Cream to remove scar
Reading File
Finding Sources
Searching PubMed
"scar" AND "topical treatment" AND "silicone"
Searching the Web
best creams to remove or reduce scars evidence based 2025
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Here is a comprehensive, evidence-based guide to creams and topical treatments for scars:
Topical Treatments for Scars: What Works
Key Principle First
No topical product can fully remove a scar — scars are permanent structural changes in the dermis. However, many topical treatments can significantly reduce their appearance, flatten raised scars, improve color, and relieve symptoms like itching.
1. 🥇 Silicone Gel / Silicone Gel Sheeting — Best Evidence
This is the #1 recommended first-line topical treatment.
International clinical guidelines explicitly recommend silicone gels and sheets as the first-line prophylactic and treatment option for hypertrophic scars and keloids. (Bailey and Love's Surgery, 28th Ed.)
How it works:
- Hydrates the stratum corneum
- Reduces collagen synthesis by fibroblasts
- Normalizes static electricity across the scar surface
Products: Mederma Scar Gel (silicone-based), BioCorneum, Dermatix, Kelo-cote, ScarAway
Use: Apply 2× daily for at least 3–6 months on fully healed wounds (once epithelium is stable)
Best for: Hypertrophic scars, keloids, surgical scars, C-section scars, burn scars
2. Topical Corticosteroids — Strong Evidence for Raised Scars
Clobetasol propionate 0.05% cream under silicone dressing occlusion is an alternative to intralesional steroid injections, especially for needle-averse patients. (Dermatology, 5th Ed.)
Best for: Hypertrophic scars and keloids; helps flatten and reduce pruritus
Caution: Risk of skin atrophy, hypopigmentation (especially in darker skin tones) with prolonged use
3. Onion Extract Creams (e.g., Mederma classic formula)
Evidence is weak and conflicting.
- One pilot study found topical onion extract ineffective in improving erythema or pruritus compared to petrolatum-based ointment alone. (Dermatology 5th Ed.)
- A 2025 systematic review (PMID 38894613) concluded evidence for onion extract remains insufficient.
- Mechanism proposed: decreased inflammation and reduced fibroblast proliferation rate (Level 1 data is lacking)
Bottom line: Popular but not strongly supported by evidence. Silicone-based products are more effective.
4. Vitamin E (Tocopherol) Cream
Not recommended by most guidelines.
- Antioxidant properties theorized to help, but clinical trials have not shown significant benefit over placebo
- Some patients develop contact dermatitis from topical vitamin E
- Often included in OTC scar products but contributes little
5. Retinoid Creams (e.g., Tretinoin)
Useful mainly for atrophic/acne scars, not hypertrophic scars or keloids
- Promotes collagen remodeling and skin cell turnover
- Best combined with other treatments (microneedling, chemical peels) for acne scarring
- Requires prescription
Summary Table
| Product | Scar Type | Evidence | OTC? |
|---|---|---|---|
| Silicone gel/sheets | Hypertrophic, keloid, surgical | ✅ Strong | Yes |
| Clobetasol cream 0.05% | Hypertrophic, keloid | ✅ Good | Rx only |
| Onion extract (Mederma) | General | ⚠️ Weak | Yes |
| Vitamin E cream | General | ❌ Not supported | Yes |
| Tretinoin (retinoid) | Acne/atrophic scars | ✅ Moderate | Rx only |
When Topicals Aren't Enough
For keloids or stubborn hypertrophic scars, dermatologists combine topicals with:
- Intralesional triamcinolone injections (10–40 mg/mL every 4–6 weeks) — most effective for raised scars
- Pulsed dye laser therapy
- Cryotherapy
- Surgical revision (for misaligned or contracture scars)
Practical Tips
- Start treatment only after the wound is fully healed (epithelium intact)
- Use sun protection (SPF 30+) over any scar — UV exposure worsens discoloration
- Massage the scar daily to improve pliability
- Be patient — most topical treatments require 3–6 months of consistent use
Sources: Dermatology 2-Volume Set 5e; Bailey and Love's Short Practice of Surgery 28th Ed.; Current Surgical Therapy 14e. PubMed: PMID 38894613 (2025 systematic review on onion extract)
Burn scar
Finding Sources
Searching PubMed
"burn scar" AND "topical treatment"
Searching the Web
burn scar cream treatment evidence based 2024 2025
Finding Sources
Searching PubMed
"burn scar" AND "silicone" AND "compression"
Reading Web Page
https://academic.oup.com/jbcr/article/46/3/504/7901652
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
burn scar hypertrophic treatment silicone
Finding Sources
I now have comprehensive, well-sourced information. Let me compile the full answer with the treatment algorithm image.
Burn Scar: Creams & Full Management Guide
Burn scars — especially from deep partial- or full-thickness burns — are among the most challenging scars to treat. They almost always form hypertrophic scars: raised, red, tight, itchy, and prone to contracture. Management requires a stepwise, multimodal approach.
Why Burn Scars Are Different
After deep burns, there is increased inflammatory response, abnormal neovascularization, aberrant cytokine expression (particularly TGF-β), and excess collagen production. This creates thickened, inelastic scar tissue that can restrict joint movement and cause chronic pain and pruritus. (Schwartz's Principles of Surgery, 11th Ed.)
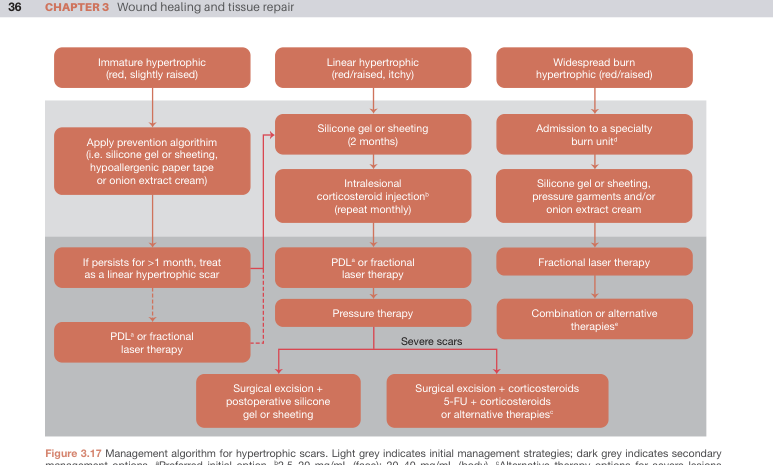
Treatment Algorithm for Burn Hypertrophic Scars
The management steps below follow this international algorithm:
Step 1 — Topical Treatments (First-Line, Home Use)
🥇 Silicone Gel / Silicone Gel Sheeting
The most evidence-supported topical for burn scars.
- Widely accepted as first-line prophylactic and treatment option for hypertrophic and keloid scars (Bailey & Love's Surgery, 28th Ed.)
- Works by increasing hydration of the stratum corneum, reducing collagen synthesis, and normalizing TGF-β signaling
- Applied 2× daily or worn as a sheet >12 hours/day for best effect
- Should extend slightly beyond the scar margins
- Minimum 3–6 months of consistent use required
Products: Kelo-cote, BioCorneum, Dermatix, ScarAway sheets, Mepiform
Real-world example:

Onion Extract Cream + Heparin + Allantoin (e.g., Contractubex)
- A combination cream studied specifically for postburn hypertrophic scars
- A comparison study (Burns, 2009) found silicone gel outperformed onion extract/heparin/allantoin for postburn scars, but the combination still showed some benefit
- Used as an adjunct option in burn units, especially for widespread hypertrophic scars when combined with pressure garments (Bailey & Love's, 28th Ed. algorithm)
- Onion extract decreases inflammation and fibroblast proliferation rate (Dermatology 5th Ed.)
Moisturizers / Emollients
- Burn skin loses its ability to produce natural oils; daily moisturizing is essential
- Reduces itching, improves pliability, and prevents cracking
- Use fragrance-free, thick creams (e.g., Vaseline, CeraVe, Eucerin)
- Apply multiple times daily, especially after bathing
Pirfenidone Topical Gel 8% (Emerging)
- Antifibrotic agent; inhibits fibroblast activity, collagen deposition, and lowers TGF-β
- A controlled trial in pediatric burn patients showed up to 67% reduction in Vancouver Scar Scale scores vs. pressure therapy alone
- Not yet widely available OTC; considered investigational
Step 2 — Sun Protection (Critical)
- Burn scars hyperpigment severely with UV exposure, permanently darkening the scar
- Apply SPF 50+ sunscreen daily to all healed burn scars
- Cover with clothing when possible for the first 2 years post-burn
Step 3 — Physical Measures (Combined with Topicals)
| Method | Purpose |
|---|---|
| Pressure garments | Worn >16 hrs/day; reduce scar blood supply, flatten hypertrophic scars |
| Massage | Breaks up collagen cross-links, improves pliability |
| Splinting/serial casting | Prevents and treats contractures across joints |
| Physiotherapy | Maintains range of motion, especially near joints |
(Current Surgical Therapy, 14th Ed.; Schwartz's Surgery, 11th Ed.)
Step 4 — Medical & Procedural (If Topicals Insufficient)
- Intralesional triamcinolone acetonide (10–40 mg/mL, every 4–6 weeks) — most effective for raised, firm scars; risk of atrophy
- Intralesional 5-FU + corticosteroids — for keloid-like scars, especially in darker skin to minimize hypopigmentation risk
- Pulsed Dye Laser (PDL) — targets hemoglobin; reduces erythema and pruritus
- Ablative CO₂ fractional laser — flattens scars, improves pliability, reduces neuropathic pain; typically started at 6–12 months post-burn, ~3 sessions (Schwartz's Surgery, 11th Ed.)
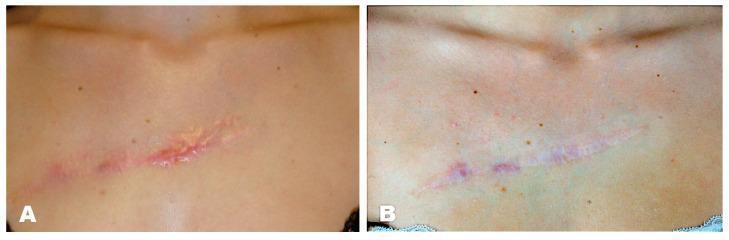
Before and after triamcinolone + silicone patch:
Step 5 — Surgery (Last Resort)
For contractures or severe functional restriction:
- Scar release + skin grafting (split or full thickness)
- Local/distant flap reconstruction
- Z-plasty or W-plasty for misaligned scars
Practical Summary
| Priority | Action |
|---|---|
| ✅ Start immediately (wound healed) | Moisturize heavily, sun protect SPF 50+ |
| ✅ Week 2–4 post-healing | Start silicone gel 2×/day + pressure garment |
| ✅ Ongoing 3–6 months | Continue silicone + massage + physio |
| ⚕️ If scar remains raised at 3 months | See dermatologist/burns clinic for steroid injection or laser |
| 🏥 Contracture limiting movement | Surgical referral |
Sources: Schwartz's Principles of Surgery 11e; Bailey & Love's Surgery 28e; Current Surgical Therapy 14e; Dermatology 5th Ed. (Dermatology 2-Volume Set). PMC11907609 (pirfenidone topical evidence, 2025).
This is a shared conversation. Sign in to Orris to start your own chat.