Diabetes mellitus
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetes mellitus" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive, high-quality content from multiple authoritative textbooks. Here is the full, detailed overview of Diabetes Mellitus:
Diabetes Mellitus
Definition
Diabetes mellitus (DM) is a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both. The chronic hyperglycemia of diabetes is associated with long-term damage, dysfunction, and failure of various organs - especially the eyes, kidneys, nerves, heart, and blood vessels.
Classification (ADA)
The current ADA classification identifies four main clinical types:
| Type | Mechanism |
|---|---|
| Type 1 DM (T1DM) | Autoimmune beta cell destruction → absolute insulin deficiency |
| Type 2 DM (T2DM) | Progressive loss of beta cell secretion + insulin resistance (~90% of all cases) |
| Gestational DM (GDM) | Diabetes first recognized during pregnancy (not clearly overt prior to gestation) |
| Other specific types | Monogenic (MODY, neonatal), exocrine pancreas disease (cystic fibrosis), drug/chemical-induced (glucocorticoids, HIV therapy, post-transplant) |
The older terms IDDM and NIDDM (and juvenile-onset/adult-onset) are no longer used. Classification is now based on etiology rather than treatment. - Tietz Textbook of Laboratory Medicine, 7th Ed.
Type 1 Diabetes Mellitus
Epidemiology: Accounts for 5-10% of all diabetes. Peak incidence in childhood and adolescence; ~75% present before age 18, though onset can occur at any age.
Pathogenesis: T1DM is a chronic autoimmune disease. Destruction or damage to beta cells in the islets of Langerhans leads to absolute insulin deficiency. Markers of the immune process include:
- Islet cell autoantibodies
- Autoantibodies to insulin
- Autoantibodies to glutamic acid decarboxylase (GAD65)
- Autoantibodies to tyrosine phosphatase-related islet antigen 2 (IA-2)
More than 60 genetic loci are associated with T1DM susceptibility, many implicating immune system genes. Environmental triggers (particularly enteroviruses) are also under investigation. - Creasy & Resnik's Maternal-Fetal Medicine
Three Stages (Tietz Textbook):
- Stage 1: Normoglycemic but multiple islet autoantibodies present
- Stage 2: Dysglycemia (IFG and/or IGT) + multiple autoantibodies
- Stage 3: Clinical diabetes with symptoms
Presentation: Abrupt onset of polyuria, polydipsia, rapid weight loss; ~30% present with diabetic ketoacidosis (DKA). Absolute dependence on insulin to sustain life and prevent ketosis.
Type 2 Diabetes Mellitus
Epidemiology: The most common form (~90% of all cases). Onset is insidious with minimal early symptoms. Many patients have irreversible complications at the time of diagnosis.
Pathophysiology: Involves both peripheral insulin resistance and progressive beta cell failure:
- Obesity - especially visceral fat accumulation - is the most important modifiable risk factor
- Initially, beta cells hypersecrete to overcome resistance; over time beta cell mass is lost via apoptosis (glucotoxicity, lipotoxicity, cytokines, leptins)
- Genetic factors, aging, and sedentary lifestyle all contribute
- Guyton & Hall Textbook of Medical Physiology; Lippincott Illustrated Reviews: Pharmacology
Key concept - "Metabolic Syndrome": Obesity + insulin resistance often precede T2DM by years. The UKPDS 35 study demonstrated that glycemia correlates directly with both macrovascular and microvascular complications.
Diagnosis (ADA Criteria)
Any ONE of the following on two separate occasions (or once with classic symptoms):
| Criterion | Threshold |
|---|---|
| Fasting plasma glucose (FPG) | ≥126 mg/dL (7.0 mmol/L) |
| 2-hour plasma glucose (75 g OGTT) | ≥200 mg/dL (11.1 mmol/L) |
| HbA1c | ≥6.5% |
| Random plasma glucose + classic symptoms | ≥200 mg/dL (11.1 mmol/L) |
Prediabetes:
- Impaired Fasting Glucose (IFG): FPG 100-125 mg/dL
- Impaired Glucose Tolerance (IGT): 2-hr OGTT 140-199 mg/dL
- HbA1c 5.7-6.4%
The ADA recommends that two tests obtained at two separate visits should be abnormal to confirm diagnosis (except in the presence of classic hyperglycemic symptoms). - Bradley and Daroff's Neurology in Clinical Practice; Quick Compendium of Clinical Pathology
Symptoms and Presentation
Classic symptoms arise from hyperglycemia and catabolic state:
- Polyuria - osmotic diuresis from glucosuria
- Polydipsia - compensatory increased thirst
- Weight loss - urinary caloric loss, muscle protein catabolism
- Blurred vision - osmotic changes in lens water content (resolves with glycemic control)
- Fatigue and weakness
- Recurrent infections (vaginitis, fungal skin infections)
- Slow wound healing
The renal threshold for glucosuria is ~200 mg/dL (11.1 mmol/L). Above this, glucose spills into urine, causing osmotic diuresis and severe dehydration. - Guyton & Hall Textbook of Medical Physiology
Acute Complications
Diabetic Ketoacidosis (DKA)
- Primarily in T1DM (also possible in T2DM under stress)
- Absolute insulin deficiency → unrestrained lipolysis → ketone body formation (acetoacetate, beta-hydroxybutyrate)
- Results in metabolic acidosis with Kussmaul breathing, dehydration, and (if untreated) coma and death
- Compensatory mechanisms: hyperventilation (CO2 expiration), urinary excretion of keto acids
Hyperosmolar Hyperglycemic State (HHS)
- Primarily T2DM
- Extreme hyperglycemia without significant ketosis
- Severe dehydration and altered consciousness
Hypoglycemia
- Complication of insulin therapy or sulfonylureas
- The DCCT showed tight glycemic control in T1DM significantly reduces microvascular risk but greatly increases hypoglycemia risk
Chronic Complications
Chronic hyperglycemia causes progressive damage via vascular and neural mechanisms.
Microvascular Complications
| Complication | Description |
|---|---|
| Diabetic Retinopathy | Leading cause of blindness in working-age adults; annual eye exams essential |
| Diabetic Nephropathy | Leading cause of end-stage renal disease; earliest sign is microalbuminuria |
| Diabetic Neuropathy | Peripheral (distal symmetric polyneuropathy) + autonomic; loss of protective sensation in feet |
The DCCT (Type 1) and UKPDS (Type 2) both demonstrated that tight glycemic control significantly reduces microvascular complication risk. - Rosen's Emergency Medicine
Macrovascular Complications
- Atherosclerosis - coronary artery disease, stroke, peripheral arterial disease
- Risk of MI in T2DM patients equals that of non-diabetic patients with prior MI (Haffner study)
- Hypertension and dyslipidemia are major amplifiers
Other Complications
- Diabetic foot - neuropathy + peripheral ischemia → ulceration and gangrene
- Periodontal disease - more frequent in DM
- Dermatological - diabetic dermopathy (shin spots), necrobiosis lipoidica
- Autonomic dysfunction - impaired cardiovascular reflexes, gastroparesis, bladder dysfunction
Management
Glycemic Targets (General)
- HbA1c target: <7% for most non-pregnant adults
- Pre-conception: HbA1c <6.5% (ADA)
- Hypoglycemia threshold: <3.0 mmol/L (<54 mg/dL)
Type 1 DM Treatment
Goal: physiologic insulin replacement that mimics endogenous secretion.
Insulin preparations:
| Type | Onset | Peak | Duration |
|---|---|---|---|
| Rapid-acting (Aspart, Glulisine, Lispro) | <15 min | 0.5-1.5 h | 3-5 h |
| Short-acting Regular | 0.5-1 h | 2-3 h | 4-8 h |
| Inhaled human insulin | <15 min | 1-2 h | 3 h |
| Intermediate (NPH) | 2-4 h | 4-10 h | 10-16 h |
| Long-acting (Glargine, Detemir, Degludec) | 1-9 h | Flat | 20-42 h |
Delivery systems:
- Multiple Daily Injections (MDI) - basal-bolus regimen
- Continuous Subcutaneous Insulin Infusion (CSII) - insulin pump
- Sensor-augmented systems (pump + CGM)
- Automated Insulin Delivery (AID) - closed-loop "artificial pancreas"
Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
Type 2 DM Treatment Algorithm
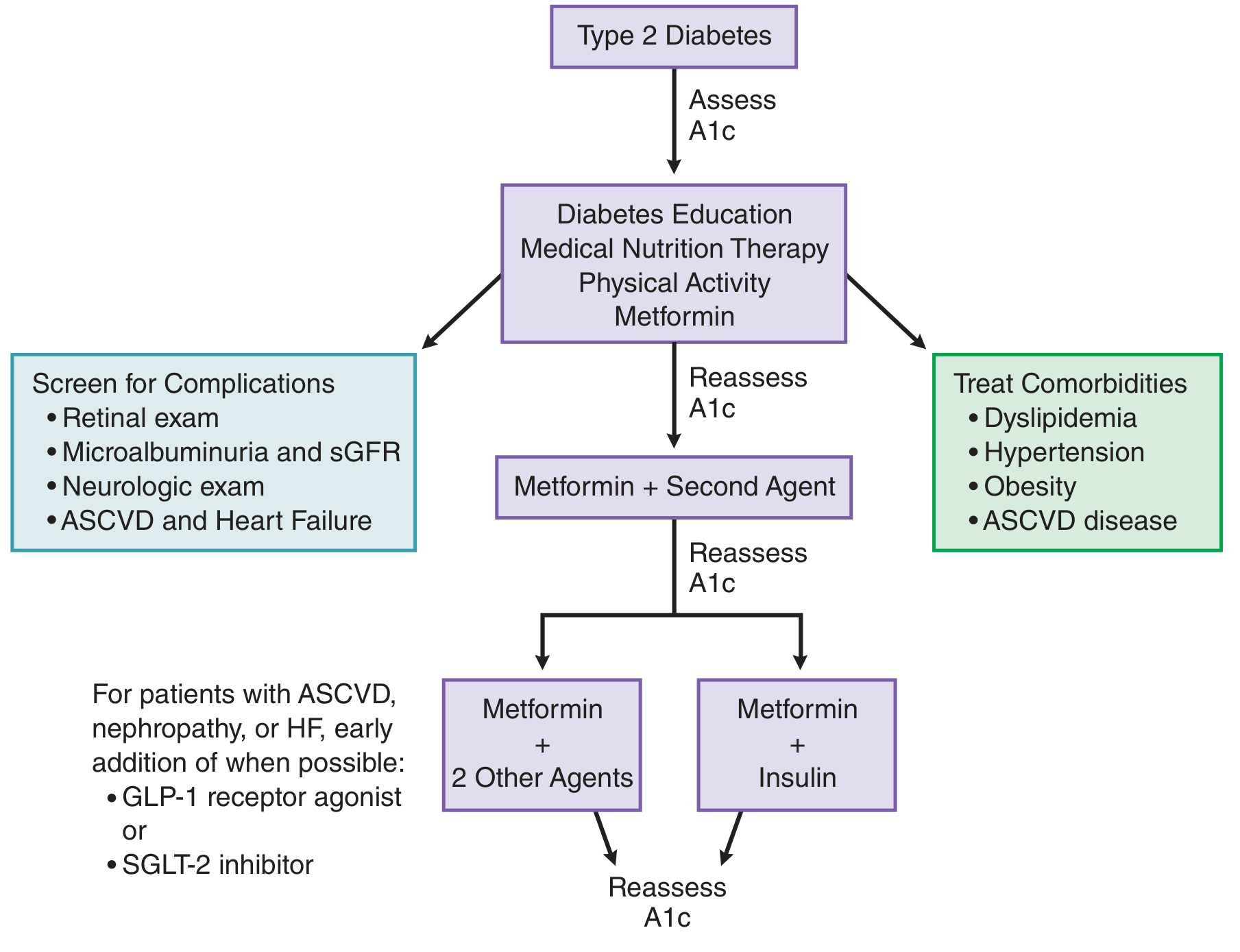
Step 1 - First line (all patients): Lifestyle modification (medical nutrition therapy, physical activity) + Metformin (initiated at diagnosis)
Step 2 - Add second agent if HbA1c target not met in 2-3 months:
- Sulfonylureas (glimepiride, glipizide)
- Thiazolidinediones (TZDs - pioglitazone)
- DPP-4 inhibitors (sitagliptin, saxagliptin)
- GLP-1 receptor agonists (semaglutide, liraglutide)
- SGLT-2 inhibitors (empagliflozin, dapagliflozin)
- Basal insulin
Special considerations:
- Established ASCVD - add GLP-1 RA or SGLT-2 inhibitor early
- Heart failure or diabetic nephropathy - SGLT-2 inhibitors are favored
- The GRADE study found liraglutide or basal insulin added to metformin gave slightly better glycemic control than glimepiride or sitagliptin
Step 3: Metformin + 2 other agents, or Metformin + insulin, with regular HbA1c reassessment
Goodman & Gilman's Pharmacological Basis of Therapeutics
Drug Class Summary
| Class | Mechanism | Key Agents |
|---|---|---|
| Biguanides | Reduces hepatic gluconeogenesis, improves insulin sensitivity | Metformin |
| Sulfonylureas | Stimulates insulin secretion from beta cells | Glimepiride, glipizide |
| TZDs | PPAR-γ agonist, improves insulin sensitivity | Pioglitazone |
| DPP-4 inhibitors | Inhibits incretin degradation, glucose-dependent insulin release | Sitagliptin |
| GLP-1 RAs | Mimics GLP-1: glucose-dependent insulin secretion, slows gastric emptying, weight loss, CV benefit | Semaglutide, liraglutide |
| SGLT-2 inhibitors | Blocks renal glucose reabsorption → glucosuria; CV and renal protection | Empagliflozin, dapagliflozin |
| Insulin | Replaces/supplements deficient insulin | Multiple preparations |
Monitoring
- HbA1c: Reflects average glycemia over ~3 months; check every 3 months until at goal, then every 6 months
- Self-monitoring blood glucose (SMBG) or Continuous glucose monitoring (CGM)
- Annual screening: Urine microalbuminuria, eGFR, dilated retinal exam, comprehensive foot exam
- Lipid panel and blood pressure at each visit
- Distal symmetric polyneuropathy screening: At diagnosis for T2DM; 5 years after diagnosis for T1DM
- Annual dental examination (increased periodontal disease risk)
Key Landmark Trials
| Trial | Finding |
|---|---|
| DCCT | Intensive glycemic control in T1DM reduces microvascular complications (retinopathy, nephropathy, neuropathy) but increases hypoglycemia risk |
| UKPDS 35 | Glycemia correlates directly with macro- and microvascular complications in T2DM |
| CARDS | Atorvastatin reduces cardiovascular events in T2DM |
| GRADE | Liraglutide/basal insulin superior to glimepiride/sitagliptin as add-ons to metformin for glycemic control |
Sources: Harrison's Principles of Internal Medicine, 22nd Ed. (2025) | Goodman & Gilman's Pharmacological Basis of Therapeutics | Guyton & Hall Textbook of Medical Physiology | Tietz Textbook of Laboratory Medicine, 7th Ed. | Lippincott Illustrated Reviews: Pharmacology | Creasy & Resnik's Maternal-Fetal Medicine | Rosen's Emergency Medicine | Robbins & Cotran Pathologic Basis of Disease
Create a quick reference guide PDF on diabetes diagnosis, monitoring, and management
Reading File
Running Command
ls /home/daytona/workspace/ 2>/dev/null && echo "exists" || mkdir -p /home/dayto…
Running Command
mkdir -p /home/daytona/workspace/diabetes-pdf && python3 -c "from reportlab.lib …
Writing File
~/diabetes-pdf/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import cm, mm
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_JUSTIFY
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.lib.colors import HexColor
import os
# ── Colour palette ──────────────────────────────────────────────────────────
NAVY = HexColor("#1B3A6B")
STEEL_BLUE = HexColor("#2E6DA4")
LIGHT_BLUE = HexColor("#D6E8F7")
TEAL = HexColor("#1B7A78")
LIGHT_TEAL = HexColor("#D4EFEE")
AMBER = HexColor("#E07B00")
AMBER_LIGHT= HexColor("#FFF3D6")
RED = HexColor("#C0392B")
RED_LIGHT = HexColor("#FDECEA")
GREEN = HexColor("#1E7E34")
GREEN_LIGHT= HexColor("#E4F5E9")
GREY_DARK = HexColor("#3D3D3D")
GREY_MID = HexColor("#6B6B6B")
GREY_LIGHT = HexColor("#F4F6F8")
WHITE = colors.white
OUTPUT = "/home/daytona/workspace/diabetes-pdf/Diabetes_Quick_Reference.pdf"
# ── Document ─────────────────────────────────────────────────────────────────
doc = SimpleDocTemplate(
OUTPUT, pagesize=A4,
leftMargin=1.5*cm, rightMargin=1.5*cm,
topMargin=1.8*cm, bottomMargin=1.8*cm,
title="Diabetes Mellitus – Quick Reference Guide",
author="Orris Medical"
)
W = A4[0] - 3*cm # usable width
styles = getSampleStyleSheet()
# Custom paragraph styles
def PS(name, **kw):
return ParagraphStyle(name, **kw)
title_style = PS("DocTitle",
fontName="Helvetica-Bold", fontSize=22, textColor=WHITE,
alignment=TA_CENTER, leading=26, spaceAfter=2)
subtitle_style = PS("DocSubtitle",
fontName="Helvetica", fontSize=11, textColor=HexColor("#C8DDEF"),
alignment=TA_CENTER, leading=14, spaceAfter=4)
section_header = PS("SectionHeader",
fontName="Helvetica-Bold", fontSize=11, textColor=WHITE,
leading=14, spaceAfter=2, spaceBefore=2,
leftIndent=4, rightIndent=4)
body = PS("Body",
fontName="Helvetica", fontSize=8.5, textColor=GREY_DARK,
leading=12, spaceAfter=3, spaceBefore=2)
body_small = PS("BodySmall",
fontName="Helvetica", fontSize=7.8, textColor=GREY_DARK,
leading=11, spaceAfter=2)
bold_body = PS("BoldBody",
fontName="Helvetica-Bold", fontSize=8.5, textColor=GREY_DARK,
leading=12, spaceAfter=2)
bullet_style = PS("Bullet",
fontName="Helvetica", fontSize=8.5, textColor=GREY_DARK,
leading=12, leftIndent=10, firstLineIndent=-7,
spaceAfter=2)
caption_style = PS("Caption",
fontName="Helvetica-Oblique", fontSize=7.5, textColor=GREY_MID,
alignment=TA_CENTER, leading=10)
note_style = PS("Note",
fontName="Helvetica-Oblique", fontSize=7.5, textColor=GREY_MID,
leading=10, spaceAfter=2)
# ── Helper functions ─────────────────────────────────────────────────────────
def section_box(title, bg=STEEL_BLUE):
"""Coloured section header bar."""
t = Table([[Paragraph(title, section_header)]], colWidths=[W])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("ROUNDEDCORNERS", [4]),
]))
return t
def note_box(text, bg=AMBER_LIGHT, border=AMBER):
"""Callout box."""
t = Table([[Paragraph(text, body_small)]], colWidths=[W])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("BOX", (0,0), (-1,-1), 1, border),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
]))
return t
def header_table(col_data, col_widths, header_bg=NAVY):
"""Table with a bold coloured header row."""
header_style = PS("TH", fontName="Helvetica-Bold", fontSize=8,
textColor=WHITE, leading=10, alignment=TA_LEFT)
cell_style = PS("TD", fontName="Helvetica", fontSize=8,
textColor=GREY_DARK, leading=11, alignment=TA_LEFT)
rows = []
for i, row in enumerate(col_data):
if i == 0:
rows.append([Paragraph(str(c), header_style) for c in row])
else:
rows.append([Paragraph(str(c), cell_style) for c in row])
t = Table(rows, colWidths=col_widths, repeatRows=1)
ts = TableStyle([
("BACKGROUND", (0,0), (-1,0), header_bg),
("ROWBACKGROUNDS",(0,1), (-1,-1), [WHITE, GREY_LIGHT]),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFCCD6")),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING", (0,0), (-1,-1), 6),
("VALIGN", (0,0), (-1,-1), "TOP"),
])
t.setStyle(ts)
return t
def bullet(txt):
return Paragraph(f"<bullet>\u2022</bullet> {txt}", bullet_style)
# ── Title Banner ──────────────────────────────────────────────────────────────
def make_title_banner():
banner = Table(
[[Paragraph("DIABETES MELLITUS", title_style)],
[Paragraph("Quick Reference Guide — Diagnosis · Monitoring · Management", subtitle_style)],
[Paragraph("Based on ADA Standards of Care | Harrison's 22e | Goodman & Gilman's | Guyton & Hall", caption_style)]],
colWidths=[W]
)
banner.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), NAVY),
("TOPPADDING", (0,0), (-1,-1), 12),
("BOTTOMPADDING", (0,0), (-1,-1), 10),
("LEFTPADDING", (0,0), (-1,-1), 12),
("RIGHTPADDING", (0,0), (-1,-1), 12),
("ROUNDEDCORNERS", [6]),
]))
return banner
# ─────────────────────────────────────────────────────────────────────────────
# BUILD CONTENT
# ─────────────────────────────────────────────────────────────────────────────
story = []
# ── TITLE ────────────────────────────────────────────────────────────────────
story.append(make_title_banner())
story.append(Spacer(1, 8))
# ═══════════════════════════════════════════════════════════════════════
# 1. CLASSIFICATION
# ═══════════════════════════════════════════════════════════════════════
story.append(section_box("1. CLASSIFICATION OF DIABETES MELLITUS", NAVY))
story.append(Spacer(1, 4))
class_data = [
["Type", "Mechanism / Aetiology", "Key Features"],
["Type 1 DM\n(T1DM)",
"Autoimmune beta-cell destruction → absolute insulin deficiency",
"5–10% of DM; abrupt onset; islet autoantibodies (GAD65, IA-2, IAA); ~30% present with DKA; peak incidence childhood/adolescence"],
["Type 2 DM\n(T2DM)",
"Progressive beta-cell secretory failure on background of insulin resistance",
"~90% of DM; insidious onset; linked to obesity, sedentary lifestyle, aging; many have complications at diagnosis"],
["Gestational DM\n(GDM)",
"Diabetes first recognised in pregnancy (not clearly pre-existing overt DM)",
"Screen all pregnant women 24–28 weeks; increased maternal/fetal risks; resolves post-partum (but ↑ future T2DM risk)"],
["Other Specific\nTypes",
"Monogenic (MODY, neonatal DM); exocrine pancreas disease (cystic fibrosis, pancreatitis); drug-induced (glucocorticoids, anti-retroviral therapy, post-transplant)",
"Consider in young, lean patients with family history or unusual clinical features; genetic testing may confirm"],
]
story.append(header_table(class_data, [2.5*cm, 6.5*cm, 8.5*cm]))
story.append(Spacer(1, 6))
# ═══════════════════════════════════════════════════════════════════════
# 2. DIAGNOSIS
# ═══════════════════════════════════════════════════════════════════════
story.append(section_box("2. DIAGNOSTIC CRITERIA (ADA)", STEEL_BLUE))
story.append(Spacer(1, 4))
# Diagnosis table – 2 column side by side
diag_data = [
["DIABETES (any ONE criterion, confirmed on 2 separate occasions unless classic symptoms present)",
"PREDIABETES (any ONE criterion)"],
["• Fasting Plasma Glucose (FPG) ≥ 126 mg/dL (7.0 mmol/L)\n"
" [fasting = no caloric intake ≥ 8 h]\n\n"
"• 2-hr Plasma Glucose (75 g OGTT) ≥ 200 mg/dL (11.1 mmol/L)\n\n"
"• HbA1c ≥ 6.5% (48 mmol/mol)\n\n"
"• Random Plasma Glucose ≥ 200 mg/dL WITH classic hyperglycaemic symptoms\n"
" (polyuria, polydipsia, unexplained weight loss)",
"• Impaired Fasting Glucose (IFG):\n FPG 100–125 mg/dL (5.6–6.9 mmol/L)\n\n"
"• Impaired Glucose Tolerance (IGT):\n 2-hr OGTT 140–199 mg/dL (7.8–11.0 mmol/L)\n\n"
"• HbA1c 5.7–6.4% (39–47 mmol/mol)\n\n"
" → Lifestyle intervention reduces progression\n"
" to T2DM by ~58% (DPP trial)\n"
" → Metformin may be offered (high-risk patients)"],
]
diag_ps = PS("DiagCell", fontName="Helvetica", fontSize=8, textColor=GREY_DARK, leading=12)
diag_hdr = PS("DiagHdr", fontName="Helvetica-Bold", fontSize=8, textColor=WHITE, leading=11, alignment=TA_CENTER)
diag_rows = [
[Paragraph(diag_data[0][0], diag_hdr), Paragraph(diag_data[0][1], diag_hdr)],
[Paragraph(diag_data[1][0], diag_ps), Paragraph(diag_data[1][1], diag_ps)],
]
diag_t = Table(diag_rows, colWidths=[W/2 - 2, W/2 - 2])
diag_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), STEEL_BLUE),
("BACKGROUND", (0,1), (0,1), LIGHT_BLUE),
("BACKGROUND", (1,1), (1,1), AMBER_LIGHT),
("BOX", (0,0), (-1,-1), 0.5, STEEL_BLUE),
("INNERGRID", (0,0), (-1,-1), 0.4, HexColor("#BFCCD6")),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 7),
("RIGHTPADDING", (0,0), (-1,-1), 7),
("VALIGN", (0,0), (-1,-1), "TOP"),
]))
story.append(diag_t)
story.append(Spacer(1, 4))
story.append(note_box(
"⚠ Renal glucose threshold ~200 mg/dL — glycosuria indicates established hyperglycaemia. "
"HbA1c is unreliable in haemolytic anaemia, haemoglobinopathies, recent blood transfusion, and pregnancy (use FPG/OGTT instead).",
bg=AMBER_LIGHT, border=AMBER))
story.append(Spacer(1, 6))
# ═══════════════════════════════════════════════════════════════════════
# 3. MONITORING
# ═══════════════════════════════════════════════════════════════════════
story.append(section_box("3. MONITORING", TEAL))
story.append(Spacer(1, 4))
mon_data = [
["Parameter", "Target / Frequency", "Notes"],
["HbA1c",
"< 7.0% (most adults)\n< 6.5% pre-conception\n> 8.0% in elderly/frail (relaxed)\nCheck every 3 months until at goal, then every 6 months",
"Reflects avg glycaemia over ~3 months; 1% reduction in HbA1c ≈ 14 mg/dL reduction in mean glucose"],
["Fasting Blood Glucose",
"80–130 mg/dL (4.4–7.2 mmol/L)\nSelf-monitor: frequency per clinical need",
"Key for basal insulin titration; morning fasting level reflects overnight hepatic glucose output"],
["Post-prandial Glucose",
"< 180 mg/dL (10.0 mmol/L)\n1–2 h after meal start",
"Target for post-meal bolus insulin dosing and GLP-1 RA assessment"],
["Continuous Glucose\nMonitoring (CGM)",
"Time-In-Range (TIR) > 70%\n(70–180 mg/dL)\nTime Below Range < 4%\n(< 70 mg/dL)",
"Preferred for T1DM; increasingly used in T2DM on insulin; reduces HbA1c and hypoglycaemia"],
["Urine Albumin/\nCreatinine Ratio (UACR)",
"Normal: < 30 mg/g\nMicro: 30–300 mg/g\nMacro: > 300 mg/g\nAnnually from diagnosis (T2DM); after 5 yrs (T1DM)",
"Earliest marker of diabetic nephropathy; ACEi/ARB indicated if UACR ≥ 30 mg/g"],
["eGFR",
"At diagnosis then annually;\nReduce SGLT-2i if eGFR < 45 mL/min;\nAvoid metformin if eGFR < 30 mL/min",
"Stage CKD and adjust drug therapy accordingly"],
["Blood Pressure",
"Target: < 130/80 mmHg\nEvery visit",
"BP control as important as glycaemia for CV/renal outcomes; ACEi/ARB first-line if DM + HTN"],
["Lipids",
"LDL-C < 100 mg/dL (high risk)\nLDL-C < 70 mg/dL (ASCVD present)\nAnnually",
"Statin therapy for all DM patients > 40 yrs or with CV risk factors (CARDS trial)"],
["Dilated Retinal Exam",
"At diagnosis (T2DM)\n5 years after diagnosis (T1DM)\nThen annually if normal; more frequently if retinopathy present",
"Diabetic retinopathy is leading cause of blindness in working-age adults"],
["Comprehensive Foot Exam",
"Annually\n(visual inspection each visit for high-risk feet)",
"Assess: pedal pulses, 10-g monofilament, 128-Hz tuning fork (great toe), ankle reflexes, nail care, deformities"],
["Dental Exam",
"Every 6 months",
"Periodontal disease more frequent in DM; bidirectional relationship with glycaemic control"],
["Weight / BMI",
"Every visit",
"5–10% weight loss improves insulin sensitivity significantly; weight loss drugs/surgery if BMI ≥ 30 kg/m²"],
]
story.append(header_table(mon_data, [3.5*cm, 5.5*cm, 8.5*cm], TEAL))
story.append(Spacer(1, 6))
# ═══════════════════════════════════════════════════════════════════════
# 4. MANAGEMENT — LIFESTYLE
# ═══════════════════════════════════════════════════════════════════════
story.append(section_box("4a. MANAGEMENT — LIFESTYLE MODIFICATIONS", STEEL_BLUE))
story.append(Spacer(1, 4))
life_data = [
["Domain", "Recommendation"],
["Medical Nutrition\nTherapy (MNT)",
"No single 'DM diet'; individualised with registered dietitian. Reduce refined carbohydrates, added sugars, saturated fats. "
"Mediterranean, DASH, or low-carb patterns all acceptable. Consistent carbohydrate intake helps insulin timing. "
"Caloric restriction (500–750 kcal/day deficit) for overweight/obese patients."],
["Physical Activity",
"≥ 150 min/week moderate aerobic exercise (e.g. brisk walking) OR ≥ 75 min/week vigorous activity. "
"Resistance training ≥ 2 days/week. Break prolonged sitting every 30 minutes. "
"Exercise improves insulin sensitivity, lowers HbA1c by ~0.6–0.7%, and reduces CV risk."],
["Weight Management",
"5–10% weight loss significantly improves glycaemia, BP, and lipids. "
"> 15% weight loss may induce T2DM remission (DiRECT trial). "
"GLP-1 RAs (semaglutide) and SGLT-2 inhibitors provide additional weight reduction. "
"Bariatric surgery for BMI ≥ 35 kg/m² with inadequate glycaemic control."],
["Smoking Cessation",
"Smoking doubles CV risk in DM. Cessation is one of the highest-yield interventions. "
"Offer pharmacotherapy + behavioural support."],
["Alcohol",
"Moderate intake only (≤ 1 drink/day women, ≤ 2 drinks/day men). "
"Alcohol can cause delayed hypoglycaemia (inhibits gluconeogenesis) — consume with food; avoid on empty stomach."],
["Sleep",
"Poor sleep impairs insulin sensitivity and glucose regulation. "
"Screen for obstructive sleep apnoea (OSA) — prevalence > 50% in T2DM. "
"CPAP treatment may improve glycaemic control."],
]
story.append(header_table(life_data, [3.5*cm, 14*cm], STEEL_BLUE))
story.append(Spacer(1, 6))
# ═══════════════════════════════════════════════════════════════════════
# 5. PHARMACOTHERAPY — T2DM
# ═══════════════════════════════════════════════════════════════════════
story.append(section_box("4b. PHARMACOTHERAPY — TYPE 2 DM", NAVY))
story.append(Spacer(1, 4))
# Treatment algorithm as styled table
alg_header_ps = PS("AlgHdr", fontName="Helvetica-Bold", fontSize=8.5, textColor=WHITE, leading=12, alignment=TA_CENTER)
alg_cell_ps = PS("AlgCell", fontName="Helvetica", fontSize=8, textColor=GREY_DARK, leading=11)
alg_note_ps = PS("AlgNote", fontName="Helvetica-Oblique", fontSize=7.5, textColor=GREY_MID, leading=10, alignment=TA_CENTER)
alg_data = [
["STEP 1", "STEP 2", "STEP 3"],
["Lifestyle + Metformin\n(start at diagnosis)\n\nReassess HbA1c in 2–3 months",
"Add 2nd agent if HbA1c target not met:\n• Sulfonylurea\n• TZD (pioglitazone)\n• DPP-4 inhibitor\n• GLP-1 RA ★\n• SGLT-2 inhibitor ★\n• Basal insulin",
"Metformin + 2 other agents\nOR\nMetformin + insulin\n\nReassess HbA1c every 3 months"],
["",
"★ For ASCVD: add GLP-1 RA or SGLT-2i early\n★ For HF/nephropathy: SGLT-2 inhibitor preferred",
""],
]
alg_rows = [
[Paragraph(c, alg_header_ps) for c in alg_data[0]],
[Paragraph(c, alg_cell_ps) for c in alg_data[1]],
[Paragraph(c, alg_note_ps) for c in alg_data[2]],
]
alg_t = Table(alg_rows, colWidths=[W/3 - 1, W/3 + 2, W/3 - 1])
alg_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), NAVY),
("BACKGROUND", (0,1), (0,1), LIGHT_BLUE),
("BACKGROUND", (1,1), (1,1), LIGHT_TEAL),
("BACKGROUND", (2,1), (2,1), LIGHT_BLUE),
("BACKGROUND", (0,2), (-1,2), GREY_LIGHT),
("BOX", (0,0), (-1,-1), 0.6, NAVY),
("INNERGRID", (0,0), (-1,-1), 0.4, HexColor("#BFCCD6")),
("TOPPADDING", (0,0), (-1,-1), 7),
("BOTTOMPADDING", (0,0), (-1,-1), 7),
("LEFTPADDING", (0,0), (-1,-1), 7),
("RIGHTPADDING", (0,0), (-1,-1), 7),
("VALIGN", (0,0), (-1,-1), "TOP"),
("ALIGN", (0,0), (-1,0), "CENTER"),
]))
story.append(alg_t)
story.append(Spacer(1, 5))
# Drug class table
drug_data = [
["Drug Class", "Key Agents", "Mechanism", "HbA1c ↓", "Advantages", "Cautions / Side Effects"],
["Biguanides\n(First-line)", "Metformin", "↓ Hepatic gluconeogenesis;\n↑ insulin sensitivity", "1–2%",
"Weight neutral; cheap;\ncardioprotective; reduces\nprogression from prediabetes",
"GI upset (start low, titrate);\nhold for contrast/surgery;\navoid if eGFR < 30; B12 deficiency"],
["Sulfonylureas", "Glimepiride\nGlipizide\nGliclazide", "Stimulates beta-cell\ninsulin secretion\n(closes K-ATP channels)", "1–2%",
"Effective; oral; cheap",
"Hypoglycaemia; weight gain;\navoiding in elderly and\nrenal impairment"],
["TZDs\n(PPAR-γ agonists)", "Pioglitazone", "↑ Insulin sensitivity\nin muscle, fat, liver", "0.5–1.4%",
"↓ TG, ↑ HDL; cardioprotective\nin some data (PROactive)",
"Weight gain; fluid retention;\ncontraindicated in HF;\n↑ fracture risk; bladder cancer risk"],
["DPP-4 Inhibitors\n(Gliptins)", "Sitagliptin\nSaxagliptin\nAlogliptin", "Inhibits DPP-4 →\n↑ active GLP-1 and GIP\n→ glucose-dependent\ninsulin secretion", "0.5–0.8%",
"Weight neutral;\nlow hypoglycaemia risk;\nrenal-dose adjustment available",
"Nasopharyngitis; do NOT\ncombine with GLP-1 RA;\nHF signal with saxagliptin"],
["GLP-1 Receptor\nAgonists", "Semaglutide\nLiraglutide\nDulaglutide\nExenatide", "Mimics GLP-1: ↑ glucose-\ndependent insulin secretion;\n↓ glucagon; slows gastric\nemptying; central satiety", "0.8–2.0%",
"↓ Weight (2–15 kg);\nCVOT benefit (LEADER,\nSUSTAIN-6);\nnephroprotective;\nnow available orally",
"GI: nausea, vomiting, diarrhoea\n(common, often transient);\ninjection (most); avoid in\npersonal/family hx MTC;\n↑ HR (liraglutide)"],
["SGLT-2 Inhibitors\n(Gliflozins)", "Empagliflozin\nDapagliflozin\nCanagliflozin", "Blocks SGLT-2 in PCT →\n↓ renal glucose reabsorption\n→ glucosuria (~70 g/day)", "0.6–1.2%",
"↓ Weight; ↓ BP;\nCVOT benefit (EMPA-REG);\n↓ HF hospitalisation;\nrenoprotective (CREDENCE)",
"Genital mycotic infections;\nDKA (rare, even in T2DM);\ndo NOT use if eGFR < 45;\nFourier's gangrene (rare)"],
["Insulin\n(all types)", "See insulin table\nbelow", "Replaces/supplements\ndeficient endogenous insulin", "1.5–3.5%\n(no ceiling)",
"Most effective at lowering\nglucose; no contraindication\nbased on renal/hepatic\nfunction; essential in T1DM",
"Hypoglycaemia; weight gain;\ninjection; requires monitoring;\ncost issues"],
]
story.append(Spacer(1, 4))
story.append(header_table(drug_data, [2.8*cm, 2.5*cm, 3.8*cm, 1.4*cm, 3.8*cm, 3.2*cm], NAVY))
story.append(Spacer(1, 6))
# ═══════════════════════════════════════════════════════════════════════
# 6. INSULIN
# ═══════════════════════════════════════════════════════════════════════
story.append(section_box("4c. INSULIN PREPARATIONS", TEAL))
story.append(Spacer(1, 4))
ins_data = [
["Type", "Examples", "Onset", "Peak", "Duration", "Clinical Use"],
["Rapid-acting\n(injected)", "Aspart, Lispro,\nGlulisine", "< 15 min", "0.5–1.5 h", "3–5 h", "Mealtime bolus; given just before meals"],
["Rapid-acting\n(inhaled)", "Afrezza\n(inhaled human)", "< 15 min", "1–2 h", "~3 h", "Pre-meal; not for smokers, lung disease"],
["Short-acting", "Regular\n(Humulin R, Actrapid)", "0.5–1 h", "2–3 h", "4–8 h", "IV drip (DKA); pre-meal if 30 min before"],
["Intermediate-acting", "NPH\n(Humulin N, Insulatard)", "2–4 h", "4–10 h", "10–16 h", "Twice-daily basal; less preferred (variable)"],
["Long-acting\nBasal", "Glargine U100\nDetemir", "2–4 h", "Minimal\npeak", "20–24 h", "Once-daily basal; T2DM basal therapy"],
["Ultra-long-acting\nBasal", "Degludec\nGlargine U300", "1–9 h", "Flat / no\npeak", "42 h (Degludec)\n> 24 h (U300)", "Once-daily; flexible timing; ↓ nocturnal hypo risk"],
["Pre-mixed", "70/30 NPH/Reg\nBiAspart 70/30", "Varies", "Dual", "Varies", "Twice-daily convenience; less flexible"],
]
story.append(header_table(ins_data, [2.5*cm, 3.5*cm, 1.8*cm, 2.2*cm, 2.5*cm, 5*cm], TEAL))
story.append(Spacer(1, 4))
story.append(note_box(
"Basal-Bolus Regimen: Long-acting insulin once daily (basal) + rapid-acting with each meal (bolus) — best mimics physiological insulin secretion. "
"Automated Insulin Delivery (AID / closed-loop systems): pump + CGM + algorithm — significantly improves TIR and reduces hypoglycaemia in T1DM.",
bg=LIGHT_TEAL, border=TEAL))
story.append(Spacer(1, 6))
# ═══════════════════════════════════════════════════════════════════════
# 7. ACUTE COMPLICATIONS
# ═══════════════════════════════════════════════════════════════════════
story.append(section_box("5. ACUTE COMPLICATIONS", RED))
story.append(Spacer(1, 4))
acute_data = [
["Complication", "Typical Patient", "Key Features", "Management Principles"],
["Diabetic Ketoacidosis\n(DKA)",
"T1DM (also T2DM\nunder physiological stress\nor SGLT-2i use)",
"Glucose > 250 mg/dL; pH < 7.3; bicarb < 18; ketones +++ "
"in blood/urine; Kussmaul breathing; fruity breath; "
"dehydration; altered consciousness in severe cases",
"IV fluids (0.9% NaCl); insulin infusion (0.1 U/kg/h); "
"K⁺ replacement (hold insulin if K⁺ < 3.5); "
"bicarbonate only if pH < 6.9; identify & treat precipitant"],
["Hyperosmolar Hyperglycaemic\nState (HHS)",
"Elderly T2DM;\noften dehydrated,\ninfected",
"Glucose > 600 mg/dL; plasma osmolality > 320 mOsm/kg; "
"minimal ketosis; pH normal; profound dehydration; "
"neurological signs (seizures, coma) common",
"Gradual fluid replacement (avoid too-rapid correction); "
"low-dose insulin; anticoagulation (DVT risk); "
"treat precipitant; correct Na⁺ carefully"],
["Hypoglycaemia",
"T1DM/T2DM on\ninsulin or sulfonylurea",
"< 70 mg/dL (mild-moderate); < 54 mg/dL (clinically significant); "
"symptoms: tremor, sweating, palpitations, confusion, seizure; "
"autonomic unawareness with recurrent episodes",
"Conscious: 15 g fast-acting carbohydrate (rule of 15); "
"unconscious: IM glucagon 1 mg or IV dextrose 50%; "
"review insulin/medication dose; consider CGM"],
]
story.append(header_table(acute_data, [3.5*cm, 3.5*cm, 5.5*cm, 5*cm], RED))
story.append(Spacer(1, 6))
# ═══════════════════════════════════════════════════════════════════════
# 8. CHRONIC COMPLICATIONS
# ═══════════════════════════════════════════════════════════════════════
story.append(section_box("6. CHRONIC COMPLICATIONS", NAVY))
story.append(Spacer(1, 4))
# Micro / Macro two-column
micro_hdr = PS("MicroHdr", fontName="Helvetica-Bold", fontSize=8.5, textColor=WHITE, leading=12, alignment=TA_CENTER)
micro_cell = PS("MicroCell", fontName="Helvetica", fontSize=8, textColor=GREY_DARK, leading=11)
comp_rows = [
[Paragraph("MICROVASCULAR COMPLICATIONS", micro_hdr), Paragraph("MACROVASCULAR COMPLICATIONS", micro_hdr)],
[
Paragraph(
"<b>Diabetic Retinopathy</b><br/>"
"• Leading cause of blindness in working-age adults<br/>"
"• Background → pre-proliferative → proliferative (neovascularisation)<br/>"
"• Also: diabetic macular oedema (DMO)<br/>"
"• Prevention: tight glycaemia + BP control<br/>"
"• Treatment: laser photocoagulation, intravitreal anti-VEGF<br/><br/>"
"<b>Diabetic Nephropathy (DKD)</b><br/>"
"• Leading cause of ESRD in developed countries<br/>"
"• Progression: microalbuminuria → macroalbuminuria → ↓ GFR → ESRD<br/>"
"• Prevention: HbA1c control, BP control (ACEi/ARB), SGLT-2i<br/>"
"• Screen UACR + eGFR annually<br/><br/>"
"<b>Diabetic Neuropathy</b><br/>"
"• Distal symmetric polyneuropathy (most common): numbness, tingling, burning feet; "
"loss of protective sensation (LOPS)<br/>"
"• Autonomic neuropathy: gastroparesis, erectile dysfunction, postural hypotension, "
"neurogenic bladder, abnormal cardiac reflexes<br/>"
"• Treatment: glycaemic control; duloxetine/pregabalin for pain; foot care",
micro_cell),
Paragraph(
"<b>Cardiovascular Disease (CVD)</b><br/>"
"• DM doubles CV risk; T2DM patients have equivalent MI risk to non-diabetics with prior MI<br/>"
"• Atherosclerosis: CAD, stroke, peripheral arterial disease (PAD)<br/>"
"• Management: statins, ACEi/ARB, antiplatelet (if indicated), GLP-1 RA / SGLT-2i<br/><br/>"
"<b>Diabetic Foot</b><br/>"
"• Triad: neuropathy + ischaemia + infection<br/>"
"• Annual foot exam: monofilament, tuning fork, pedal pulses, ankle reflexes<br/>"
"• Deformities: hammer toes, Charcot foot, callus formation<br/>"
"• Ulceration may lead to osteomyelitis and amputation<br/>"
"• Multidisciplinary foot team essential<br/><br/>"
"<b>Other</b><br/>"
"• Periodontal disease (bidirectional relationship with glycaemia)<br/>"
"• Dermatological: diabetic dermopathy ('shin spots'), necrobiosis lipoidica, "
"acanthosis nigricans<br/>"
"• Sexual dysfunction; urinary tract infections; non-alcoholic fatty liver disease (NAFLD)<br/>"
"• Cognitive impairment / dementia (↑ risk)",
micro_cell)
]
]
comp_t = Table(comp_rows, colWidths=[W/2 - 2, W/2 - 2])
comp_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), NAVY),
("BACKGROUND", (0,1), (0,1), LIGHT_BLUE),
("BACKGROUND", (1,1), (1,1), RED_LIGHT),
("BOX", (0,0), (-1,-1), 0.5, NAVY),
("INNERGRID", (0,0), (-1,-1), 0.5, HexColor("#BFCCD6")),
("TOPPADDING", (0,0), (-1,-1), 7),
("BOTTOMPADDING", (0,0), (-1,-1), 7),
("LEFTPADDING", (0,0), (-1,-1), 7),
("RIGHTPADDING", (0,0), (-1,-1), 7),
("VALIGN", (0,0), (-1,-1), "TOP"),
]))
story.append(comp_t)
story.append(Spacer(1, 4))
story.append(note_box(
"DCCT (T1DM): Intensive glycaemic control reduces retinopathy, nephropathy, and neuropathy risk significantly. "
"UKPDS 35 (T2DM): Each 1% reduction in HbA1c → 37% ↓ microvascular complications, 21% ↓ DM-related deaths. "
"EMPA-REG OUTCOME: Empagliflozin ↓ CV death by 38% and ↓ HF hospitalisation by 35% in T2DM with established CVD.",
bg=GREEN_LIGHT, border=GREEN))
story.append(Spacer(1, 6))
# ═══════════════════════════════════════════════════════════════════════
# 9. SPECIAL SITUATIONS
# ═══════════════════════════════════════════════════════════════════════
story.append(section_box("7. SPECIAL CLINICAL SITUATIONS", STEEL_BLUE))
story.append(Spacer(1, 4))
spec_data = [
["Situation", "Key Considerations"],
["Pregnancy (Pre-existing DM)",
"Target HbA1c < 6.5% (ideally < 6%) before conception. Tight control throughout; "
"insulin is the only approved agent; metformin/glyburide used in some guidelines for GDM but not preferred. "
"Risks: congenital anomalies, macrosomia, pre-eclampsia, perinatal mortality. "
"Close obstetric + diabetic team collaboration essential."],
["Gestational DM (GDM)",
"Screen all women 24–28 weeks (75 g OGTT). First-line: MNT + exercise. "
"If targets not met (FPG ≥ 95 / 1-hr ≥ 140 / 2-hr ≥ 120 mg/dL): insulin. "
"Postpartum: re-test at 6–12 weeks; lifetime screening for T2DM every 1–3 years."],
["Elderly Patients",
"Relax HbA1c target to 7.5–8.0% (or even 8.5% in frail/limited life expectancy). "
"Hypoglycaemia is particularly dangerous (falls, cognitive impairment, cardiac events). "
"Avoid complex regimens; prefer agents with low hypo risk (DPP-4i, SGLT-2i if tolerated). "
"Screen for cognitive impairment and depression annually."],
["Chronic Kidney Disease\n(CKD)",
"Metformin: avoid if eGFR < 30; reduce dose if eGFR 30–45. "
"SGLT-2 inhibitors: renoprotective (CREDENCE, DAPA-CKD); stop if eGFR < 20–25. "
"GLP-1 RAs: mostly safe (dose reduce exenatide if CKD stage ≥ 3). "
"Insulin dose reduction needed as eGFR falls (reduced insulin clearance)."],
["Heart Failure (HF)",
"SGLT-2 inhibitors are first-choice add-on (reduce HF hospitalisations regardless of EF). "
"Avoid TZDs (fluid retention, worsens HF). Avoid saxagliptin (↑ HF hospitalisation in SAVOR-TIMI). "
"Metformin: use with caution in decompensated HF; acceptable in stable HF."],
["Perioperative",
"Hold metformin on day of surgery (especially if contrast or major procedure). "
"Hold SGLT-2i at least 3–4 days pre-operatively (DKA risk). "
"Continue basal insulin at 75–80% of usual dose; hold rapid-acting while NBM. "
"Target glucose 140–180 mg/dL intra-operatively (tighter in cardiac surgery: 110–140)."],
["Sick Day Rules",
"Never stop insulin in T1DM even when not eating. "
"Monitor glucose every 2–4 h; check ketones if glucose > 250 mg/dL. "
"Maintain hydration with fluids containing carbohydrate if glucose < 200 mg/dL. "
"Seek medical attention if vomiting, ketones ++, glucose > 300, or altered consciousness."],
]
story.append(header_table(spec_data, [3.5*cm, 14*cm], STEEL_BLUE))
story.append(Spacer(1, 6))
# ═══════════════════════════════════════════════════════════════════════
# 10. GLYCAEMIC TARGETS SUMMARY BOX
# ═══════════════════════════════════════════════════════════════════════
story.append(section_box("8. GLYCAEMIC TARGETS AT A GLANCE", TEAL))
story.append(Spacer(1, 4))
tgt_data = [
["Measure", "General Adult", "Pre-Conception / Pregnancy", "Elderly / Frail", "Paediatric (T1DM)"],
["HbA1c", "< 7.0%", "< 6.5% (ideally < 6%)", "> 7.5–8.5%", "< 7.0%"],
["Fasting BG", "80–130\nmg/dL", "60–99 mg/dL", "90–150 mg/dL","90–130 mg/dL"],
["Post-prandial\n(1–2 hr)", "< 180 mg/dL", "< 120–140 mg/dL", "< 200 mg/dL", "< 180 mg/dL"],
["Time-In-Range\n(CGM, 70–180)", "> 70%", "> 70% (63% in preg.)", "> 50%", "> 70%"],
["Time Below Range\n(< 70 mg/dL)", "< 4%", "< 4%", "< 1%", "< 4%"],
["BP", "< 130/80 mmHg", "< 135/85 mmHg", "< 140/90 mmHg", "< 95th percentile"],
["LDL-C", "< 100 mg/dL\n(< 70 if ASCVD)", "Statins contraindicated in\npregnancy", "Individualise", "< 100 mg/dL\n(if risk factors)"],
]
story.append(header_table(tgt_data, [3.5*cm, 3.2*cm, 4.2*cm, 3.2*cm, 3.4*cm], TEAL))
story.append(Spacer(1, 6))
# ═══════════════════════════════════════════════════════════════════════
# 11. KEY LANDMARK TRIALS
# ═══════════════════════════════════════════════════════════════════════
story.append(section_box("9. KEY LANDMARK TRIALS", NAVY))
story.append(Spacer(1, 4))
trial_data = [
["Trial", "Year", "Population", "Key Finding"],
["DCCT", "1993", "T1DM", "Intensive glycaemic control ↓ retinopathy 76%, nephropathy 50%, neuropathy 60%; ↑ hypoglycaemia 3×"],
["UKPDS 33", "1998", "T2DM (new diagnosis)", "Intensive control ↓ microvascular complications by 25%; no significant ↓ in CV events"],
["UKPDS 35", "2000", "T2DM", "Each 1% ↓ in HbA1c → 37% ↓ microvascular complications, 21% ↓ DM-related deaths, 14% ↓ MI"],
["ACCORD", "2008", "T2DM + high CV risk", "Targeting HbA1c < 6% ↑ all-cause mortality — intensive arm stopped early; avoid over-treatment"],
["EMPA-REG OUTCOME", "2015", "T2DM + established CVD", "Empagliflozin ↓ CV death 38%, ↓ HF hospitalisation 35%, ↓ progression of nephropathy"],
["LEADER", "2016", "T2DM + high CV risk", "Liraglutide ↓ MACE 13%, ↓ CV death 22%, ↓ nephropathy progression"],
["CREDENCE", "2019", "T2DM + CKD (eGFR 30–90)", "Canagliflozin ↓ renal failure/CV death composite by 30%; stopped early due to benefit"],
["SUSTAIN-6", "2016", "T2DM + high CV risk", "Semaglutide ↓ MACE 26% vs placebo; ↑ diabetic retinopathy (rapid HbA1c ↓)"],
["DAPA-HF", "2019", "HFrEF (with/without DM)", "Dapagliflozin ↓ CV death/worsening HF by 26%; benefit in patients without DM too"],
["GRADE", "2022", "T2DM on metformin", "Liraglutide or basal insulin → slightly better glycaemic control vs glimepiride or sitagliptin as add-on"],
]
story.append(header_table(trial_data, [3.5*cm, 1.3*cm, 3.7*cm, 9*cm], NAVY))
story.append(Spacer(1, 6))
# ═══════════════════════════════════════════════════════════════════════
# FOOTER NOTE
# ═══════════════════════════════════════════════════════════════════════
story.append(HRFlowable(width=W, thickness=0.5, color=GREY_MID))
story.append(Spacer(1, 4))
story.append(Paragraph(
"<b>Sources:</b> Harrison's Principles of Internal Medicine 22e (2025) | Goodman & Gilman's Pharmacological Basis of Therapeutics | "
"Guyton & Hall Textbook of Medical Physiology | Tietz Textbook of Laboratory Medicine 7e | "
"Lippincott Illustrated Reviews: Pharmacology | Creasy & Resnik's Maternal-Fetal Medicine | Rosen's Emergency Medicine | "
"Robbins & Cotran Pathologic Basis of Disease | ADA Standards of Medical Care in Diabetes",
note_style))
story.append(Spacer(1, 2))
story.append(Paragraph(
"This document is a clinical quick-reference summary. Always verify drug doses and guidelines against current local formularies and institutional protocols. "
"Not a substitute for professional clinical judgement.",
note_style))
# ─────────────────────────────────────────────────────────────────────────────
# Build PDF
doc.build(story)
print(f"PDF created: {OUTPUT}")
Running Command
cd /home/daytona/workspace/diabetes-pdf && python3 generate_pdf.py 2>&1
Running Command
ls -lh /home/daytona/workspace/diabetes-pdf/Diabetes_Quick_Reference.pdf
Your quick reference guide is ready:
Diabetes Quick Reference
PDF Document · PDF
Here's what's included across 9 sections:
| Section | Contents |
|---|---|
| 1. Classification | T1DM, T2DM, GDM, other specific types with mechanisms and key features |
| 2. Diagnosis | ADA diagnostic criteria table (FPG, OGTT, HbA1c, random glucose) + prediabetes thresholds with caveats |
| 3. Monitoring | 10 parameters — HbA1c, CGM targets (TIR), UACR/eGFR, retinal exam, foot exam, BP, lipids, weight, with frequencies and targets |
| 4a. Lifestyle | Nutrition, exercise, weight management, smoking, alcohol, sleep — each with specific recommendations |
| 4b. Pharmacotherapy (T2DM) | Step 1-2-3 treatment algorithm + full drug class table (7 classes: mechanism, HbA1c reduction, advantages, cautions) |
| 4c. Insulin | All preparations with onset/peak/duration/clinical use; note on basal-bolus and AID systems |
| 5. Acute Complications | DKA, HHS, hypoglycaemia — features and management principles side by side |
| 6. Chronic Complications | Micro (retinopathy, nephropathy, neuropathy) vs macro (CVD, diabetic foot) in a two-column layout; key trial callout box |
| 7. Special Situations | Pregnancy, GDM, elderly, CKD, heart failure, perioperative, sick day rules |
| 8. Targets at a Glance | HbA1c, fasting BG, post-prandial, TIR, BP, LDL-C - across four patient groups |
| 9. Landmark Trials | 10 key trials (DCCT, UKPDS, EMPA-REG, LEADER, CREDENCE, GRADE, etc.) with year, population, and findings |
This is a shared conversation. Sign in to Orris to start your own chat.