Schwanomma histology diagram and key points pathology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content and images needed. Let me compile the comprehensive answer.
Schwannoma - Histology & Pathology
Histology Diagrams
From Robbins & Kumar Pathologic Basis of Disease (Cotran, Fig. 27.14):
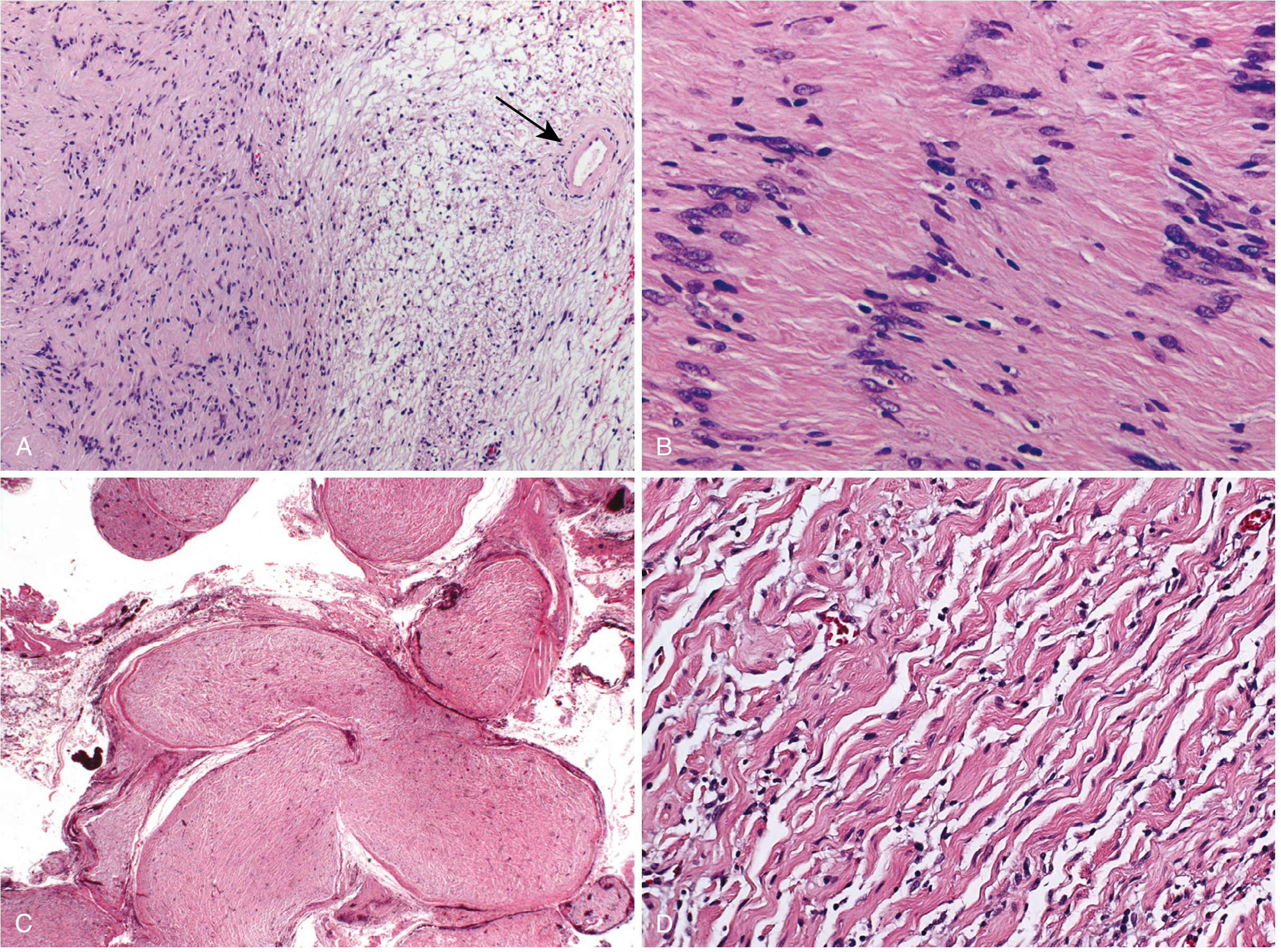
(A) Dense eosinophilic Antoni A area (left) vs loose pale Antoni B area (right), with hyalinized blood vessels (arrow). (B) High-power view of the Antoni A area showing nuclear palisading rows forming Verocay bodies (anuclear zones between palisading nuclei).
From Robbins & Kumar Basic Pathology (Fig. 20.6), with Verocay body highlighted:
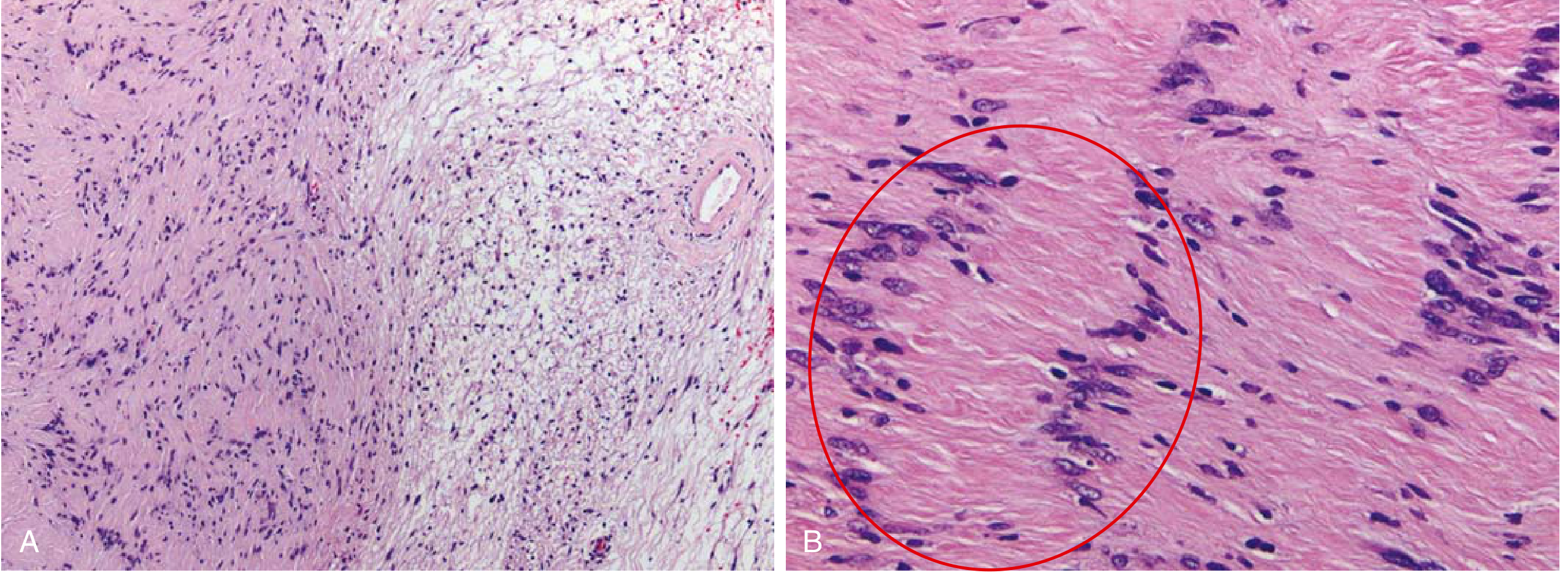
(A) Low-power: densely cellular Antoni A (left) + loose hypocellular Antoni B (right) + hyalinized vessels. (B) Circled area = a single Verocay body - two palisading rows of nuclei flanking a nuclear-free zone.
From Fitzpatrick's Dermatology (Fig. 121-22B) - Verocay bodies in focus:
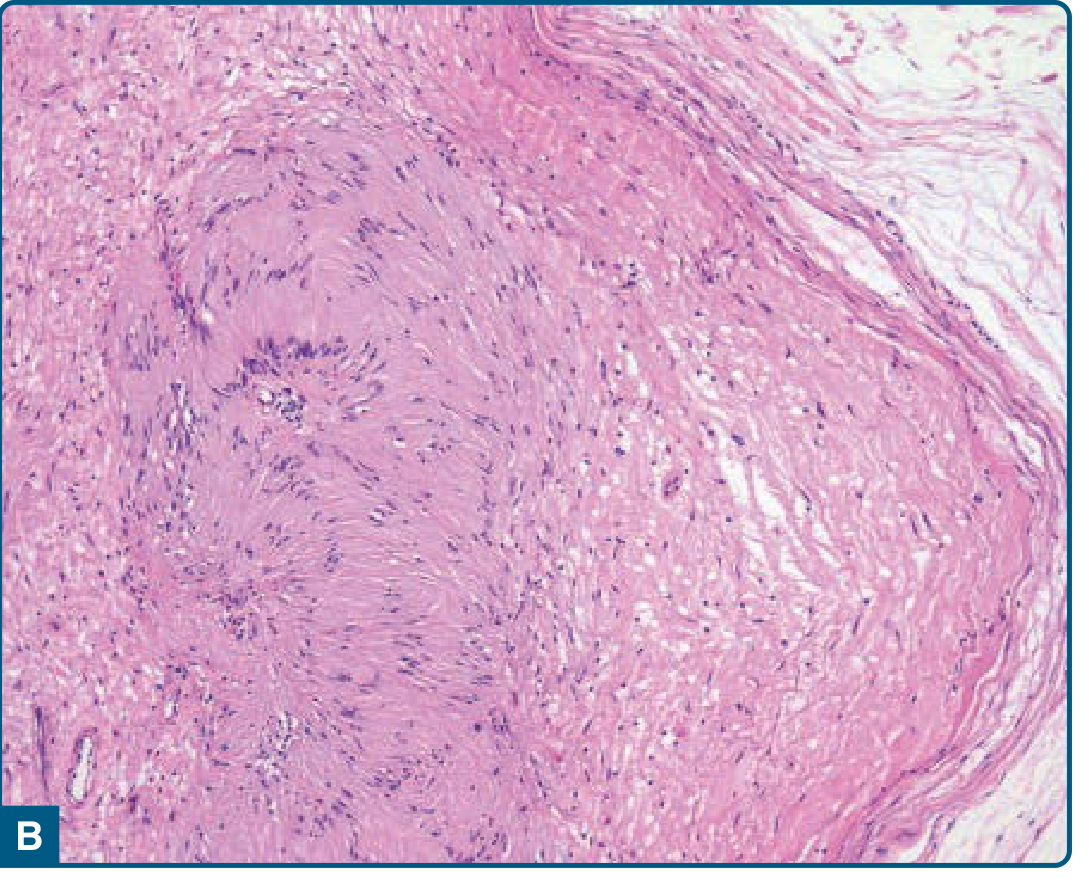
Nuclear palisades surrounding aggregates of cytoplasmic processes = Verocay bodies.
Key Pathology Points
Origin & Definition
- Benign tumor arising from Schwann cells of the peripheral nerve sheath
- Also called neurilemmoma or neurilemoma
- Tumor cells express S-100 protein and SOX10 - key IHC markers
- Surrounded by continuous basement membrane (visible on EM or IHC)
Gross Pathology
- Well-circumscribed, encapsulated mass (fibrous capsule = epineurium + residual nerve fibers)
- Attaches loosely to the nerve but does not invade it - grows eccentrically, displacing nerve fascicles
- Firm, gray/tan-yellow; may be cystic when >3-4 cm
- No axons are detectable within the tumor (unlike neurofibromas)
Microscopic Hallmarks (H&E)
| Feature | Description |
|---|---|
| Antoni A areas | Hypercellular; compact spindle-shaped Schwann cells in short bundles or interlacing fascicles; nuclei elongated, twisted, wavy/"buckled" |
| Antoni B areas | Hypocellular; cells loosely arranged in myxoid matrix; irregular cystic spaces; thick-walled hyalinized blood vessels |
| Verocay bodies | Pathognomonic - two parallel rows of palisading nuclei separated by anuclear zones of stacked cytoplasmic processes (found in Antoni A areas) |
| Blood vessels | Thick-walled, hyalinized - characteristic finding |
| Axons | Absent (excluded from tumor) |
Immunohistochemistry
| Marker | Result |
|---|---|
| S-100 | Strongly and diffusely positive (nuclear + cytoplasmic) |
| SOX10 | Positive |
| EMA | Negative (helps distinguish from perineurioma) |
| CD34 | Variable |
| Neurofilament | Negative (no axons) |
Special Subtypes
| Subtype | Features |
|---|---|
| Ancient schwannoma | Long-standing tumor with marked degenerative changes, nuclear atypia (large hyperchromatic nuclei), but NO mitoses - behaves benignly |
| Cellular schwannoma | Hypercellular, predominantly Antoni A, lacks Antoni B areas - can mimic sarcoma; still benign |
| Plexiform schwannoma | Multiple lobules along nerve; associated with NF2 or schwannomatosis (rare intradermal type) |
| Melanotic psammomatous schwannoma | Associated with Carney syndrome (spotty pigmentation + myxomas + endocrine overactivity) |
Degenerative Changes (especially in Antoni B)
- Hyalinization
- Cyst formation
- Hemorrhage
- Fibrosis
- Calcification
- Xanthomatous change
These are degenerative, not malignant features.
Genetics
- Sporadic schwannomas: somatic inactivating mutations in NF2 gene (chr 22q12)
- NF2 (Neurofibromatosis type 2): autosomal dominant; bilateral vestibular schwannomas are hallmark; NF2 gene product = merlin (cytoskeletal protein; regulates cell shape, growth, adhesion)
- Schwannomatosis: rare familial syndrome with multiple schwannomas without bilateral vestibular schwannomas
MRI Correlates (mirroring histology)
- Predominantly Antoni A component → intermediate signal on T1 and T2
- Predominantly Antoni B component → hyperintense on T2 (loose myxoid stroma)
- "Split fat sign": rim of fat on T1
- "Target sign": low T2 centrally + high T2 peripherally (in ~50% of cases) - suggests benign diagnosis
- Fusiform mass along a nerve course
Key Differentials
| Tumor | Distinguishing Features |
|---|---|
| Neurofibroma | Contains axons, no capsule, no Verocay bodies, wavy collagen "carrot shavings," NF1 association; malignant transformation possible |
| MPNST | High mitoses, necrosis, nuclear pleomorphism, loss of S-100 |
| Leiomyoma | SMA/desmin positive, no S-100 |
| Solitary fibrous tumor | CD34+, STAT6+, patternless architecture |
| Fibrosarcoma | Herringbone pattern, mitoses, no S-100 |
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (Fig. 27.14) | Robbins & Kumar - Basic Pathology (Fig. 20.6) | Fitzpatrick's Dermatology Vol. 1-2 (Fig. 121-22) | Campbell's Operative Orthopaedics 15e | Cummings Otolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.