microcephaly
Reading File
Finding Sources
Searching PubMed
microcephaly etiology management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, well-sourced information. Here is a complete answer:
Microcephaly
Definition
Microcephaly is a condition in which the head circumference (HC) is 2-3 standard deviations below the mean for gestational age on standardized charts. Using a 2 SD cutoff, about 2% of the general population would meet criteria; at ≥3 SD below the mean, only ~0.1% qualify, and the vast majority of these have a significant disability.
- Microcephaly vera (primary hereditary form): head circumference < 45 cm in adult life, i.e., 5 SDs below the mean. Brain weight may be < 300 g (normal adult: 1,100-1,500 g).
- Creasy & Resnik's Maternal-Fetal Medicine, p. 408
Epidemiology
- Birth incidence: 1:6,250 to 1:8,500, rising to 1:625 by age 1 year (reflecting cases not diagnosed at birth).
- Higher incidence in populations with elevated consanguinity rates.
- In the United States, approximately 25,000 infants are diagnosed annually.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 408; Langman's Medical Embryology, p. 176
Pathogenesis
The core mechanism is reduced neurogenesis - a failure of neural progenitor cells to properly expand during development. The result is a smaller brain that does not exert sufficient pressure to drive neurocranial expansion. The skull bones are present and sutures are intact (distinguishing true microcephaly from craniosynostosis, where sutures close prematurely but the brain itself may be normal).
At the molecular level, mutations in microtubule spindle components are the most common cause of congenital primary microcephaly. Key genes include:
| Gene | Notes |
|---|---|
| ASPM | Abnormal spindle-like microcephaly-associated |
| WDR62 | Spindle pole protein |
| MCPH1 | DNA damage response |
| CDK5RAP2 | Centrosomal spindle regulation |
In primary autosomal recessive microcephaly (MCPH types 1-7), the brain is small but has no gross structural abnormality. Onset occurs during the second trimester.
- Langman's Medical Embryology; Harrison's Principles of Internal Medicine 22E; The Developing Human, p. 935
Causes / Etiology
Microcephaly is a common final pathway for many heterogeneous conditions:
Genetic
- Autosomal recessive primary microcephaly (MCPH1-MCPH7) - isolated, rare (1:30,000 to 1:250,000)
- Chromosomal anomalies: trisomy 13, 18, 21; 4p- (Wolf-Hirschhorn), 5p- (cri du chat)
- Syndromes: Cornelia de Lange, Fraser, Meckel, Smith-Lemli-Opitz, Williams, Miller-Dieker
- Associated brain malformations: holoprosencephaly, lissencephaly, agenesis of corpus callosum
Infections (TORCH + Zika)
- Zika virus - cytotoxic to neural progenitor cells; established cause of congenital microcephaly
- Cytomegalovirus (CMV)
- Rubella virus
- Toxoplasma gondii
- Herpes simplex virus
Metabolic / Toxic
- Phenylketonuria (PKU) - untreated maternal PKU is a major cause
- Maternal alcohol abuse (fetal alcohol syndrome)
- Hydantoin (phenytoin) exposure
- Poorly controlled maternal diabetes
Vascular / Structural
- Intrauterine ischemia / trauma
- Intracranial hemorrhage
- Porencephaly
- Creasy & Resnik's Maternal-Fetal Medicine, p. 408-409; The Developing Human, p. 935-936
Clinical Features
- Small calvaria with normal-sized face - anthropoid appearance at birth
- Narrow, receding forehead with flat occiput (in microcephaly vera)
- Severe intellectual disability / cognitive impairment
- Lack of communicative speech
- Lumbering gait; stature is moderately reduced
- Vision, hearing, and cutaneous sensation are generally spared
- Skull films: cranial sutures are present, with exaggerated convolutional markings on the inner table
- Some cases have associated cerebellar hypoplasia or infantile muscular atrophy
- Seizures are common in syndromic cases
- Adams and Victor's Principles of Neurology, 12th Ed.
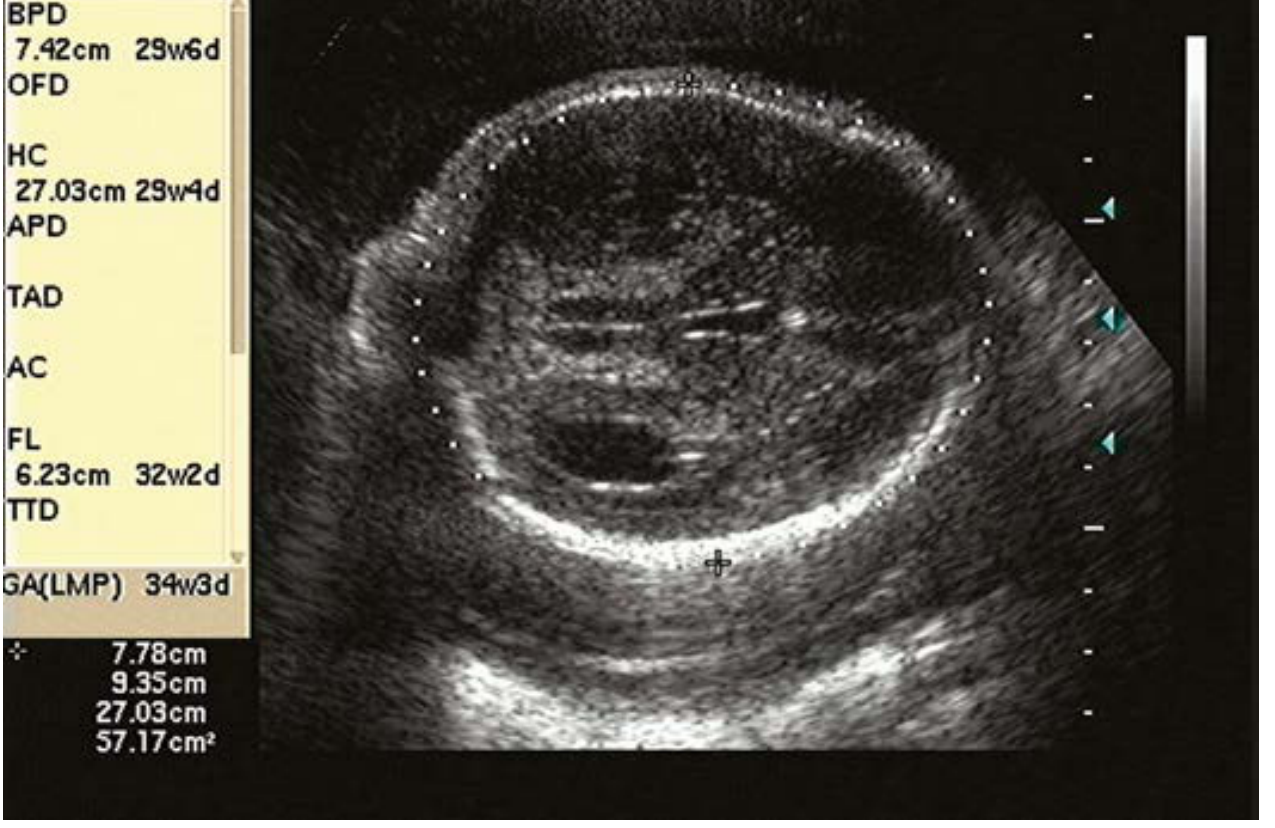
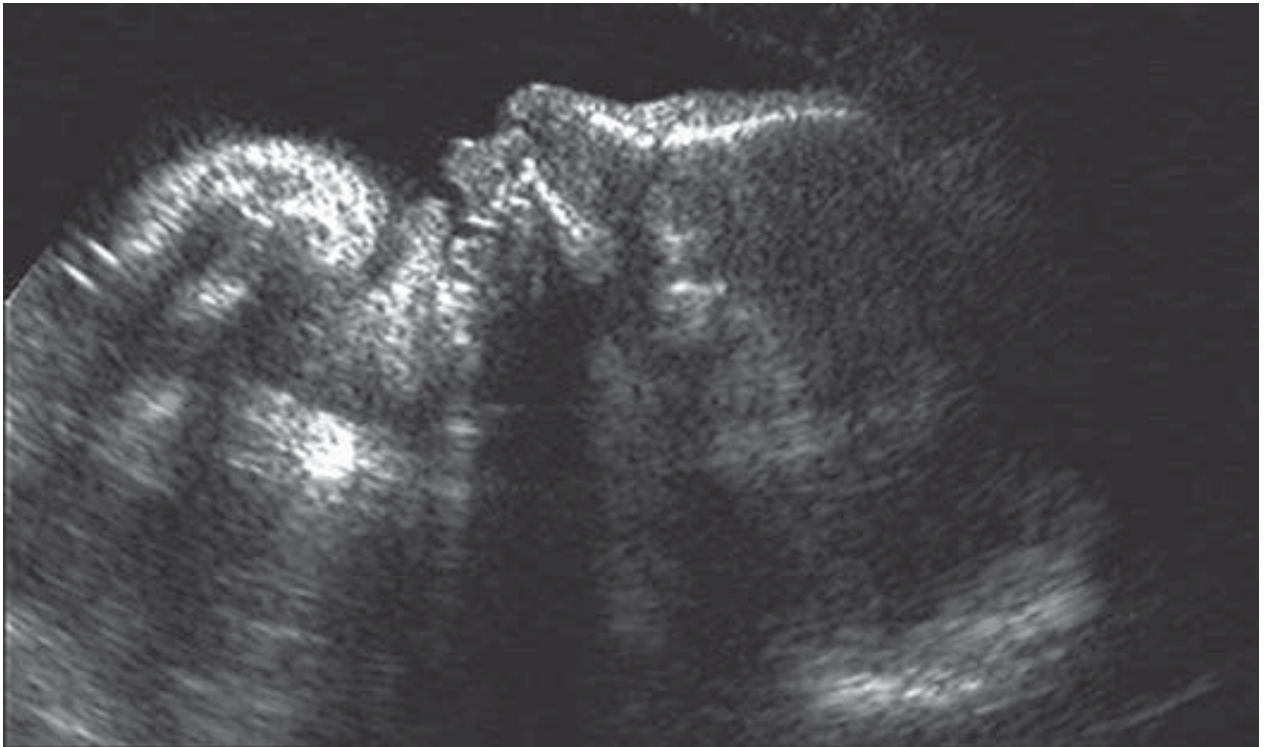
Prenatal Diagnosis (Imaging)
Microcephaly can be detected in utero by serial ultrasound. Key sonographic features include:
- HC > 3 SDs below the mean for gestational age
- Small biparietal diameter (BPD) and cerebellar diameter
- Sloping forehead (seen in profile)
- Reduced frontal lobe distance
- Ventriculomegaly
- Large subarachnoid space
- Brain appearing "small" for skull size
- Associated intracranial anomalies
Note: Abnormal HC may become apparent only late in pregnancy, so serial scans are important.
Ultrasound images from Creasy & Resnik's Maternal-Fetal Medicine:
Differential Diagnosis on Imaging
- Anencephaly
- Hydrocephalus (head is large, not small - key distinction)
- Brain atrophy
- Craniosynostosis (sutures fused, but brain normal)
Management
Antenatal
- Genetic counseling + karyotype, chromosomal microarray, or subtelomeric rearrangement analysis
- Chromosomal breakage studies
- TORCH titers + Zika virus IgM antibody testing (follow-up with PCR or PRNT if IgM positive)
- Screen for maternal PKU; consider screening for illicit drugs and alcohol
- Fetal echocardiography (associated cardiac anomalies)
- Fetal MRI to evaluate cortical abnormalities
- Pediatric neurology consultation
- Offer pregnancy termination counseling
- Serial scans for fetal growth
Obstetric
- Vaginal delivery is not contraindicated
- Cesarean section may be needed for other fetal anomalies, malposition, or maternal indications
- In severe cases, the small head may pass through the cervix before adequate dilation for the trunk
Neonatal
- Consultations: neurology, neonatology, genetics
- Repeat head ultrasound and/or MRI
- Serial head biometry to track growth
- Parental testing for carrier status in syndromic cases
- Creasy & Resnik's Maternal-Fetal Medicine, p. 408-409
Prognosis
Outcome depends heavily on the underlying etiology and severity:
- Primary (isolated) MCPH: severely impaired intellectual development; no gross brain structural anomaly but profound cognitive disability
- Syndromic / secondary microcephaly: prognosis varies by syndrome and associated anomalies
- Microcephaly vera: the most severe form - severe cognitive impairment, absent communicative speech, though sensory functions (vision, hearing, sensation) are preserved
- A milder form ("radial microbrain") exists where the sulcal pattern and neuronal arrangement are normal; the defect is simply a reduced number of neurons generated, and outcomes can be less severe
Key Points Summary
| Feature | Detail |
|---|---|
| Definition | HC ≥ 2 SD below mean for age |
| Mechanism | Reduced neurogenesis → insufficient brain growth → skull fails to expand |
| Key genes | ASPM, WDR62, MCPH1, CDK5RAP2 |
| Infections | Zika, CMV, Rubella, Toxoplasma |
| Toxins | Alcohol, phenytoin, maternal PKU |
| Prenatal detection | Serial ultrasound; HC ± 3 SD; sloping forehead |
| Management | Genetic workup, TORCH/Zika serology, MRI, neurology consult |
| Prognosis | Usually severe intellectual disability; sensory function preserved |
This is a shared conversation. Sign in to Orris to start your own chat.