Uterus types
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
Here is a complete overview of the types of uterus, organized by the two main classification schemes: positional variants and congenital structural anomalies.
Types of Uterus
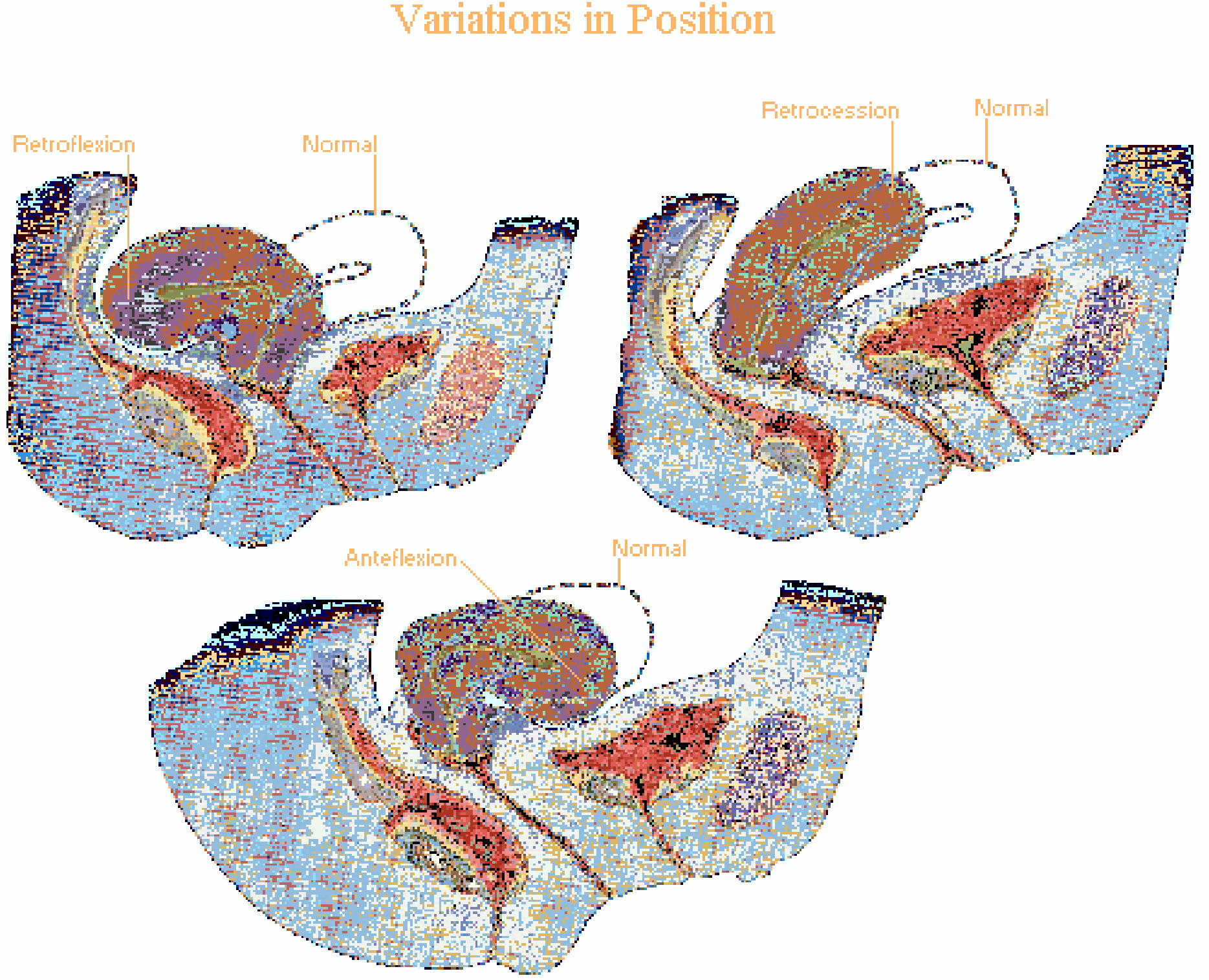
A. Positional Variants (Normal vs. Abnormal Position)
The uterus can vary in its version (angle relative to vagina) and flexion (angle of body on cervix):
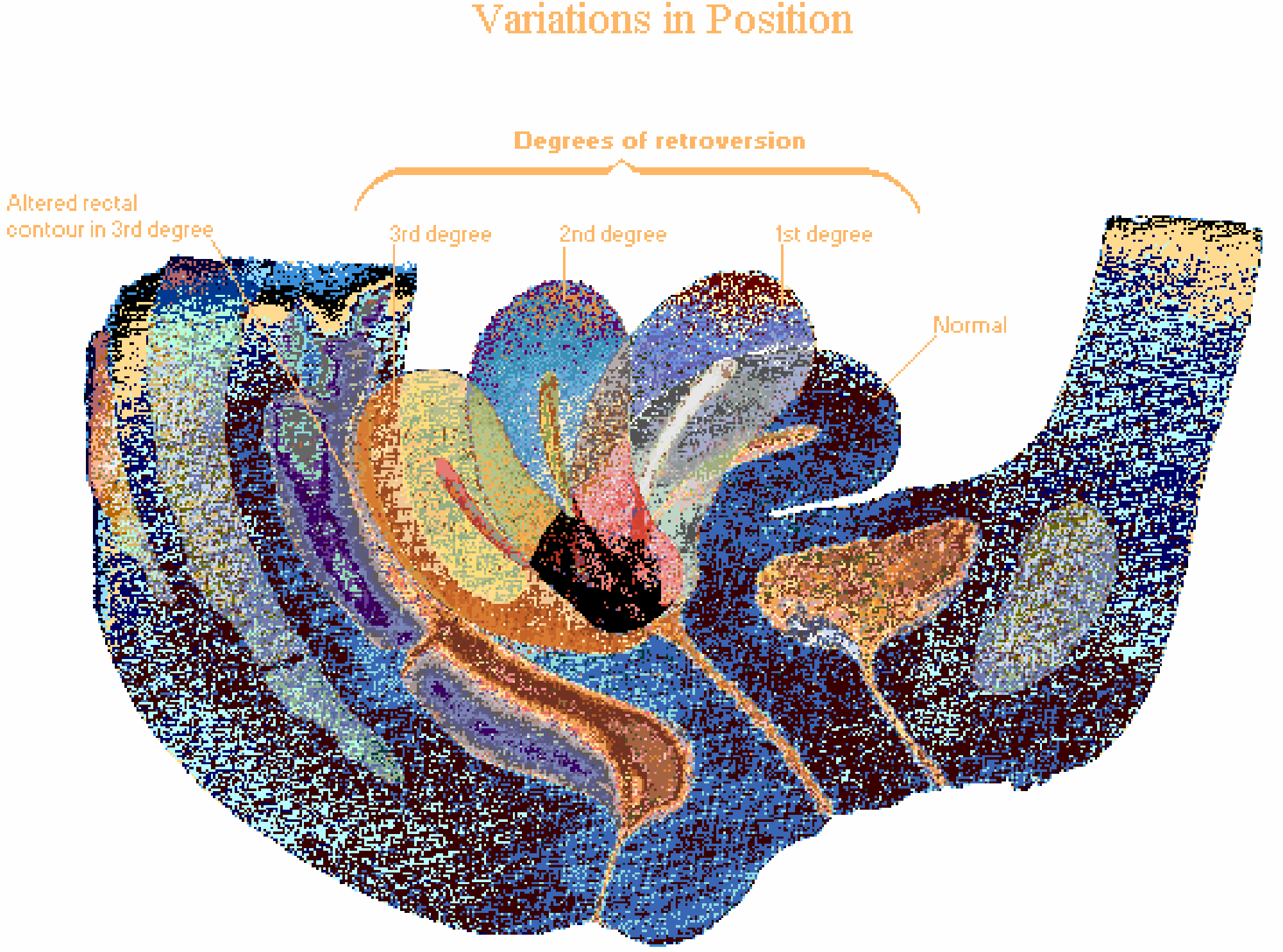
Version (Relationship of uterus to vaginal axis)
| Type | Description |
|---|---|
| Anteversion (normal) | Uterus tilts forward over the bladder (~80% of women) |
| Retroversion | Uterus tilts backward toward the rectum |
| Retroversion - degrees | 1st, 2nd, and 3rd degree based on extent of backward tilt; 3rd degree alters the rectal contour |
| Retrocession | Entire uterus displaced posteriorly in the pelvis |
Flexion (Relationship of body to cervix)
| Type | Description |
|---|---|
| Anteflexion (normal) | Body of uterus bent forward on the cervix |
| Retroflexion | Body of uterus bent backward on the cervix |
From Netter's Atlas of Human Anatomy (Variations in Position):
B. Congenital Structural Anomalies (Mullerian Duct Anomalies)
These result from failures in the fusion, development, or canalization of the paramesonephric (Mullerian) ducts during the 8th week of gestation. They occur in ~3-4% of women, rising to 25% in those with recurrent pregnancy loss.
From Berek & Novak's Gynecology and The Developing Human (Moore):
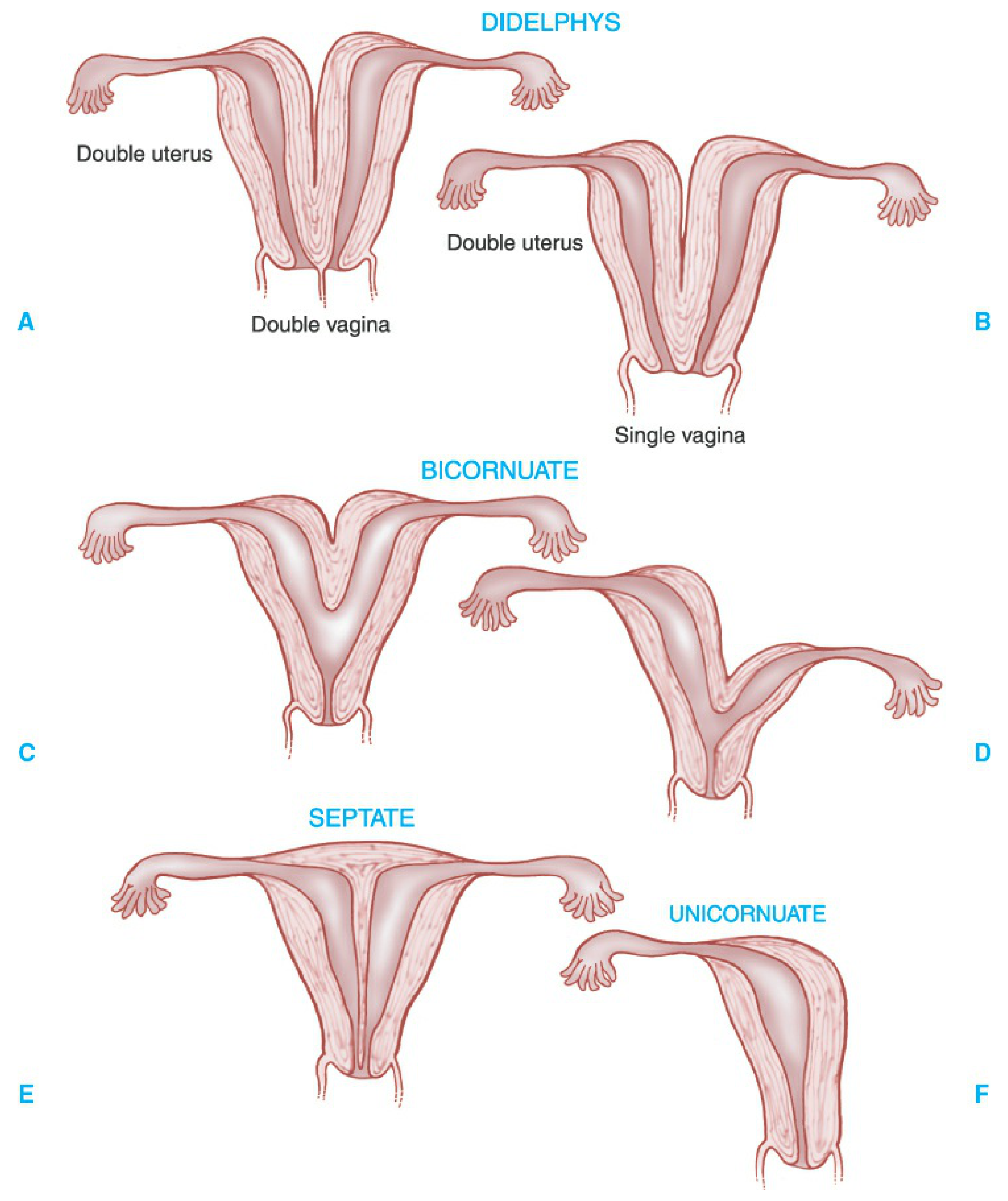
1. Uterus Didelphys (Double Uterus)
- Complete failure of fusion of both inferior paramesonephric ducts
- Results in two separate uterine bodies and two cervices
- May have double vagina or single vagina
- Caused by: failure of fusion of the inferior parts of the paramesonephric ducts
2. Bicornuate Uterus
- Incomplete fusion involving only the superior part of the uterine body
- Two uterine horns (cornua) with a shared lower uterine segment/cervix
- Bicornuate with rudimentary horn: Growth retardation of one duct causes one full horn and one small, non-communicating horn
3. Septate Uterus
- External shape appears normal but the interior is divided by a fibrous/fibromuscular septum
- Most common uterine anomaly
- Results from failure of resorption of the intervening septum after duct fusion
- Most strongly associated with recurrent pregnancy loss; hysteroscopic metroplasty significantly reduces pregnancy loss rates
4. Unicornuate Uterus
- One paramesonephric duct fails to develop entirely
- Single uterine horn with only one fallopian tube
- Associated with increased preterm delivery and recurrent pregnancy loss
5. Arcuate Uterus
- Mildest anomaly - slight saddle-shaped indentation at the fundus
- Considered a normal variant by many; live birth rates comparable to normal uterus
6. T-shaped Uterus
- Associated with in utero DES (diethylstilbestrol) exposure
- Narrow, T-shaped uterine cavity
- Associated with obstetric complications (preterm birth, ectopic pregnancy)
C. Acquired Uterine Anomalies
These are not congenital but alter uterine structure:
| Condition | Effect |
|---|---|
| Leiomyomas (fibroids) | Submucosal, intramural, subserosal - distort cavity depending on type |
| Intrauterine adhesions (Asherman's syndrome) | Post-surgical or post-infectious scarring obliterates cavity |
| Endometrial polyps | Focal overgrowth of endometrium |
Key Clinical Notes
- Renal anomalies frequently co-exist with Mullerian anomalies (paramesonephric and urinary systems develop in close proximity) - urologic imaging is recommended whenever a Mullerian anomaly is diagnosed
- Uterine anomalies are more associated with pregnancy wastage than infertility
- Septate uterus has the worst obstetric outcomes among structural anomalies; hysteroscopic metroplasty is recommended
- Rudimentary horns require surgical removal on diagnosis
- Mullerian agenesis (Mayer-Rokitansky-Kuster-Hauser syndrome): absent uterus and vagina; genetic children only possible via IVF with gestational carrier
Sources: Berek & Novak's Gynecology; The Developing Human - Clinically Oriented Embryology; Netter's Atlas of Human Anatomy; Creasy & Resnik's Maternal-Fetal Medicine
Fallopian tube parts
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Here is a complete breakdown of the parts of the fallopian tube (also called the uterine tube / oviduct):
Parts of the Fallopian Tube
The fallopian tubes are paired bilateral structures, approximately 10-14 cm in total length, originating at the upper lateral cornua of the uterus and extending laterally to coil around each ovary.
The 4 Anatomical Segments (Medial → Lateral)
| # | Segment | Length | Key Features |
|---|---|---|---|
| 1 | Intramural (Interstitial) | 1-2 cm | Passes through the myometrium of the uterine wall; completely surrounded by myometrium; narrowest lumen (~1 mm) |
| 2 | Isthmus | ~4 cm | Narrow, straight portion immediately beyond the uterine wall; most muscular segment; thick-walled with small lumen |
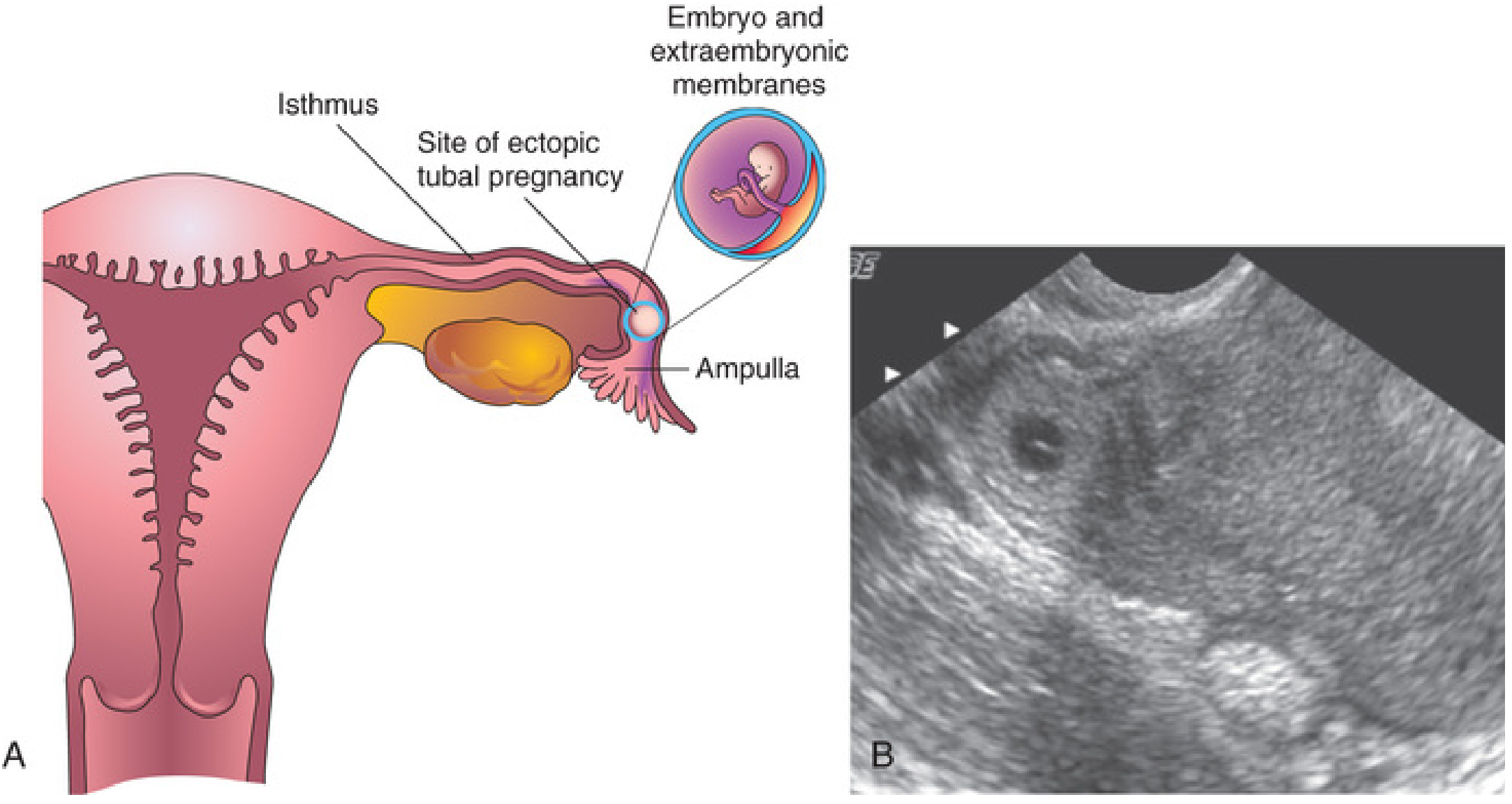
| 3 | Ampulla | 4-6 cm | Widest and longest segment; thin-walled and tortuous; site of fertilization; free of broad ligament laterally |
| 4 | Infundibulum | ~1 cm | Funnel-shaped distal end; surrounded by fimbriae (finger-like projections); opens directly into the peritoneal cavity |
The Fimbriae
- Frond-like finger projections at the infundibulum
- Surround the ostium (opening of the tube)
- The fimbria ovarica is the longest fimbria, attached to the ovary
- Function: sweep the oocyte from the ovarian surface into the tube after ovulation
Wall Layers (3 Layers)
| Layer | Description |
|---|---|
| Serosa (Adventitia) | Outermost layer; continuous with the broad ligament (mesosalpinx) |
| Muscularis | Middle layer of smooth muscle; inner circular and outer longitudinal bundles; thickest at the isthmus; generates peristaltic contractions |
| Mucosa | Innermost layer; highly folded (most complex in the ampulla); simple columnar epithelium |
Mucosal Epithelium Cell Types
The mucosa is lined by simple columnar epithelium with two main cell types:
| Cell Type | Function |
|---|---|
| Ciliated cells | Beat toward the uterus; propel the oocyte/zygote along the tube |
| Non-ciliated (peg/secretory) cells | Produce fluid that nourishes the oocyte and facilitates capacitation of sperm |
The ratio of ciliated to secretory cells varies by region - the ampulla has the most ciliated cells; the isthmus has the most secretory cells.
Transport of Oocyte
- After ovulation, fimbriae sweep the oocyte into the infundibulum
- Peristaltic contractions + ciliary action propel it through the infundibulum → ampulla
- Fertilization occurs in the ampulla
- The zygote takes 3-4 days to transit the tube and reach the uterine cavity
Blood Supply
- Branches of the ovarian artery (lateral 2/3) and uterine artery (medial 1/3)
- Travel through the mesosalpinx (peritoneal fold forming the upper border of the broad ligament)
Nerve Supply
- Both sympathetic and parasympathetic via the uterine and ovarian plexuses
Clinical Relevance
| Condition | Segment involved |
|---|---|
| Ectopic pregnancy | Most common in the ampulla (~70%); also isthmus (~12%) - isthmic rupture occurs earlier and is more dangerous |
| Pelvic inflammatory disease (PID) | Ascending infection scars the mucosa |
| Hydrosalpinx | Distal tube obstruction with fluid accumulation |
| High-grade serous ovarian cancer | Most now believed to originate in the fallopian tube (fimbriated end) |
Sources: Sabiston Textbook of Surgery; Schwartz's Principles of Surgery; Histology: A Text and Atlas (Pawlina); The Developing Human - Clinically Oriented Embryology
Ectopic pregnancy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information to deliver a detailed answer. Let me compile everything.
Ectopic Pregnancy
An ectopic pregnancy is implantation of the fertilized ovum outside the uterine cavity. It accounts for approximately 1-2% of all pregnancies and is the 3rd leading cause of maternal death (responsible for ~2.7-10% of maternal deaths).
Sites of Implantation
| Site | Frequency | Notes |
|---|---|---|
| Fallopian tube (overall) | ~95-98% | Most common site |
| - Ampulla | ~70% | Most common tubal site |
| - Isthmus | ~12% | Ruptures earlier, more dangerous |
| - Fimbriae | ~11% | |
| - Interstitial (cornual) | ~2-3% | Highest mortality; ruptures late at 8-16 wks with massive hemorrhage |
| Ovarian | ~0.5-1% | |
| Cervical | <1% | |
| Abdominal | ~1% | Can progress to advanced gestational age; very rare |
| Heterotopic | ~1:4,000 | Simultaneous intra + extrauterine; higher with ART |
Risk Factors
Most important risk factor = Prior ectopic pregnancy (recurrence risk 10-15% after first, 30% after second)
| Risk Factor | Notes |
|---|---|
| Prior ectopic pregnancy | Strongest single risk factor |
| Pelvic inflammatory disease (PID) | Tubal damage in ~90% of ectopics; Chlamydia cultured in 7-30% |
| Tubal surgery / sterilization | Sterilization failure → 10-year ectopic rate ~7.3/1,000 |
| Assisted reproductive technology (IVF) | Multiple embryo transfer increases heterotopic risk |
| History of infertility | Increases risk 4-40x depending on cause |
| IUD in situ | If pregnancy occurs despite IUD, more likely ectopic |
| Smoking | Dose-dependent; alters tubal motility and ciliary activity |
| Endometriosis | Tubal/peritoneal scarring |
| Salpingitis isthmica nodosa | |
| Prior abdominal/pelvic surgery |
Up to 50% of women with ectopic pregnancy have no identifiable risk factor - so a high index of suspicion is always required.
Pathophysiology
- Fertilized ovum normally reaches the uterus in ~3-4 days via ciliary action + peristalsis
- Any factor delaying transit through the tube leads to implantation before reaching the uterus
- The fallopian tube cannot support placentation - trophoblastic invasion leads to erosion of tubal wall → rupture and hemorrhage
- Isthmic ectopics rupture earlier (thinner wall, smaller lumen) than ampullary ones
Clinical Features
Classic Triad (present in ~50% of cases)
- Abdominal/pelvic pain (most common - may be unilateral, dull/sharp/crampy)
- Amenorrhea (missed period ~6-8 weeks)
- Vaginal bleeding (usually light, dark spotting)
Additional Symptoms
- Shoulder tip pain - referred pain from diaphragmatic irritation by hemoperitoneum (indicates rupture)
- Syncope / dizziness with rupture
- Transient pain relief can occur with rupture (stretching of tubal serosa ceases)
Physical Examination
| Finding | Notes |
|---|---|
| Adnexal tenderness | Most consistent sign |
| Adnexal mass | Palpable in ~50% (may be corpus luteum, not ectopic itself) |
| Cervical motion tenderness | Variable |
| Ruptured: tachycardia, hypotension, rigid abdomen, rebound | Hemodynamic instability = emergency |
Diagnosis
1. Beta-hCG (Serum Quantitative)
- Positive in virtually all ectopic pregnancies
- In normal IUP: doubles every 48 hours (minimum 53-66% rise)
- In ectopic: slower rise, plateau, or abnormal decline
- Discriminatory zone: β-hCG level at which an IUP should be visible on TVUS
- Transvaginal: 1,500-2,000 mIU/mL (some institutions use 3,510 mIU/mL to avoid false positives)
- No IUP seen above discriminatory zone → strongly suspect ectopic
- Note: ectopic hCG does NOT correlate with ectopic size
2. Serum Progesterone
- >25 ng/mL: strongly suggests viable IUP (only 1-2% of ectopics this high)
- <5 ng/mL: suggests non-viable pregnancy (IUP or ectopic)
3. Transvaginal Ultrasound (TVUS)
- Imaging modality of choice
- Key findings:
- Empty uterine cavity
- Pseudogestational sac (intrauterine fluid collection): occurs in 8-29% of ectopics; mimics IUP
- Double decidual sac sign (DDSS): two echogenic rings = true IUP
- Adnexal ring sign: echogenic ring around extrauterine sac (seen in <50% of ectopics)
- Complex/solid adnexal mass
- Free fluid in the cul-de-sac (not proof of rupture)
- Intra-abdominal free fluid above the uterus → suggests rupture
4. Dilation and Curettage (D&C)
- Performed when pregnancy confirmed non-viable and location unknown
- Presence of chorionic villi (float in saline, lacy frond appearance) = IUP
- Absence of villi with declining hCG post-curettage = ectopic
Treatment
Treatment depends on: hemodynamic stability, ectopic site, size, hCG level, patient's fertility goals, and resources.
A. Expectant Management
- Reserved for selected stable patients with: declining hCG, small ectopic, no cardiac activity, reliable follow-up
- Close serial hCG monitoring required
B. Medical Treatment: Methotrexate (MTX)
MTX is a folic acid antagonist that inhibits trophoblastic cell division.
Eligibility criteria (all must be met):
- Hemodynamically stable
- Unruptured ectopic
- No contraindications to MTX
- Reliable for follow-up
- hCG typically <5,000 mIU/mL (higher levels = higher failure rate)
- Ectopic mass <4 cm (with no cardiac activity)
Absolute contraindications:
- Hemodynamic instability / rupture
- Breastfeeding
- Immunodeficiency
- Renal/hepatic/hematologic dysfunction
- Active pulmonary disease
- Peptic ulcer disease
- Sensitivity to MTX
- Intrauterine pregnancy
Regimens:
| Regimen | Dose | Monitoring | Success Rate |
|---|---|---|---|
| Single dose | 50 mg/m² IM on day 1 | β-hCG days 4 & 7; if <15% drop → 2nd dose | ~78-96% overall; 15-20% need 2nd dose |
| Two-dose | MTX day 0 and day 4 | β-hCG days 4 & 7 | ~87% |
| Multidose | 1 mg/kg IM days 1,3,5,7 + leucovorin alternate days | β-hCG each treatment day | Higher efficacy, more side effects |
Side effects (dose-dependent): nausea, vomiting, stomatitis, abdominal pain (30-40%); bone marrow suppression, hepatotoxicity, alopecia, pneumonitis (less common)
Post-MTX precautions: Avoid alcohol, NSAIDs, folate supplements, sexual intercourse, sun exposure; avoid new pregnancy for 3 months
C. Surgical Treatment
- Indicated for: rupture, hemodynamic instability, MTX failure/contraindication, or patient preference
| Approach | Preferred over | Notes |
|---|---|---|
| Laparoscopy | Laparotomy in most cases | Shorter hospital stay, less blood loss, faster recovery, fewer adhesions |
| Laparotomy | When hemodynamically unstable, extensive adhesions, or abdominal pregnancy | Faster entry if hemorrhage is massive |
Procedures:
| Procedure | When Used | Notes |
|---|---|---|
| Salpingectomy | Ruptured tube, patient not concerned with ipsilateral fertility, severely damaged tube | Recurrent ectopic rate lower (4% vs 10% with salpingostomy) |
| Salpingostomy (linear) | Unruptured ectopic, patient wants to preserve fertility, contralateral tube absent/damaged | Risk of persistent ectopic ~8%; post-op weekly hCG monitoring required |
| Milking | Only if fimbrial location | Associated with higher recurrence; generally not recommended for ampullary ectopics |
Reproductive Outcomes After Treatment
| Treatment | Subsequent IUP Rate | Recurrent Ectopic Rate | Tubal Patency |
|---|---|---|---|
| Laparoscopic salpingostomy | ~60% | ~10% | ~84% ipsilateral |
| Laparoscopic salpingectomy | ~54% | ~4% | N/A |
| Methotrexate | 36-64% | ~10% | >80% |
- No significant difference in future fertility between MTX and salpingostomy overall
Special Types
Interstitial (Cornual) Ectopic
- Located in myometrial portion of tube
- Larger blood supply → late rupture at 8-16 weeks, massive hemorrhage
- Treatment: MTX preferred if unruptured; surgical = cornual resection
Cervical Ectopic
- Implants in cervical canal
- Conservative options: MTX, uterine artery ligation + hysteroscopic resection
- Hysterectomy sometimes required
Ovarian Ectopic
- Criteria (Spiegelberg): tube intact on same side, mass in ovarian position, ovarian tissue in wall, connected to uterus by utero-ovarian ligament
- Treatment: cystectomy/wedge resection; MTX has been used successfully
Abdominal Ectopic
- Most dangerous; can reach advanced gestation
- Treatment: surgical - laparotomy (placenta removal risks massive hemorrhage; often left in situ)
Sources: Berek & Novak's Gynecology; Rosen's Emergency Medicine; Schwartz's Principles of Surgery; Creasy & Resnik's Maternal-Fetal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.