Causes of postcoital p/v bleeding
Causes of Postcoital (Per Vaginal) Bleeding
1. Cervical Causes (most common overall)
| Cause | Notes |
|---|---|
| Cervical ectropion (erosion) | Eversion of fragile columnar endocervical epithelium onto the ectocervix; bleeds on contact. Common in OCP users and pregnancy. |
| Cervical polyp | Pedunculated benign growths from the endocervical canal; bleed easily on contact |
| Cervicitis | Inflammation from STIs — Chlamydia trachomatis (most common), Neisseria gonorrhoeae, Trichomonas vaginalis, HSV; manifests as cervical friability |
| Cervical intraepithelial neoplasia (CIN) / Cervical carcinoma | PCB is a hallmark symptom; must be excluded regardless of Pap smear status — colposcopy is indicated for any unexplained PCB |
| Condylomata acuminata (HPV) | Friable lesions on the cervix or vaginal walls |
| Nabothian cysts | Usually innocent; rarely bleed |
2. Vaginal Causes
| Cause | Notes |
|---|---|
| Atrophic vaginitis | Postmenopausal hypoestrogenic mucosa is fragile and tears easily during intercourse |
| Vaginal lacerations / trauma | The most common mechanism of genital injury in adult women is coitus itself; ranges from minor contusions to deep lacerations |
| Vaginal candidiasis / trichomoniasis | Inflamed, friable vaginal epithelium |
| Vaginal carcinoma | Rare but important to exclude |
| Foreign body | May cause inflammation and contact bleeding |
3. Uterine / Endometrial Causes
| Cause | Notes |
|---|---|
| Endocervical / endometrial polyps | Polyps prolapsing through the os can bleed post-coitally |
| Endometrial carcinoma | Less commonly presents as PCB; more typical of postmenopausal bleeding |
| Submucosal fibroids | May cause irregular and contact bleeding |
4. Pregnancy-Related Causes
| Cause | Notes |
|---|---|
| Physiological (increased cervical vascularity) | PCB is more common in pregnancy due to increased cervical blood flow |
| Threatened / inevitable abortion | Any trimester |
| Ectopic pregnancy | First trimester; associated with pain |
| Cervical carcinoma in pregnancy | Must be excluded |
| Placenta previa | Second/third trimester — do NOT perform digital exam without USS |
5. Iatrogenic / Other
| Cause | Notes |
|---|---|
| IUD (intrauterine device) | Copper IUD especially can increase bleeding; misplaced string |
| Exogenous hormones / OCP | Breakthrough bleeding; missed doses |
| Tamoxifen use | Associated with endometrial polyps; must sample |
| Coagulopathy | von Willebrand disease, thrombocytopenia; predispose to abnormal bleeding at any site |
| Schistosomiasis haematobium | Genitourinary granulomas causing contact bleeding (in endemic areas) |
Key Clinical Pearls
- Abnormal PCB should always prompt colposcopy, regardless of a normal Pap smear — cervical cancer must be excluded — Pfenninger & Fowler's Procedures for Primary Care
- In postmenopausal women, any PCB warrants endometrial sampling to exclude malignancy — Berek & Novak's Gynecology
- Chlamydial cervicitis is an important and often missed cause, particularly in adolescents and young women — Berek & Novak's Gynecology
- In pregnancy, PCB with cervical motion tenderness/discharge suggests PID or STI — Rosen's Emergency Medicine
Vaginal lacerations / trauma post coitus causes of heavy bleeding
Causes of Heavy Bleeding from Vaginal/Coital Trauma
Why Coital Lacerations Can Bleed Heavily
Predisposing Factors for Heavy Coital Bleeding
1. Anatomical / Site-Related
| Factor | Mechanism |
|---|---|
| Posterior fornix laceration | Most common site of serious coital injury; thin wall adjacent to pouch of Douglas; vessels close to surface |
| Vaginal vault laceration | Following hysterectomy, the vault suture line is a weak point susceptible to penetrative injury |
| Hymenal tears (first intercourse) | Minor but occasionally bleeds significantly; rarely severe unless underlying coagulopathy |
2. Tissue Fragility
| Condition | Mechanism |
|---|---|
| Atrophic vaginitis (postmenopausal) | Hypoestrogenic mucosa is thin, inelastic, poorly lubricated — tears at minimal force |
| Post-radiation vaginitis | Radiation-induced fibrosis and poor vascularity paradoxically causes fragility and impaired healing |
| Lichen sclerosus | Pale, atrophic, friable epithelium; splits easily |
| Lichen planus / erosive vulvovaginitis | Ulcerated and inflamed surfaces |
| Inflammatory vaginitis | Inflamed mucosa is hyperaemic and bleeds more readily |
3. Mechanical / Situational Factors
| Factor | Mechanism |
|---|---|
| Inadequate lubrication / arousal | Friction injury to urothelium |
| Unusual/forceful coital positions | Increased shearing force on posterior fornix |
| Foreign object penetration | Irregular objects cause deeper or wider lacerations |
| Sexual assault / rape | Non-consensual intercourse with struggling — higher force, unprepared tissues |
| First coitus (defloration) | Hymenal and introital tears |
4. Underlying Bleeding Diatheses
| Condition | Notes |
|---|---|
| Von Willebrand disease | Most common inherited coagulopathy; minor trauma → disproportionate bleeding |
| Thrombocytopenia | ITP, haematological malignancy, medication-induced |
| Anticoagulant therapy | Warfarin, DOACs, heparin |
| Liver disease | Coagulopathy from reduced clotting factor synthesis |
| DIC | Consumption of clotting factors |
5. Vascular Abnormalities
| Condition | Notes |
|---|---|
| Arteriovenous malformation (AVM) of vagina/uterus | Rare; can cause catastrophic haemorrhage from minor trauma |
| Varicosities | Pelvic or vulvovaginal varices (seen in pregnancy, portal hypertension) |
| Pregnancy-related hypervascularity | Markedly increased blood flow to cervix and vagina in pregnancy — any laceration bleeds heavily |
AAST Vaginal Injury Scale (severity grading)
| Grade | Injury |
|---|---|
| I | Contusion or haematoma |
| II | Laceration — superficial (mucosa only) |
| III | Laceration — deep (into fat or muscle) |
| IV | Laceration — complex, into cervix or peritoneum |
| V | Injury into adjacent organs (anus, rectum, urethra, bladder) |
Red Flags Warranting Urgent Surgical Evaluation
- Haemodynamic instability after coital trauma
- Bleeding not controlled by direct pressure
- Suspected posterior fornix / peritoneal extension
- Expanding pelvic haematoma
- Post-hysterectomy vault laceration
- Injury following assault with foreign object
Posterior fornix laceration Most common site of serious coital injury; thin wall adjacent to pouch of Douglas; vessels close to surface.
posterior fornix vagina anatomy pouch of Douglas sagittal
Posterior Fornix Laceration — Anatomy & Why It Causes Heavy Bleeding
Anatomical Basis
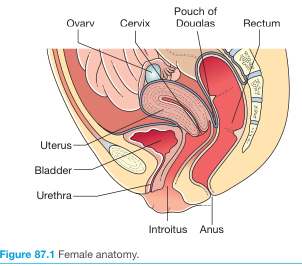
"The posterior vaginal fornix is separated from the posterior cul-de-sac and peritoneal cavity by the vaginal wall and peritoneum." — Berek & Novak's Gynecology
- Anteriorly: posterior surface of uterus, cervix, and posterior vaginal fornix
- Posteriorly: anterior wall of rectum
- Laterally: uterosacral ligaments
Why the Posterior Fornix Bleeds So Heavily
1. Thin wall — only two layers between vaginal lumen and peritoneum
- The thin vaginal wall (mucosa + submucosa + a thin muscularis)
- A layer of peritoneum
2. Rich vascular supply immediately adjacent
- Vaginal artery (branch of internal iliac artery)
- Descending branch of the uterine artery — runs laterally at 3 o'clock and 9 o'clock at the cervix, with anastomoses extending into the fornix
- Anastomotic plexus with middle rectal and internal pudendal arteries
3. Intraperitoneal haemorrhage — "hidden" bleeding
- Blood can pour freely into the abdomen without proportionate external PV bleeding
- The patient may present with haemodynamic shock with surprisingly little visible blood
- This is the same reason culdocentesis (needle aspiration through the posterior fornix) is used to detect haemoperitoneum in ruptured ectopic pregnancy
4. Retroperitoneal extension
Clinical Presentations of Posterior Fornix Laceration
| Severity | Presentation |
|---|---|
| Minor | Superficial mucosal tear, controlled PV bleeding |
| Moderate | Deep laceration into fat/muscle, heavy PV bleeding, haematoma |
| Severe | Full-thickness breach into peritoneal cavity, haemoperitoneum, peritonitis, shock |
| Catastrophic | Vascular injury to uterine/vaginal artery branch — uncontrolled haemorrhage |
High-Risk Scenarios for Posterior Fornix Laceration
- Forceful or unusual coital positions (woman astride — penis directed toward posterior fornix)
- Atrophic postmenopausal vagina — thin walls, poor elasticity, inadequate lubrication
- First intercourse — unrelaxed introitus directs force posteriorly
- Sexual assault — non-consensual, struggle, unprepared tissues
- Post-hysterectomy vault — vault scar is relatively avascular and inelastic; vault dehiscence can occur with vigorous intercourse
- Foreign body penetration — irregular objects, deeper/wider trajectory
Management Principles
- Examination under anaesthesia (EUA) — mandatory if bleeding not adequately assessed in outpatient setting
- Suture repair under direct vision
- If peritoneal breach suspected → laparoscopy/laparotomy
- Uterine artery embolisation for uncontrolled haemorrhage
- Monitor for delayed haemoperitoneum
Guidelines for treatment of vaginal tear grade 4
vaginal laceration repair management guidelines
PMID: 39581327
ACOG RCOG guidelines treatment grade 4 vaginal laceration coital tear management 2023 2024
Treatment of Grade 4 Vaginal/Perineal Tear — Clinical Guidelines
Classification First: Understanding "Grade 4"
| Grade | Extent |
|---|---|
| 1st degree | Perineal skin and vaginal mucosa only |
| 2nd degree | Perineal muscles (not anal sphincter) |
| 3rd degree (a/b/c) | External anal sphincter (EAS) ± internal anal sphincter (IAS) |
| 4th degree | Full thickness through EAS + IAS + rectal mucosa |
| Grade | Extent |
|---|---|
| I | Contusion/haematoma |
| II | Superficial laceration (mucosa only) |
| III | Deep laceration (into fat/muscle) |
| IV | Laceration complex — into cervix or peritoneum |
| V | Injury into adjacent organs (bladder, urethra, rectum) |
A. 4th Degree Perineal Tear (RCOG GTG-29 / ACOG PB-198 / SOGC Guideline 457)
Immediate Principles
- Recognised as an obstetric anal sphincter injury (OASIS)
- Repair must be performed in a well-lit environment (operating theatre preferred)
- Regional or general anaesthesia is mandatory — adequate relaxation is essential for proper repair
- Repair should not be delayed beyond 8–12 hours if an experienced surgeon is not immediately available — studies show equivalent outcomes if repaired within this window (Berek & Novak's Gynecology)
Step-by-Step Surgical Repair (RCOG GTG-29 / ACOG PB-198)
Step 1 — Rectal Mucosa Repair
- The torn rectal mucosa must be repaired first
- Interrupted or continuous sutures using 3-0 polyglactin (Vicryl) or 3-0 chromic catgut
- Sutures placed through the submucosal layer only — do not penetrate the rectal lumen (to reduce infection risk)
- Alternatively, a continuous submucosal suture is acceptable
Step 2 — Internal Anal Sphincter (IAS) Repair
- The IAS is the pale, white smooth muscle layer between rectal mucosa and EAS
- Repair with interrupted or mattress sutures using 3-0 PDS (polydioxanone) or 2-0 Vicryl
- The IAS is often not separately identified or repaired — this is a common error; separate IAS repair improves continence outcomes
Step 3 — External Anal Sphincter (EAS) Repair
| Method | Technique |
|---|---|
| Overlap repair | The two ends of EAS are overlapped and secured with mattress sutures — preferred if ends are long enough |
| End-to-end (approximation) repair | Direct apposition of sphincter ends — used when muscle ends are short or retracted |
Step 4 — Vaginal Wall, Perineal Body, and Perineal Skin
- Perineal body (central tendon) reconstructed with interrupted sutures
- Vaginal mucosa closed with continuous unlocked 2-0 or 3-0 Vicryl
- Perineal skin — subcuticular suture preferred (less pain, fewer suture removal issues)
Postoperative Management (RCOG / ACOG / SOGC)
| Measure | Detail |
|---|---|
| Antibiotics | Single-dose IV cefuroxime + metronidazole intraoperatively (or oral prophylaxis for 5–7 days) — reduces wound infection and breakdown |
| Laxatives | Lactulose or Movicol (macrogol) — start immediately postoperatively; prevents constipation and straining at stool; continue for 10–14 days |
| Avoid enemas/suppositories acutely | Risk of disrupting repair |
| Analgesia | Regular NSAIDs + paracetamol; avoid constipating opioids where possible |
| Urinary catheter | Leave for minimum 24–48 hours (some centres 5 days) |
| Pelvic floor physiotherapy | Referral before discharge; commence pelvic floor exercises at 6 weeks |
| Follow-up | Clinic review at 6–12 weeks; assess wound healing, continence symptoms, sexual function |
| Endoanal ultrasound + anorectal manometry | If continence symptoms at follow-up — refer to urogynaecologist or colorectal surgeon |
Counselling for Future Pregnancies
- Women with previous OASIS should be counselled about mode of delivery
- Documented discussion in notes required (RCOG)
- Factors favouring elective caesarean section: persistent incontinence, manometry/USS defect, poor repair, patient preference
- No consensus on routine caesarean — individualise
B. AAST Grade IV Vaginal Laceration (Coital/Traumatic — into Cervix or Peritoneum)
Immediate Management
- Resuscitation first — IV access × 2, blood products, crossmatch, correct coagulopathy
- Examination under anaesthesia (EUA) in theatre — essential for adequate assessment
- Speculum examination — delineate extent; identify active bleeders
- Assess for peritoneal entry — if posterior fornix laceration extends into pouch of Douglas:
- Laparotomy / laparoscopy required to exclude visceral injury (bowel, bladder), haemoperitoneum, and to repair peritoneal defect
- Vaginal repair — layered closure:
- Deep layers: interrupted 0 Vicryl or PDS to achieve haemostasis
- Vaginal mucosa: continuous 2-0 Vicryl
- Haemostasis adjuncts if needed:
- Vaginal packing (temporary tamponade)
- Uterine/internal iliac artery embolisation (interventional radiology) for uncontrolled haemorrhage
- Internal iliac artery ligation (surgical last resort)
- Antibiotics — broad-spectrum cover (e.g., co-amoxiclav or cephalosporin + metronidazole)
- If vault dehiscence (post-hysterectomy) with eviseration — urgent laparotomy, reduce and repair vault with interrupted non-absorbable sutures
Key Points
- Diverting colostomy indicated if rectal injury accompanies vaginal injury — to protect repair and prevent faecal contamination (Schwartz's Principles of Surgery)
- Delayed repair (48–72 h) acceptable in haemodynamically unstable patients — damage control → stabilise → definitive repair
Explain the below with every possible outcomes and prognosis. AAST Grade IV Vaginal Laceration (Coital/Traumatic — into Cervix or Peritoneum) This is a surgical emergency and differs fundamentally from obstetric tears. Immediate Management Resuscitation first — IV access × 2, blood products, crossmatch, correct coagulopathy Examination under anaesthesia (EUA) in theatre — essential for adequate assessment. Speculum examination — delineate extent; identify active bleeders Assess for peritoneal entry — if posterior fornix laceration extends into pouch of Douglas: Laparotomy / laparoscopy required to exclude visceral injury (bowel, bladder), haemoperitoneum, and to repair peritoneal defect. Vaginal repair — layered closure: Deep layers: interrupted 0 Vicryl or PDS to achieve haemostasis Vaginal mucosa: continuous 2-0 Vicryl Haemostasis adjuncts if needed: Vaginal packing (temporary tamponade) Uterine/internal iliac artery embolisation (interventional radiology) for uncontrolled haemorrhage. Internal iliac artery ligation (surgical last resort)
coital vaginal laceration outcomes complications prognosis
vaginal laceration sexual intercourse treatment outcome
PMID: 34574671
pelvic haemorrhage internal iliac ligation embolisation outcome
AAST Grade IV Vaginal Laceration (Coital/Traumatic) — Full Outcomes & Prognosis
Overview of the Clinical Spectrum
- Haemorrhagic shock from arterial/venous pelvic bleeding
- Haemoperitoneum or pneumoperitoneum from peritoneal breach
- Potential visceral injury to bowel, bladder, or ureter
Stage 1 — Resuscitation
What Is Done
- IV access × 2 (large bore, antecubital)
- Blood products: packed red cells, fresh frozen plasma (FFP), platelets in 1:1:1 ratio (massive transfusion protocol)
- Crossmatch, FBC, coagulation screen, U&E, LFTs, group & save
- Correct coagulopathy — FFP, cryoprecipitate, TXA (tranexamic acid) if within 3 hours of injury
- Urinary catheter — monitor output (target >0.5 mL/kg/hr)
Possible Outcomes at This Stage
| Scenario | Outcome |
|---|---|
| Prompt resuscitation, haemodynamically stable | Patient proceeds safely to EUA; optimal surgical outcome likely |
| Delayed presentation (>2–4 hours) | Progressive coagulopathy, hypothermia, acidosis — lethal triad of trauma |
| Failure to achieve haemostasis with resuscitation alone | Requires damage control surgery — morbidity rises significantly |
| Massive transfusion (>10 units pRBC in 24h) | Risk of transfusion-related acute lung injury (TRALI), TACO (transfusion-associated circulatory overload), hyperkalaemia, hypocalcaemia, dilutional coagulopathy |
| TXA given within 3 hours | Reduces mortality from haemorrhage by ~15% (CRASH-2 trial data) |
| Irreversible haemorrhagic shock before theatre | Cardiac arrest, death — rare if hospital reached promptly |
Prognostic Determinants
- Systolic BP on arrival: <70 mmHg = high-risk; >90 mmHg = favourable
- Lactate / base excess: lactate >4 mmol/L or BE worse than –6 = severe shock
- Time from injury to theatre: the single most important factor
Stage 2 — Examination Under Anaesthesia (EUA)
What Is Done
- Lithotomy position, good lighting, theatre environment
- Speculum examination with suction to delineate the full extent of the laceration
- Assessment of: depth, direction (anterior/posterior/lateral), involvement of fornix, cervix, vault
Possible Outcomes at This Stage
| Finding | Implication |
|---|---|
| Isolated deep vaginal laceration (no peritoneal breach) | Can be repaired vaginally — excellent prognosis |
| Posterior fornix laceration extending into pouch of Douglas | Peritoneal entry confirmed — laparoscopy/laparotomy mandatory |
| Active arterial spurting vessel identified | Suture ligation or diathermy at EUA — may resolve haemorrhage completely |
| Haematoma in broad ligament / paravaginal space | Risk of expansion and late haemorrhage; may need drainage and packing |
| Cervical laceration (lateral fornix) | Proximity to uterine artery at 3/9 o'clock — high-volume arterial bleeding likely |
| EUA inadequate (obese patient, uncooperative, poor view) | Underestimation of injury — risk of missed peritoneal entry or visceral damage |
Stage 3 — Vaginal Repair (Layered Closure)
What Is Done
- Deep layers: interrupted 0 Vicryl/PDS — achieves haemostasis, obliterates dead space
- Vaginal mucosa: continuous 2-0 Vicryl — restores epithelial integrity
Possible Outcomes
Favourable
- Complete haemostasis — bleeding stops; no further intervention needed
- Normal healing over 4–6 weeks; full mucosal re-epithelialisation
- Return to sexual function in 6–8 weeks if repair uncomplicated
Complications of Vaginal Repair
| Complication | Timeframe | Details |
|---|---|---|
| Wound breakdown / dehiscence | Days 3–7 | Infection, poor tissue quality, tension on sutures; more common in atrophic/post-radiation tissue |
| Haematoma formation | Hours to days | Dead space not adequately closed; may expand and become infected; requires drainage |
| Infection / abscess | Days 5–14 | Bacterial contamination especially if bowel injured; presents as fever, purulent discharge, pelvic pain |
| Rectovaginal fistula | Weeks to months | If rectal wall involved but not recognised; presents as passing flatus/stool PV; requires staged surgical repair |
| Vesicovaginal fistula | Weeks | If bladder involved or suture placed through bladder; presents as continuous urinary incontinence |
| Vaginal stenosis | Months | Excessive fibrosis/scarring, especially if large area of mucosa lost; causes dyspareunia and difficulty with intercourse |
| Dyspareunia (painful intercourse) | Weeks to permanent | Scar tissue at repair site; more common with posterior fornix involvement; may require vaginal dilators or surgical revision |
| Psychological sequelae | Immediate to long-term | PTSD, sexual aversion, relationship difficulties — especially after assault; requires psychological support |
Long-term Prognosis of Uncomplicated Repair
- Good to excellent in young, otherwise healthy women
- Atrophic/postmenopausal tissue: higher complication rate — topical oestrogen aids healing pre- and post-operatively
- Post-hysterectomy vault: vault dehiscence repairs have higher re-dehiscence risk (~5–10%)
Stage 4 — Laparotomy / Laparoscopy for Peritoneal Entry
What Is Found and What Happens
A. Haemoperitoneum Without Visceral Injury
- Peritoneal cavity irrigated, bleeding source identified and controlled
- Peritoneal defect repaired (vaginal wall sutured from above if needed)
- Prognosis: Excellent if haemostasis achieved and no visceral injury
B. Small Bowel Injury
- Most common visceral injury in posterior fornix perforation (small bowel lies in the pouch of Douglas)
- Primary repair if clean laceration, minimal contamination, healthy bowel
- Resection + anastomosis if devascularised segment or large injury
- Diverting ileostomy if contamination heavy, patient unstable, or immunocompromised
- Risk of: anastomotic leak (3–8%), intra-abdominal abscess, ileus, adhesions, future bowel obstruction
- Systematic review (Stabile et al., 2021, PMID 34574671): in 16 cases of postcoital vaginal perforation with evisceration (1980–2020) in women with no prior surgery, all occurred at the posterior fornix; majority required laparotomy; no mortality reported in cases reaching surgical care — confirming that prompt diagnosis is the key determinant of survival
C. Rectal / Sigmoid Injury
- Requires diverting colostomy (Hartmann's procedure or loop colostomy) + distal washout
- Definitive rectal repair delayed until infection controlled
- Colostomy reversal 3–6 months later (second surgery)
- Risk of: anastomotic leak, wound infection, colostomy complications, adhesions
- Prognosis: Guarded — longer hospital stay, two-stage surgery, colostomy-related morbidity
D. Bladder Injury
- Primary repair in two layers (mucosa + seromuscular)
- Urinary catheter drainage for 7–14 days
- Risk of: vesicovaginal fistula (1–3%), urinary infection, urethral stricture
- Prognosis: Good with prompt repair
E. Ureteric Injury
- Rare; occurs with lateral fornix/parametrial extension
- Requires urological expertise: ureteric stenting or ureteroneocystostomy
- Missed injury → urinoma, hydronephrosis, renal impairment
- Prognosis: Good if identified intraoperatively; Poor if delayed >72h (stricture, loss of renal function)
F. Evisceration (Bowel Prolapsing Through Vaginal Defect)
- Dramatic presentation; bowel is usually viable if no prolonged exposure
- Reduction + vaginal/peritoneal repair ± bowel resection
- Prognosis: Good if bowel viable (no ischaemia); mortality approaches 0% in reported surgical cases
Stage 5 — Haemostasis Adjuncts
A. Vaginal Packing (Tamponade)
| Outcome | Details |
|---|---|
| Successful tamponade | Buys time for resuscitation and definitive repair; removed after 24–48 hours |
| Failure | Bleeding continues around pack; must escalate to embolisation or ligation |
| Complication | Retained pack (must document and remove at set time); pressure necrosis of vaginal epithelium with prolonged packing |
B. Uterine / Internal Iliac Artery Embolisation (UAE/IAE)
| Outcome | Rate / Details |
|---|---|
| Technical success (angiographic occlusion) | 85–95% |
| Clinical success (haemostasis achieved, surgery avoided) | 70–90% |
| Failure requiring surgery | 10–20%; escalate to ligation or hysterectomy |
| Recurrent haemorrhage | 5–10%; can re-embolise |
| Uterine ischaemia / necrosis | Rare (<1%); presents as sepsis, pain, foul discharge |
| Fertility preservation | UAE largely preserves fertility — menstruation typically resumes in 3–6 months; successful subsequent pregnancies documented |
| Ovarian failure | Rare (<5%) if non-target embolisation of ovarian artery |
| Post-embolisation syndrome | Fever, pain, leukocytosis in 30–50%; self-limiting, managed conservatively |
| Contrast nephropathy | 1–5%; risk higher in pre-existing renal impairment |
| Access site haematoma | 2–5% at femoral puncture site |
C. Internal Iliac (Hypogastric) Artery Ligation — Surgical Last Resort
| Outcome | Rate / Details |
|---|---|
| Haemostasis success rate | 40–75% (less reliable than embolisation in trauma) |
| Failure requiring hysterectomy | 25–50% if ligation alone insufficient |
| Uterine / pelvic organ necrosis | Rare — rich collateral circulation protects |
| Buttock claudication | Rare; due to reduced gluteal artery perfusion |
| Bladder / ureter injury (during ligation) | 1–3%; dissection near ureter and bladder at pelvic sidewall |
| Nerve injury | Obturator or lumbosacral nerve injury possible |
| Fertility | Reduced compared to UAE — subsequent pregnancies less likely; uterine blood flow permanently reduced |
| Future embolisation possible | Yes — ligation does not preclude subsequent radiological intervention |
Stage 6 — If All Else Fails: Hysterectomy
- Emergency hysterectomy (total or subtotal) is life-saving
- Prognosis: Life-saving but permanent loss of fertility
- Morbidity: haemorrhage, adjacent organ injury, adhesions
- Psychological impact of infertility — especially in young nulliparous patients; requires counselling
Overall Prognosis Summary
| Scenario | Prognosis |
|---|---|
| Isolated deep vaginal laceration, no peritoneal entry, haemostasis at EUA | Excellent — near-complete recovery |
| Peritoneal entry, small bowel injury, repaired within hours | Very good — mortality near zero with surgical care |
| Posterior fornix perforation with evisceration, bowel viable | Good — all 16 literature cases survived with surgery (Stabile et al., 2021) |
| Rectal injury requiring colostomy | Good but prolonged — 2-stage surgery, months of recovery |
| Bladder injury, repaired promptly | Good — low fistula risk |
| Ureteric injury, missed >72h | Guarded — risk of renal function loss |
| Massive haemorrhage, UAE/ligation successful | Good — fertility potentially preserved with UAE |
| Uncontrolled haemorrhage requiring hysterectomy | Survival good; permanent fertility loss |
| Delayed presentation (>6–12 hours) with peritonitis | Guarded to poor — septic shock, multi-organ dysfunction, ICU admission |
| Haemorrhagic shock with cardiac arrest before theatre | Poor — mortality high |
Key Prognostic Message
"Post-coital vaginal perforation and evisceration… is usually not a life-threatening condition, but a delay in diagnosis can lead to severe complications." — Stabile et al., 2021 (Systematic Review, PMID 34574671)