Femoral triangle - importance in orthopaedics
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
I now have comprehensive content from multiple authoritative orthopaedic and anatomy textbooks. Let me compile the full answer.
Femoral Triangle - Importance in Orthopaedics

Fig. 1 - Femoral triangle boundaries showing continuity with the adductor canal (Gray's Anatomy for Students)
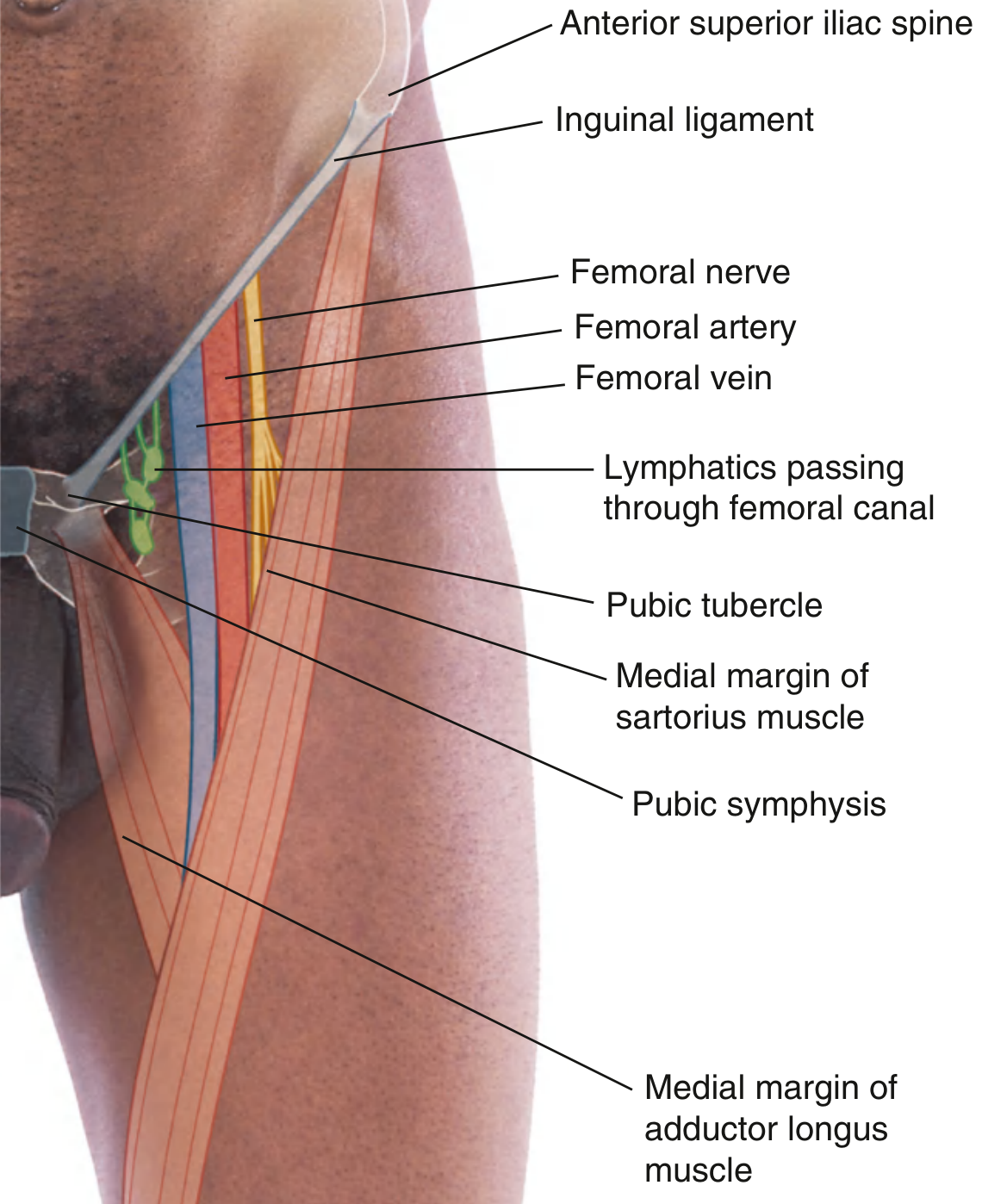
Fig. 2 - Position of the femoral artery and contents in the femoral triangle (Gray's Anatomy for Students)
1. Basic Anatomy
The femoral triangle is a wedge-shaped depression in the proximal anterior thigh at the junction between the anterior abdominal wall and the lower limb.
Borders:
| Boundary | Structure |
|---|---|
| Superior (base) | Inguinal ligament |
| Lateral | Medial margin of sartorius |
| Medial | Medial margin of adductor longus |
Floor (lateral to medial): Iliopsoas, pectineus, adductor longus
Roof: Fascia lata (cribriform fascia over the saphenous opening)
Contents (lateral to medial) - mnemonic "NAVeL":
- Nerve - femoral nerve
- Artery - femoral artery
- Vein - femoral vein
- (empty space)
- Lymphatics (in femoral canal)
The femoral nerve lies outside the femoral sheath (lateral), while the artery, vein, and lymphatics are enclosed within it. - Miller's Review of Orthopaedics, 9th Ed.
Apex: Points inferiorly and is continuous with the adductor (Hunter's) canal, which carries the superficial femoral artery and vein down to the popliteal fossa via the adductor hiatus in adductor magnus. - Gray's Anatomy for Students
2. Orthopaedic Significance
A. Surface Landmark for Femoral Pulse and Vascular Access
The femoral artery can be palpated just inferior to the inguinal ligament, midway between the anterior superior iliac spine (ASIS) and the pubic symphysis (the "mid-inguinal point"). This is the standard site for:
- Femoral arterial line placement
- Intra-aortic balloon pump insertion
- Pre-operative vascular assessment in polytrauma and hip/pelvis fractures
Gray's Anatomy for Students emphasizes that the femoral canal, containing lymphatics, lies immediately lateral to the pubic tubercle - a point critical to avoid puncturing the vein when cannulating the artery.
B. Total Hip Arthroplasty (THA) - Retractor Placement
This is one of the most examined orthopaedic correlations:
"In total hip arthroplasty, retractors placed more inferiorly and medially along the acetabulum place the femoral nerve (and external iliac artery) at risk for injury." - Miller's Review of Orthopaedics, 9th Ed.
"Care should be taken when using a retractor over the anterior acetabular wall because it occludes the femoral vein." - Campbell's Operative Orthopaedics, 15th Ed.
Acetabular screws placed in the anterosuperior quadrant can injure the external iliac artery as it transitions to the femoral artery just under the inguinal ligament. - Miller's Review of Orthopaedics
C. Anterior Approach (Direct Anterior Approach / Smith-Petersen) to the Hip
The anterior/direct anterior approach to the hip proceeds just lateral to the femoral triangle. Key hazards:
- Lateral femoral cutaneous nerve (LFCN) of the thigh, which enters the thigh near the ASIS just lateral to the sartorius - prone to injury, causing meralgia paresthetica
- Ascending branch of the lateral femoral circumflex artery (LFCA), which travels deep to the sartorius and rectus femoris - at risk during anterolateral approaches
- Superior gluteal nerve can be damaged when ligating the ascending branch of the LFCA where it enters tensor fascia latae
Campbell's Operative Orthopaedics notes that anterior approaches offer the shortest distance to the femoral head center but carry significant risk to the LFCN leading to patient dissatisfaction.
D. Femoral Nerve Block (FNB) and Adductor Canal Block (ACB)
The femoral triangle is the target zone for femoral nerve block, a cornerstone of peri-operative analgesia in lower-limb orthopaedic surgery.
Indications (from Morgan & Mikhail's Clinical Anesthesiology):
| Procedure | Preferred Block |
|---|---|
| Hip arthroplasty / fracture / ORIF | Suprainguinal fascia iliaca OR femoral nerve block |
| Total knee arthroplasty (TKA) | Adductor canal block (ACB) preferred over FNB |
| Knee arthroscopy | Adductor canal block |
| Patellar ORIF / tendon repair | Femoral block (with knee immobilizer) |
| ACL reconstruction | ACB (equivalent analgesia, better quadriceps strength) |
The adductor canal block is performed just distal to the femoral triangle apex, targeting the saphenous nerve and nerve to vastus medialis inside the adductor canal. Compared to FNB, it:
- Provides non-inferior analgesia for TKA
- Preserves quadriceps strength, enabling earlier mobilization
- Is now preferred over FNB for TKA in most protocols - Miller's Anesthesia, 10th Ed.
E. Femoral Nerve - Orthopaedic Injury Points
The femoral nerve lies between the iliacus and psoas muscles before entering the femoral triangle. An iliacus hematoma (e.g., in pelvic fractures, anticoagulated patients) can compress the femoral nerve causing:
- Weakness of knee extension (quadriceps palsy)
- Loss of patellar reflex
- Sensory loss over anterior thigh and medial leg
The saphenous nerve (L3, L4) branches off the femoral nerve at the apex of the femoral triangle and travels under sartorius. It becomes subcutaneous on the medial aspect of the knee (between sartorius and gracilis) and travels with the greater saphenous vein. It is:
- At risk during medial meniscus repair and hamstring graft harvest
- The infrapatellar branch can be damaged during TKA or patellar tendon harvest
- Terminal branch supplies sensation to the medial ankle and foot - Miller's Review of Orthopaedics, 9th Ed.
F. Femoral Artery Injury in Orthopaedic Trauma
- The superficial femoral artery (SFA) is the most commonly injured vessel with trauma to the hip and thigh
- Femoral shaft fractures and supracondylar femur fractures may injure the SFA (which travels in the adductor canal) or popliteal artery - require urgent vascular assessment
- Pseudoaneurysm of the femoral artery is a recognized complication of femoral arterial access used during pre-operative angiography or endovascular procedures around the hip and pelvis
- The profunda femoris (deep femoral artery) supplies the musculature of the thigh; its perforating branches are frequently encountered and ligated during femoral shaft surgery
G. Femoral Hernia - Differential in Groin Swelling
The femoral canal (most medial compartment of the femoral sheath) is a potential weak point at the femoral ring. Femoral hernias protrude here and present as groin swellings inferior and lateral to the pubic tubercle (vs. inguinal hernias which are superior and medial). The orthopaedic surgeon must be aware of this in the differential diagnosis of groin pain and masses encountered during hip surgery or examination.
3. Quick Summary Table
| Topic | Orthopaedic Relevance |
|---|---|
| Femoral pulse landmark | Vascular assessment, arterial access |
| Retractor in THA | Risk to femoral nerve/vein; anterior acetabular wall occludes femoral vein |
| Acetabular screws (anterosuperior quadrant) | External iliac/femoral artery injury |
| Direct anterior hip approach | LFCN at risk (meralgia paresthetica) |
| Femoral nerve block | Analgesia for hip fracture, THA |
| Adductor canal block | Preferred for TKA - spares quadriceps |
| Saphenous nerve at apex | At risk in meniscal repair, hamstring harvest, TKA |
| Iliacus hematoma | Femoral nerve palsy (quadriceps weakness) |
| Femoral artery SFA | Injured in femoral shaft / supracondylar fractures |
| Femoral canal | Site of femoral hernia - groin differential |
Sources:
- Miller's Review of Orthopaedics, 9th Ed. - Arthrology and neurovascular anatomy
- Campbell's Operative Orthopaedics, 15th Ed. (2026) - Hip approaches and surgical considerations
- Gray's Anatomy for Students - Femoral triangle anatomy and surface landmarks
- Fischer's Mastery of Surgery, 8th Ed. - Vascular anatomy of the femoral triangle
- Morgan & Mikhail's Clinical Anesthesiology, 7th Ed. and Miller's Anesthesia, 10th Ed. - Regional blocks
This is a shared conversation. Sign in to Orris to start your own chat.