |
| Contiguous (with vascular insufficiency) | Diabetic foot, PVD, polymicrobial, poor healing | |
| By Duration | Acute | <2 weeks; no sequestrum |
| Subacute | 2 weeks – 3 months; Brodie abscess | |
| Chronic | >3 months; sequestrum + involucrum present |
B. Cierny-Mader Classification (1985) — Best for SURGICAL PLANNING of chronic OM
| Stage | Type | Bone Involvement |
|---|---|---|
| I — Medullary | Infection in medullary canal only | Hematogenous OM; infected IM nail |
| II — Superficial | Cortical surface only | Post-radiation; contiguous spread |
| III — Localized | Full-thickness cortex + medullary; STABLE (debridement won't destabilize) | Localized chronic OM |
| IV — Diffuse | Entire bone circumference; UNSTABLE if bone removed | Infected nonunion; diffuse chronic OM |
| Host | Description |
|---|---|
| A | Normal host; standard treatment |
| Bs | Systemic compromise: DM, malnutrition, immunosuppression, CRF, HIV |
| Bl | Local compromise: vascular disease, scarring, radiation, neuropathy, tobacco |
| Bls | Both systemic + local compromise |
| C | Treatment worse than disease → suppressive therapy only, no curative surgery |
Treatment rule: Stage I & II = antibiotics ± limited surgery. Stage III & IV = aggressive debridement + 4–6 weeks antibiotics. Class C = suppress, don't cure.
3. PATHOPHYSIOLOGY — SEQUENCE OF EVENTS
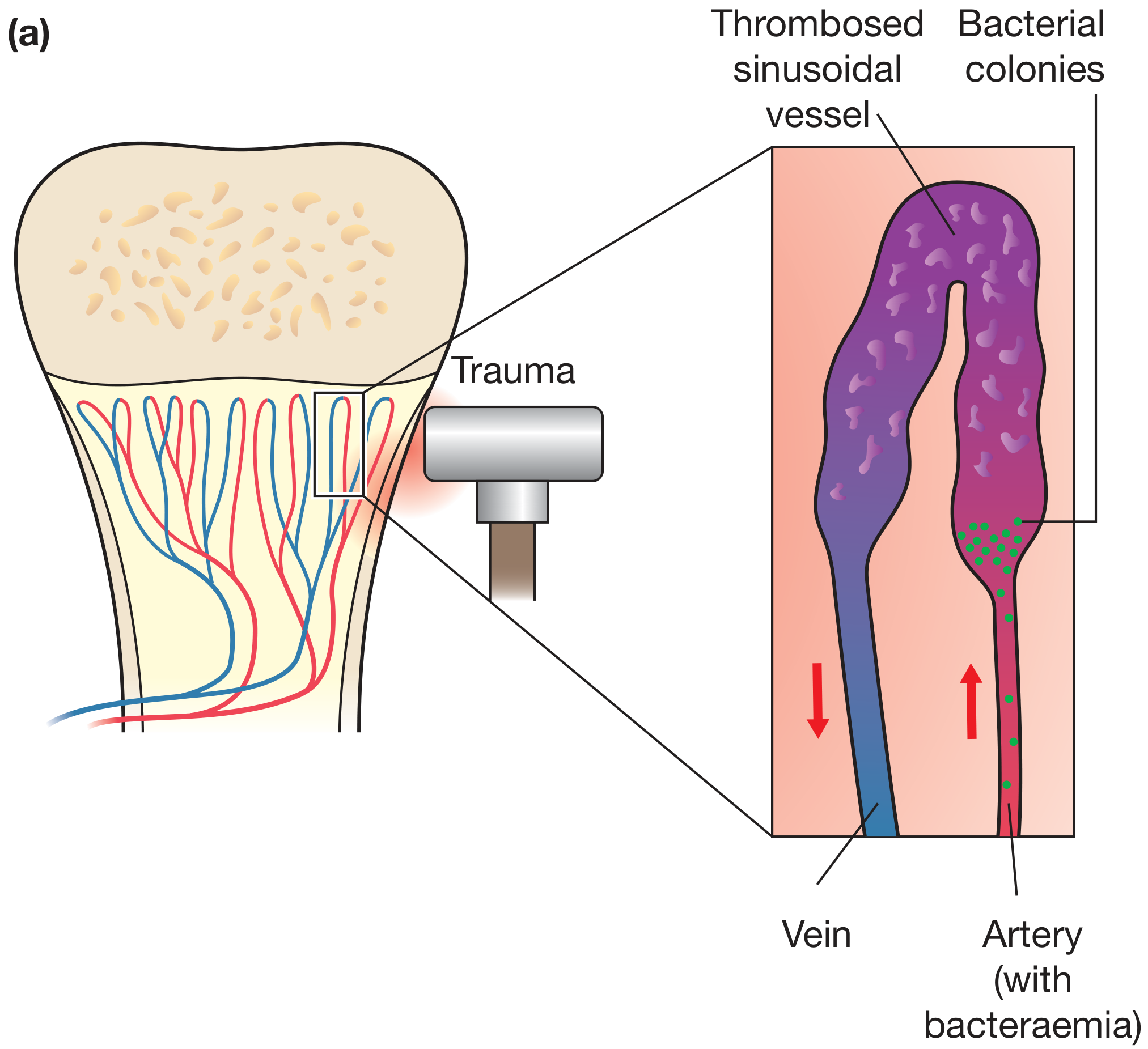
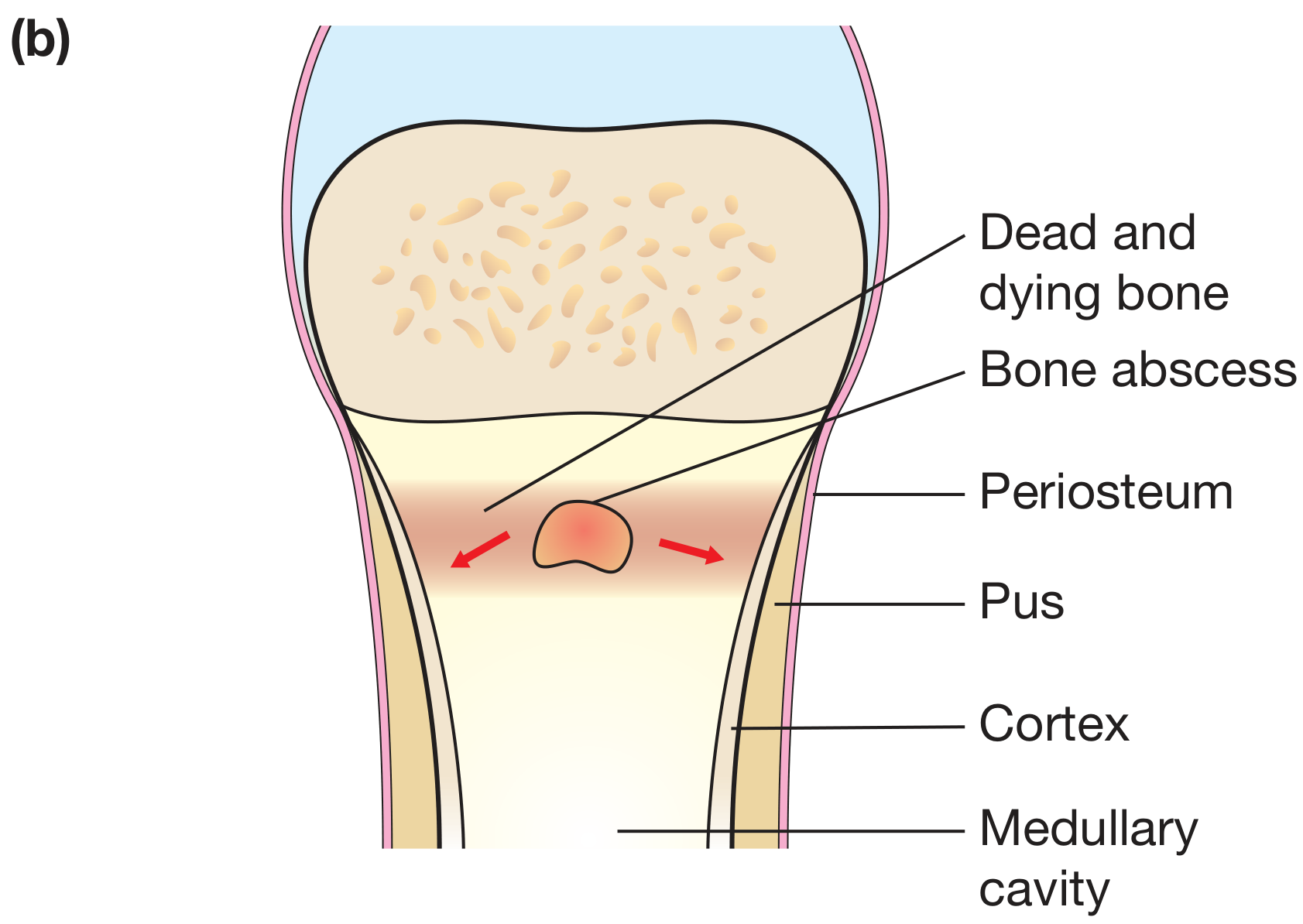
BACTEREMIA
↓
Bacteria seed METAPHYSEAL sinusoidal vessels
(slow looped flow + microtrauma → lodgment)
↓
Bacterial multiplication → Neutrophilic reaction
↓
BONE NECROSIS within 48 hours
↓
Pus forms → HIGH PRESSURE in medullary canal
↓
Pus tracks through Haversian canals → SUBPERIOSTEAL ABSCESS
↓
Periosteal ELEVATION → cortex loses blood supply
↓
SEQUESTRUM = dead avascular cortical bone
↓
Periosteum reacts → new bone forms
↓
INVOLUCRUM = reactive shell of new living bone around sequestrum
↓
Hole in involucrum = CLOACA
↓
Track to skin = SINUS TRACT
KEY TERMS — HIGH YIELD
| Term | Definition |
|---|---|
| Sequestrum | Dead, devascularized necrotic cortical bone — NO antibiotic penetration (avascular) |
| Involucrum | Reactive new periosteal bone shell forming around the sequestrum |
| Cloaca | Opening / hole in the involucrum — through which pus and bone fragments drain |
| Sinus tract | Track from cloaca to skin surface; lined by granulation tissue |
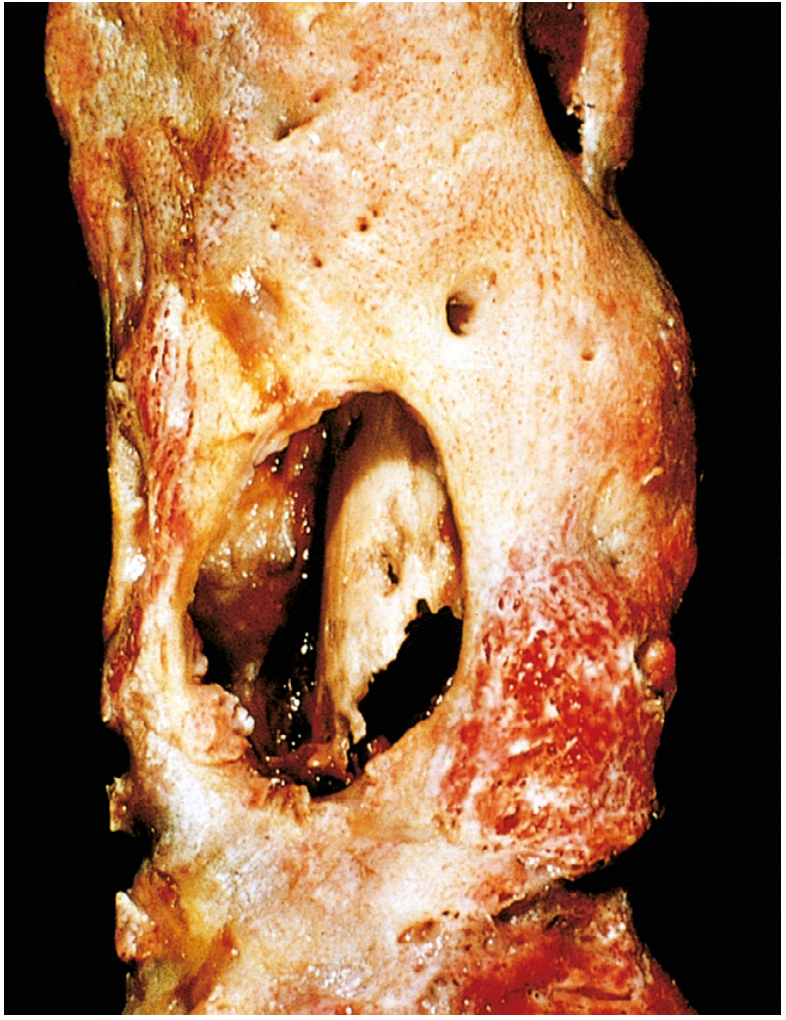
4. MICROBIOLOGY — HIGH-YIELD TABLE
| Clinical Setting | Organism | Exam Note |
|---|---|---|
| Any/all cases (#1) | S. aureus | 80–90% of all culture-positive OM |
| Sickle cell disease | Salmonella spp. | CLASSIC exam answer; bone infarcts + asplenia |
| IV drug user | Pseudomonas aeruginosa | Vertebral, sternoclavicular, pubic symphysis |
| Neonates | Group B Streptococcus + E. coli | Multiple sites; joint involvement common |
| Puncture wound (rubber sole) | Pseudomonas aeruginosa | Classic: nail through sneaker |
| Dog/cat bite | Pasteurella multocida | Rapidly progressive |
| Human fight bite | Eikenella corrodens + oral flora | Metacarpal head; very destructive |
| Diabetic foot | Polymicrobial | S. aureus + Strep + gram-neg + anaerobes |
| TB spine (Pott's) | M. tuberculosis | Anterior vertebral body; disc involved |
| Post-surgery / implant | S. epidermidis (CoNS) | Biofilm; slow onset |
EXAM TRAP: Salmonella for sickle cell is the most tested association in osteomyelitis MCQs worldwide.
5. CLINICAL FEATURES
Age-based differences:
| Age | Site | Presentation | Septic Arthritis Risk |
|---|---|---|---|
| Neonate (0–1 mo) | Metaphysis + epiphysis (vessels cross physis) | Pseudoparalysis; minimal systemic signs; insidious | HIGH — hip, shoulder, knee commonly involved |
| Child (1–16 yr) | Metaphysis only (vessels don't cross physis) | Fever + pain + local tenderness + limp | Lower (depends on intracapsular metaphysis) |
| Adult | Epiphysis + subchondral (anastomoses form after physis closes) | Variable; often contiguous/post-surgical | Variable |
Chronic Osteomyelitis Signs:
- Thickened, sclerotic bone on palpation
- Discharging sinus with watery/purulent discharge
- "Quiet intervals" between flares
- Limb deformity, shortening
- Marjolin's ulcer — raised, everted, indurated edge around sinus = SCC warning
6. INVESTIGATIONS
Imaging Timeline:
| Modality | Positive At | Key Findings | Use |
|---|---|---|---|
| Plain X-ray | 10–21 days (need 30–50% bone loss) | Lucency, periosteal reaction, sequestrum | First-line; follow-up |
| MRI (GOLD STANDARD) | 3–5 days | T1↓ / T2↑ / STIR↑ in marrow; gadolinium enhances | Best overall; spinal OM; diabetic foot |
| Tc-99m Bone Scan | 24–72 hours | Three-phase positive | Early diagnosis; polyostotic disease |
| CT scan | Anytime | Best for sequestrum, cortical detail | Pre-op planning |
| Ultrasound | Early | Subperiosteal abscess | Neonates; guides aspiration |
MRI is the gold standard for diagnosis but bone scan is the EARLIEST positive test (24–72 hrs)
Kocher Criteria (Septic arthritis vs. Transient Synovitis of Hip):
| Criterion | Cut-off | Points |
|---|---|---|
| Fever | > 38.5°C | 1 |
| Non-weight-bearing | Complete refusal | 1 |
| ESR | > 40 mm/hr | 1 |
| WBC | > 12,000/mm³ | 1 |
| CRP (Caird 5th criterion) | > 2.0 mg/dL | 1 |
7. MANAGEMENT
Antibiotic Selection:
| Organism | First-Line | Oral Step-Down |
|---|---|---|
| MSSA | Flucloxacillin IV | Flucloxacillin, cefalexin |
| MRSA | Vancomycin IV | Linezolid, teicoplanin, daptomycin, oritavancin (new) |
| Pseudomonas | Ceftazidime / pip-tazo | Ciprofloxacin (excellent bone penetration) |
| Salmonella | Ciprofloxacin / 3rd gen ceph | Ciprofloxacin oral |
| Anaerobes | Piperacillin-tazo + metronidazole | Clindamycin |
| TB (Pott's) | 2HRZE / 4HR | WHO regimen; 6 months minimum |
Ciprofloxacin has excellent bone penetration — one of few oral agents achieving therapeutic bone concentrations.
Surgical Indications & Procedures:
| Indication | Procedure |
|---|---|
| Subperiosteal abscess / no response to 48h antibiotics | Surgical drainage + cortical drilling/decompression |
| Sequestrum present (chronic OM) | Sequestrectomy — MANDATORY (antibiotics cannot reach avascular dead bone) |
| Dead space after debridement | Antibiotic beads (PMMA + gentamicin); Masquelet technique |
| Large bone defect | Masquelet (induced membrane) + bone graft OR bone transport (Ilizarov) |
| Instability (Cierny-Mader Stage IV) | Ilizarov external fixator / Taylor Spatial Frame |
| Infected non-union | Implant removal + debridement + external fixation |
| Diabetic foot OM | Debridement ± ray amputation ± BKA |
Masquelet Technique (2-Stage for Bone Defects):
- Stage 1: Radical debridement + antibiotic cement spacer → forms "induced membrane" in 6–8 weeks
- Stage 2: Remove spacer → fill defect with autologous bone graft (membrane secretes growth factors to aid graft incorporation)
8. SPECIAL TYPES
Brodie Abscess (Subacute OM)
- Walled-off intraosseous abscess; distal tibia metaphysis most common
- S. aureus (low virulence); insidious onset; no systemic sepsis
- X-ray: Lytic lesion + dense sclerotic rim + periosteal reaction
- MRI: "Tongue-like" extension toward physis — pathognomonic
- Mimics tumor → ALWAYS send tissue for culture + histology
- Treatment: Curettage + antibiotics
Pott's Disease (Spinal TB)
- Site: T10–L2 (lower thoracic/upper lumbar) most common
- Starts: ANTERIOR part of vertebral body (paradiscal) → spreads to disc → adjacent vertebra
- Key difference from mets: Disc INVOLVED (TB) vs. disc SPARED (mets)
- Psoas abscess: "Cold abscess" tracking along psoas sheath to iliac fossa
- Complications: Pott's kyphosis (gibbus); Pott's paraplegia (early = active disease; late = healed scar)
- Imaging: MRI gold standard; X-ray: anterior wedging, disc space loss
Garre's Sclerosing Osteomyelitis
- Chronic non-suppurative; no pus, no sinus; dense sclerosis + periosteal thickening
- Most common: mandible; also tibia
9. COMPLICATIONS
| Complication | Key Points |
|---|---|
| Chronic osteomyelitis | 5–25% of acute OM; sequestrum forms |
| Septic arthritis | Especially neonates; hip/shoulder/knee |
| Growth disturbance | Physeal damage → LLD, angular deformity |
| Pathologic fracture | Through weakened bone |
| Marjolin's ulcer (SCC) | Squamous cell carcinoma in chronic sinus tract after 20–30 years |
| Secondary amyloidosis | Long-standing chronic OM |
| Endocarditis | From bacteremia |
| Non-union | In post-fracture OM |
Marjolin's ulcer: Raised, indurated, everted edge at chronic sinus tract → biopsy → SCC. Wide excision / amputation needed. Always warn about this in long-standing chronic OM.
10. RECENT EVIDENCE (2023–2026)
| PMID | Study | Key Finding |
|---|---|---|
| 36421016 | Zhang et al. 2023 — Meta-analysis | Procalcitonin: high Se+Sp for OM/septic arthritis in children |
| 39722225 | Edelbach et al. Spine 2025 | 6 weeks antibiotics optimal for spondylodiscitis; oral step-down safe |
| 41224240 | Krsak et al. 2025 | Oritavancin (once-weekly) effective for MRSA osteomyelitis outpatient treatment |
| 40982761 | Sood et al. 2025 | Oral antibiotics (fluoroquinolone + rifampicin) effective for diabetic foot OM |
| 38566503 | Ansert et al. 2024 | ESR/CRP/WBC limited for diabetic foot OM diagnosis; MRI remains gold standard |
11. CLASSIC LANDMARK ARTICLES
| Author / Year | Contribution |
|---|---|
| Waldvogel, Medoff & Swartz (1970) | NEJM — first comprehensive classification; pathogenesis + duration basis; most widely used clinically |
| Cierny & Mader (1985) | Staging system for chronic OM — anatomic type + host physiology; surgical planning guide |
| Lew & Waldvogel (1997, 2004) | Lancet reviews — modern management principles; antibiotic duration; benchmarks |
| Pott (1779) | First description of spinal TB, kyphosis, paraplegia |
| Roberts et al. (1982) | Brodie abscess classification Types I–VI |
| Kocher et al. (1999) | Criteria for septic arthritis vs. transient synovitis |
| Caird et al. (2006) | Added CRP as 5th Kocher criterion |
| Masquelet & Begue (2010) | Induced membrane technique for large bone defects |
12. KEY MNEMONICS
| Mnemonic | For |
|---|---|
| "Slow vessels + microtrauma = seeding" | Why metaphysis is affected |
| SIS = Sequestrum Inside Shell (Involucrum) | Chronic OM structure |
| "Salmonella in Sickle cell" | CLASSIC exam answer |
| "Probe to bone = OM" | Diabetic foot |
| "X-ray 10 days, MRI 3 days, Scan 1 day" | Imaging timeline |
| "C host = No cure" | Cierny-Mader Class C → suppressive only |
| "Brodie = Benign abscess" | Subacute; sclerotic rim; mimics tumour |
| "Marjolin = Malignant complication" | SCC in chronic sinus after 20–30 years |