Give me easy way to learn obstetrics topics for a mbbs student and explain everything. I might forget some topics because of my medicine exam i didn't study from a long time.
Reading File
Finding Sources
Searching the Web
MBBS obstetrics important topics exam guide 2025
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have solid textbook content. Here is your complete, easy-to-revise MBBS Obstetrics guide — organized by high-yield topic with clear explanations, mnemonics, and key numbers.
🤰 MBBS Obstetrics — Complete Revision Guide
Everything you need to revise, organized logically. High-yield topics first. Read actively — test yourself after each section.
How to Use This Guide
- Read one section at a time — don't try to do everything in one day
- Write the key numbers/criteria from memory after each topic
- Focus on the bold-text and tables — that's what examiners ask
- Use the mnemonics at the end of each section
🗂️ MASTER TOPIC LIST (MBBS Obstetrics)
| Priority | Topic |
|---|---|
| ⭐⭐⭐ High | Normal Labor & Stages, Preeclampsia/Eclampsia, APH, PPH |
| ⭐⭐⭐ High | Gestational Diabetes, Preterm Labor, PROM |
| ⭐⭐ Medium | Malpresentations, Cord Prolapse, Instrumental Delivery |
| ⭐⭐ Medium | Antenatal Care, Normal Puerperium |
| ⭐ Background | Physiology of Pregnancy, Placenta, Amniotic Fluid |
TOPIC 1: NORMAL LABOR & STAGES 🏆 [Most asked topic]
Definition of Labor
Labor = regular uterine contractions of sufficient frequency, intensity, and duration to cause cervical effacement and dilation.
- Contractions in active labor: every 2–3 minutes, lasting ~1 minute, intensity ~40 mmHg
- Bloody show: blood-tinged mucus discharge → most women go into labor within 3 days
The 4 Stages of Labor
| Stage | Onset → End | Nullipara | Multipara |
|---|---|---|---|
| 1st Stage | Active labor → Full dilation (10 cm) | Up to 20 hrs (latent) | Up to 14 hrs (latent) |
| 2nd Stage | Full dilation → Delivery of baby | ≤2 hrs | ≤1 hr |
| 3rd Stage | Baby delivery → Placenta delivery | ≤30 min | ≤30 min |
| 4th Stage | Placenta delivery → Uterus contracts | 1 hr | 1 hr |
First Stage: Phases
Latent Phase: Little dilation, cervix softens/effaces. Duration variable — up to 20 hrs (nullipara), 14 hrs (multipara)
Active Phase: Dilation from ~6 cm → 10 cm. Cervix dilates at ≥1 cm/hr (nullipara) or ≥1.2 cm/hr (multipara)
Friedman Curve — Normal vs Abnormal Labor
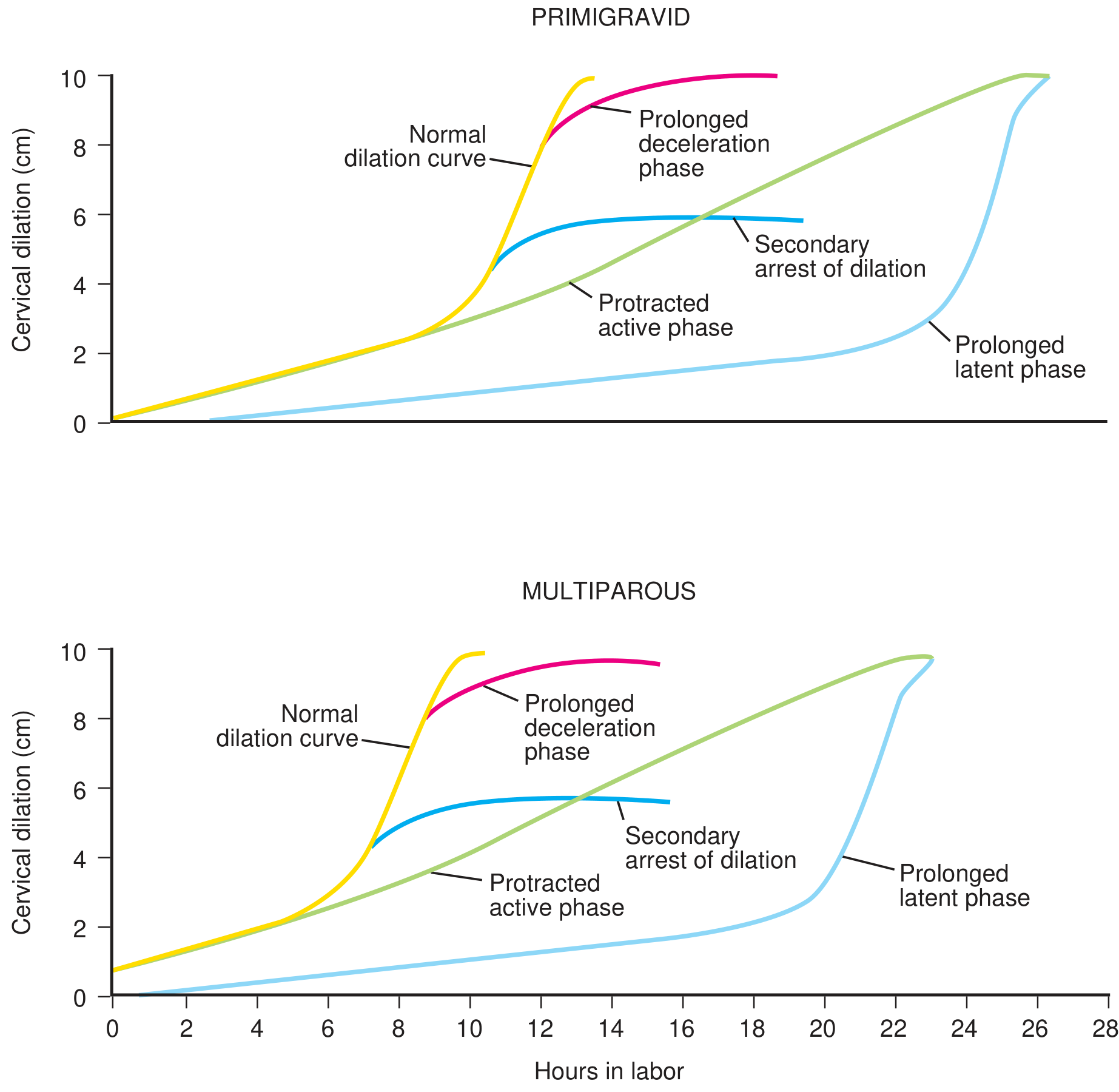
Abnormal patterns to know:
- Prolonged latent phase — >20 hrs (nullipara), >14 hrs (multipara)
- Protracted active phase — slow dilation rate
- Secondary arrest of dilation — stops at 5–6 cm
- Prolonged deceleration phase — slows near full dilation
Cardinal Movements of Labor (2nd Stage)
Mnemonic: "Every Fetal Infant Demands Immediate Expert Rearing"
- Engagement
- Flexion
- Internal rotation
- Descent
- Imminent crowning (Extension)
- External rotation (Restitution)
- Repulsion → Expulsion
Textbook of Family Medicine 9e
TOPIC 2: PREECLAMPSIA & ECLAMPSIA 🏆 [Highest yield in theory + viva]
Classification of Hypertensive Disorders of Pregnancy
| Type | BP | Timing | Proteinuria |
|---|---|---|---|
| Chronic HTN (cHTN) | ≥140/90 | <20 weeks or pre-existing | ± |
| Gestational HTN (gHTN) | ≥140/90 | ≥20 weeks | ❌ |
| Preeclampsia | ≥140/90 | ≥20 weeks | ✅ or other features |
| Eclampsia | ≥140/90 | Any time (incl. postpartum) | + Seizures |
Preeclampsia — Diagnosis
New-onset BP ≥140/90 mmHg on 2 occasions ≥4 hours apart after 20 weeks, PLUS:
- Proteinuria ≥300 mg/24 hrs, OR urine protein:creatinine ratio ≥0.3
Preeclampsia WITH Severe Features — Any 1 of:
- BP ≥160/110 mmHg on 2 occasions
- Platelets ≤100,000/μL (thrombocytopenia)
- Serum creatinine >1.1 mg/dL (or doubling without renal disease)
- Liver transaminases >2× normal
- Persistent epigastric / RUQ pain unresponsive to medication
- Pulmonary edema
- New-onset headache unresponsive to medication
- Visual disturbances
Mnemonic: "HELP + Visual HEadaches" → HELLP, Epigastric pain, Low platelets, Pulm edema + Visual, Headache
HELLP Syndrome
- H = Hemolysis
- EL = Elevated Liver enzymes
- LP = Low Platelets
Management — When to Deliver
| Condition | Deliver at |
|---|---|
| Preeclampsia without severe features | ≥37 weeks |
| Preeclampsia with severe features (stable) | ≥34 weeks |
| Preeclampsia with severe features (unstable), HELLP, Eclampsia | Soon after maternal stabilization |
Drugs
| Drug | Use |
|---|---|
| Magnesium sulfate (MgSO₄) | Seizure prophylaxis and treatment of eclampsia |
| Labetalol / Hydralazine / Nifedipine | Acute severe HTN control |
| NOT methyldopa acutely | Methyldopa is for maintenance/chronic |
MgSO₄ toxicity signs: Loss of DTRs (first sign), respiratory depression, cardiac arrest
Antidote: Calcium gluconate 10%
Swanson's Family Medicine Review; Creasy & Resnik's Maternal-Fetal Medicine
TOPIC 3: ANTEPARTUM HEMORRHAGE (APH) 🏆
Definition: Bleeding from genital tract after 28 weeks (viability) and before delivery of baby.
The Big 3 Causes
| Cause | Key Feature | Bleeding | Uterus | Pain |
|---|---|---|---|---|
| Placenta Previa | Low-lying placenta | Painless, bright red | Soft | ❌ |
| Placental Abruption | Premature separation | Dark, clotted ± concealed | Tender/woody hard | ✅ |
| Vasa Previa | Fetal vessels over os | Fetal blood loss | Soft | ❌ |
Placenta Previa
- Diagnosis: Ultrasound (do NOT do vaginal examination — causes massive bleed!)
- Management:
- If fetus immature + bleeding not profuse → Expectant management, admit, IV access, blood ready
- If severe or fetus mature → Cesarean section
- Vaginal birth is CONTRAINDICATED
- Anesthesia: Neuraxial preferred (if hemodynamically stable)
- Complication: Associated with placenta accreta — risk rises from 3% (1st C/S) to 61% with 3 prior cesareans
Placental Abruption
- Incidence: ~1% of deliveries, usually last 10 weeks
- Risk factors: Tobacco, cocaine, trauma, multiple gestation, hypertension, preeclampsia, PPROM
- Signs: Uterine tenderness + hypertonus, dark clotted blood, concealed bleeding possible
- Fetal mortality: 9–12% (developed countries); if >50% separation → likely stillbirth
- Complication: DIC (check coagulation studies!)
- Management: Depends on GA + severity — may need emergency C/S; if fetal death + stable mother → attempt vaginal delivery
Barash, Cullen & Stoelting's Clinical Anesthesia 9e; Creasy & Resnik's
TOPIC 4: POSTPARTUM HEMORRHAGE (PPH) 🏆
Definition
PPH = Blood loss ≥1,000 mL after any delivery (ACOG updated definition), OR any blood loss with signs/symptoms of hypovolemia within 24 hours of birth.
(Old definition: >500 mL vaginal, >1,000 mL cesarean)
The "4 T's" — Causes of PPH
| T | Cause | % of PPH |
|---|---|---|
| Tone | Uterine atony | >70% (most common!) |
| Trauma | Lacerations, uterine rupture | 20% |
| Tissue | Retained placenta/products | 10% |
| Thrombin | Coagulopathy | <1% |
Risk Factors for Atony (Mnemonic "O-F-M-A-L-C")
- Overdistension (multiple gestation, polyhydramnios)
- Fatigue (prolonged labor)
- Magnesium sulfate
- Augmentation with oxytocin
- Labor induction
- Chorioamnionitis
Management
- Bimanual uterine massage + IV oxytocin (do NOT give as IV bolus — causes hypotension!)
- Uterotonics: Oxytocin → Ergometrine/Syntometrine → Misoprostol → Carboprost (PGF2α)
- Surgical: B-Lynch suture, uterine artery ligation, hysterectomy (last resort)
- Jada system (intrauterine vacuum device) — >90% control of atony-related PPH
Active management of 3rd stage = oxytocin before placenta delivery → reduces PPH risk
Clinical Anesthesia 9e; Textbook of Family Medicine 9e; Roberts & Hedges' Emergency Procedures
TOPIC 5: GESTATIONAL DIABETES MELLITUS (GDM)
Screening
- When: After 24 weeks (USPSTF recommendation)
- How: 50g oral glucose challenge test (GCT) — blood glucose at 1 hour
- Abnormal if ≥140 mg/dL → proceed to diagnostic OGTT
Diagnosis — 100g 3-hour OGTT (Carpenter-Coustan criteria)
| Time | Abnormal value |
|---|---|
| Fasting | ≥95 mg/dL |
| 1 hour | ≥180 mg/dL |
| 2 hour | ≥155 mg/dL |
| 3 hour | ≥140 mg/dL |
≥2 abnormal values = GDM diagnosis
Management
- Diet (30–35 kcal/kg lean body weight) + Exercise (walking)
- Targets: Fasting <105 mg/dL, 2-hr postprandial <120 mg/dL
- If not achieved → Insulin therapy
- USG every 4–6 weeks (fetal size), HbA1c every 4–6 weeks
- Antenatal testing in 3rd trimester for insulin-requiring patients
Neonatal Complications (if poorly controlled)
- Hypoglycemia
- Hypocalcemia
- Polycythemia
- Hyperbilirubinemia
- Macrosomia (→ shoulder dystocia risk)
Long-term Risk
- Mother: 30–60% chance of developing Type 2 DM lifetime
- Recommend postpartum and yearly glucose tolerance testing
Textbook of Family Medicine 9e
TOPIC 6: PRETERM LABOR (PTL)
Definition: Labor before 37 completed weeks gestation
- Between 24–34 weeks = treatment may be initiated to delay delivery
Management Goals
- Tocolysis (delay delivery 48 hrs to give steroids): Nifedipine, Indomethacin, Terbutaline, Magnesium sulfate (also neuroprotective at <32 weeks)
- Antenatal corticosteroids: Betamethasone or Dexamethasone (12 mg IM × 2 doses, 24 hrs apart) → accelerates fetal lung maturity
- GBS prophylaxis if GBS status unknown or positive
- Progesterone (17-OHPC) — used for prevention in women with prior preterm birth
TOPIC 7: PREMATURE RUPTURE OF MEMBRANES (PROM)
| Type | Definition |
|---|---|
| PROM | Membrane rupture at term (≥37 wks) before onset of labor |
| PPROM | Premature PROM — rupture before 37 weeks |
Diagnosis
- Pooling of fluid in vagina
- Nitrazine test — turns blue (alkaline pH)
- Ferning on microscopy
- USG — oligohydramnios
Management of PPROM
| GA | Action |
|---|---|
| ≥34 weeks | Deliver |
| 24–33 weeks | Expectant management + Antibiotics (ampicillin + erythromycin) + Steroids |
| <24 weeks | Counseling (periviable) |
TOPIC 8: NORMAL PUERPERIUM
Puerperium = Period from delivery of placenta until 6 weeks postpartum
Lochia (postpartum vaginal discharge)
| Type | Duration | Color |
|---|---|---|
| Lochia rubra | Days 1–4 | Red (blood) |
| Lochia serosa | Days 4–10 | Pink/brown |
| Lochia alba | Day 10 → 6 weeks | White/yellow |
Important Changes
- Uterus involutes at 1 cm/day (at umbilicus immediately after delivery, reaches pelvis by ~10 days)
- Menstruation returns: ~6–8 weeks (non-breastfeeding); may be delayed for months in breastfeeding
- Postpartum blues vs Postpartum depression (>2 weeks) vs Postpartum psychosis (emergency)
QUICK RECALL TABLES 📋
High-Yield Numbers to Memorize
| Fact | Number |
|---|---|
| Full cervical dilation | 10 cm |
| Latent phase limit (nullipara) | 20 hours |
| Latent phase limit (multipara) | 14 hours |
| Preeclampsia BP cutoff | ≥140/90 mmHg |
| Severe preeclampsia BP cutoff | ≥160/110 mmHg |
| Proteinuria in preeclampsia | ≥300 mg/24 hrs |
| Platelets in severe PE | ≤100,000/μL |
| PPH blood loss cutoff (ACOG) | ≥1,000 mL |
| GDM screening timing | After 24 weeks |
| GDM GCT abnormal | ≥140 mg/dL at 1 hr |
| Abruption: stillbirth risk | >50% separation |
| Placenta accreta risk (3 C/S) | 61% |
| APH definition | ≥28 weeks |
| Preeclampsia delivery (no severe) | ≥37 weeks |
| Preeclampsia delivery (severe, stable) | ≥34 weeks |
MASTER MNEMONIC SHEET 🧠
| Topic | Mnemonic |
|---|---|
| Severe preeclampsia features | "HELP + VH" (HELLP, Epigastric pain, Low plts, Pulm edema, Visual, Headache) |
| Causes of PPH | "4 T's" — Tone, Trauma, Tissue, Thrombin |
| Cardinal movements | "Every Fetal Infant Demands Immediate Expert Rearing" |
| GDM neonatal complications | "4 H's" — Hypoglycemia, Hypocalcemia, Hyperbilirubinemia, High hematocrit (polycythemia) |
| Abruption risk factors | "THCMP" — Tobacco, Hypertension, Cocaine, Multiparity, Preeclampsia |
EXAM STRATEGY FOR OBSTETRICS
Theory Paper: Focus on preeclampsia criteria, APH comparison table, PPH management algorithm
Short notes commonly asked:
- HELLP syndrome
- Active management of 3rd stage
- Placenta previa vs abruption
- Bishop score
- GDM screening
- MgSO₄ toxicity and antidote
Viva hot topics:
- Differentiate true vs false labor
- When do you deliver in preeclampsia?
- What is Bishop score and when do you use it?
- What is the first drug for PPH?
- What are the 4 T's?
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Textbook of Family Medicine 9e; Swanson's Family Medicine Review; Barash Clinical Anesthesia 9e; Morgan & Mikhail's Clinical Anesthesiology
What to Study Next (in order)
- ✅ Normal labor (done above)
- ✅ Preeclampsia/Eclampsia (done above)
- ✅ APH — Previa vs Abruption (done above)
- ✅ PPH and 4 T's (done above)
- ✅ GDM (done above)
- 📌 Malpresentations (breech, shoulder, brow, face)
- 📌 Cord prolapse (emergency management)
- 📌 Instrumental delivery (forceps vs ventouse)
- 📌 Antenatal care (ANC schedule, investigations)
- 📌 Contraception (MBBS exams increasingly ask this)
Ask me about any specific topic on this list and I'll give you a deep dive with clinical scenarios, MCQs, and practice questions!
This is a shared conversation. Sign in to Orris to start your own chat.