Imagine you're a examiner , prepare notes on cutaneous amyloidosis for theory examination md
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cutaneous amyloidosis" classification treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from three authoritative dermatology textbooks (Andrews', Dermatology 2-Volume Set 5e, and Fitzpatrick's), complete with clinical images and histology. Here are the complete MD examination notes:
CUTANEOUS AMYLOIDOSIS
MD Dermatology Theory Examination Notes
I. DEFINITION & OVERVIEW
Cutaneous amyloidosis refers to the deposition of amyloid - an extracellular, proteinaceous material - within the skin, either as a primary phenomenon confined to the skin or as part of systemic amyloidosis.
Amyloid in all forms is composed of three components:
- Protein-derived amyloid fibers (the subtype that differs between forms)
- Amyloid P component (~15% of amyloid)
- Ground substance
II. CLASSIFICATION
A. Primary Cutaneous Amyloidosis (Amyloid confined to skin, no systemic involvement)
- Macular amyloidosis
- Lichen amyloidosis (most common form)
- Biphasic amyloidosis
- Nodular amyloidosis
- Familial primary cutaneous amyloidosis syndromes
- Pharmaceutical (injection-site) amyloidosis
B. Secondary Cutaneous Amyloidosis
- Amyloid deposits within pre-existing skin lesions (seborrheic keratoses, BCC, etc.) - a histologic epiphenomenon
C. Systemic Amyloidosis with Skin Involvement
- Primary systemic (AL amyloidosis) - skin involved in ~25-40%
- Secondary systemic (AA amyloidosis)
- Dialysis-related amyloidosis
- Senile systemic amyloidosis
D. Heredofamilial Amyloidosis
III. AMYLOID: ESSENTIAL PROPERTIES
Staining Characteristics
| Stain | Appearance |
|---|---|
| H&E | Homogeneous, hyaline, eosinophilic deposits |
| Congo red | Apple-green birefringence under polarized light |
| Crystal violet | Metachromasia (purple) |
| Thioflavin T | Fluorescence |
| Cotton dyes (Dylon, Pagoda red) | Intense bright orange |
| PAS | Weakly positive, diastase-resistant |
Key discriminator: AA (secondary systemic) amyloid loses Congo red birefringence after potassium permanganate treatment. Primary and localized cutaneous forms do not.
Ultrastructure
- Straight, non-branching, non-anastomosing filaments
- 60-100 nm in diameter
- Irregularly arranged
IV. PRIMARY LOCALIZED CUTANEOUS AMYLOIDOSIS (PLCA)
The macular and lichen forms are also called:
- Keratinocyte-derived amyloidosis
- Frictional amyloidosis
- Frictional melanosis
Pathogenesis
The amyloid contains keratin (primarily keratin 5) as its protein component - strongly suggesting traumatic damage to basal keratinocytes causes the deposits. Rubbing and chronic friction lead to apoptosis of keratinocytes, which are then deposited as amyloid in the papillary dermis.
Risk factors:
- Asian, Hispanic, Middle Eastern ancestry
- Use of abrasive devices during bathing (nylon brushes, towels)
- Coexistent atopic dermatitis
- Primary biliary cirrhosis
- Chronic renal failure
V. MACULAR AMYLOIDOSIS
Epidemiology: Women >> men (5:1 ratio); presents in early adulthood; chronic course
Clinical features:
- Moderately pruritic brown, grey-brown macules
- Characteristic rippled or "salt and pepper" appearance - best appreciated by stretching the skin
- Confluent or rippled pigmentation pattern
- Primary site: interscapular region of the back; also thighs, shins, arms, breasts, buttocks
Key association: Many cases between the scapulae result from rubbing of dysesthetic areas in notalgia paresthetica

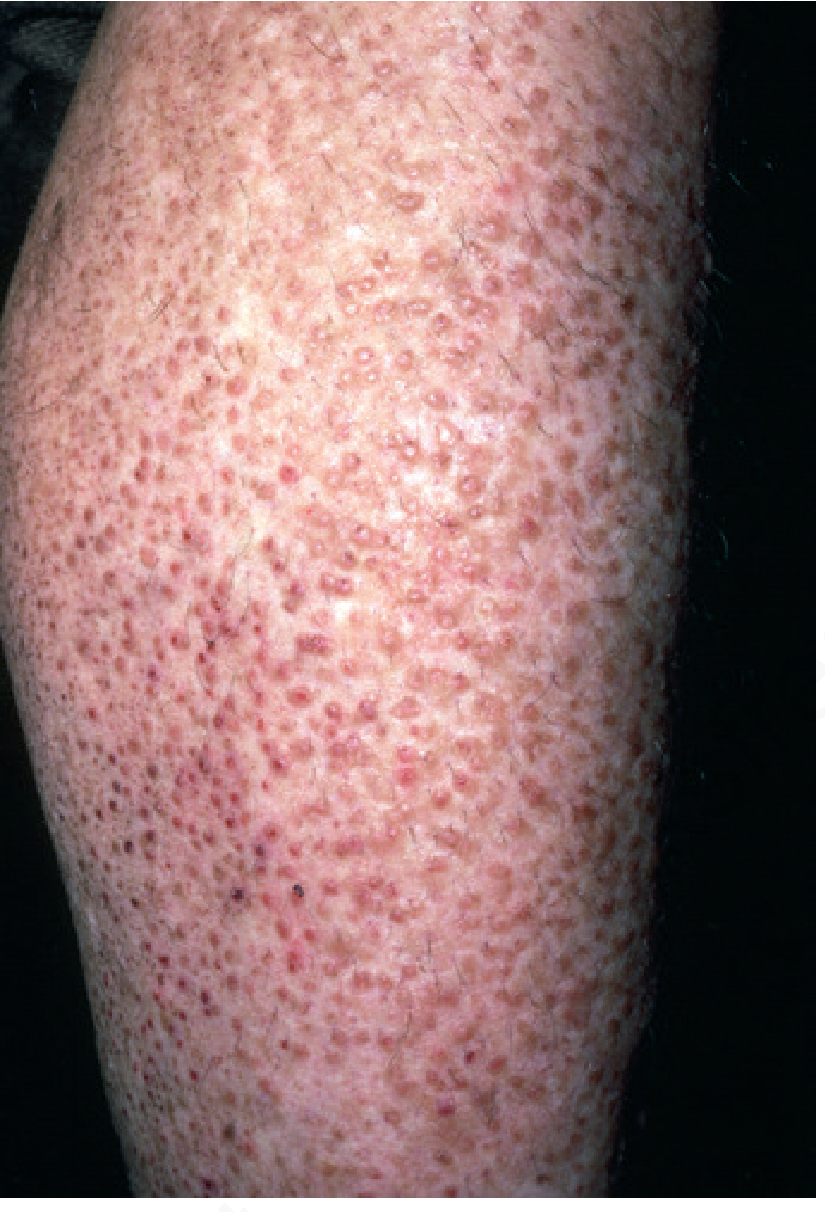
VI. LICHEN AMYLOIDOSIS
The most common form of primary cutaneous amyloidosis
Clinical features:
- Persistent, pruritic plaques on the shins and other extensor surfaces (anterior thighs, forearms)
- Initial: discrete, firm, scaly, skin-colored or hyperpigmented papules
- Later: coalesce into plaques with rippled or ridged pattern
- Initially unilateral; over time bilateral symmetric distribution
- Intense pruritus is a hallmark
VII. BIPHASIC AMYLOIDOSIS
- Fine papular lesions (lichen) are superimposed upon a background of macular hyperpigmentation
- Represents the clinical overlap between macular and lichen forms
- Both forms share the same pathogenic basis (friction/rubbing)
VIII. NODULAR AMYLOIDOSIS
Rare; distinct pathogenesis from macular/lichen forms
Clinical features:
- Single or multiple waxy nodules or tumefactions
- Sites: acral areas, trunk, genitalia, face
- Asymptomatic; slowly enlarging
- Overlying epidermis may appear atrophic; may resemble bullae
Amyloid type: Immunoglobulin-derived AL amyloid (not keratin-derived) - produced locally by plasma cells in the vicinity
Key associations:
- Sjogren syndrome (up to 25% of cases) - typically around age 60, often precedes the diagnosis
- Systemic sclerosis/CREST
- Rheumatoid arthritis
Risk of systemic progression: ~7% (previously quoted as 50% - reassessed in recent data). Long-term follow-up is required. Regular evaluation for plasma cell dyscrasia or lymphoproliferative disease is indicated.
Important concept: Some cases of nodular amyloidosis may represent a variant of primary cutaneous marginal zone lymphoproliferative disorder - monoclonal plasma cells have been demonstrated. Despite this, prognosis is excellent.
IX. VARIANT FORMS
| Variant | Key Feature |
|---|---|
| Anosacral amyloidosis | Brownish patches/plaques in anosacral region; pruritic; described mainly in Chinese and Japanese patients |
| Friction (towel) amyloidosis | Due to prolonged contact with nylon towels/brushes; likely a variant of macular/lichen amyloidosis |
| Notalgia paresthetica amyloidosis | Isolated sensory neuropathy on back; amyloid from prolonged scratching |
| Lichen amyloidosis of auricular concha | Hyperpigmentation of the bowl of the ear |
| Pharmaceutical (injection-site) amyloidosis | At sites of insulin, other drug injections |
X. FAMILIAL PRIMARY CUTANEOUS AMYLOIDOSIS SYNDROMES
1. IL-31 Receptor-Associated Amyloidosis (PLCA1 and PLCA2)
- PLCA1: Pathogenic variants in OSMR gene (oncostatin M receptor beta subunit)
- PLCA2: Pathogenic variants in IL-31RA gene (IL-31 receptor alpha subunit)
- OSMR and IL-31RA together form the IL-31 receptor
- IL-31 is important in pruritic skin conditions (atopic dermatitis, prurigo nodularis)
- Nemolizumab (anti-IL-31RA antibody) - potential therapeutic target
2. Dyschromic Amyloidosis (PLCA3)
- Guttate leukoderma superimposed on hyperpigmentation + macular/lichen amyloidosis features
- Caused by mutations in GPNMB gene (glycoprotein nonmetastatic melanoma protein b)
3. MEN Type 2A (Sipple Syndrome) - KEY ASSOCIATION
- Autosomal dominant: medullary carcinoma of thyroid + pheochromocytoma + hyperparathyroidism
- Pruritic hyperpigmentation on the upper back (macular/lichen amyloidosis)
- Unusual: early onset, often before age 10 years
- 36% incidence of lichen amyloidosis in MEN 2A
- All cases associated with pathogenic variant in codon 634 of RET proto-oncogene
- Recognition can lead to prophylactic thyroidectomy
4. X-linked Reticulate Pigmentary Disorder (Partington Amyloidosis)
- X-linked; adult women: linear streaks of hyperpigmentation; male patients: reticulated mottled brown pigmentation with dermal amyloid deposits on biopsy
XI. HISTOPATHOLOGY
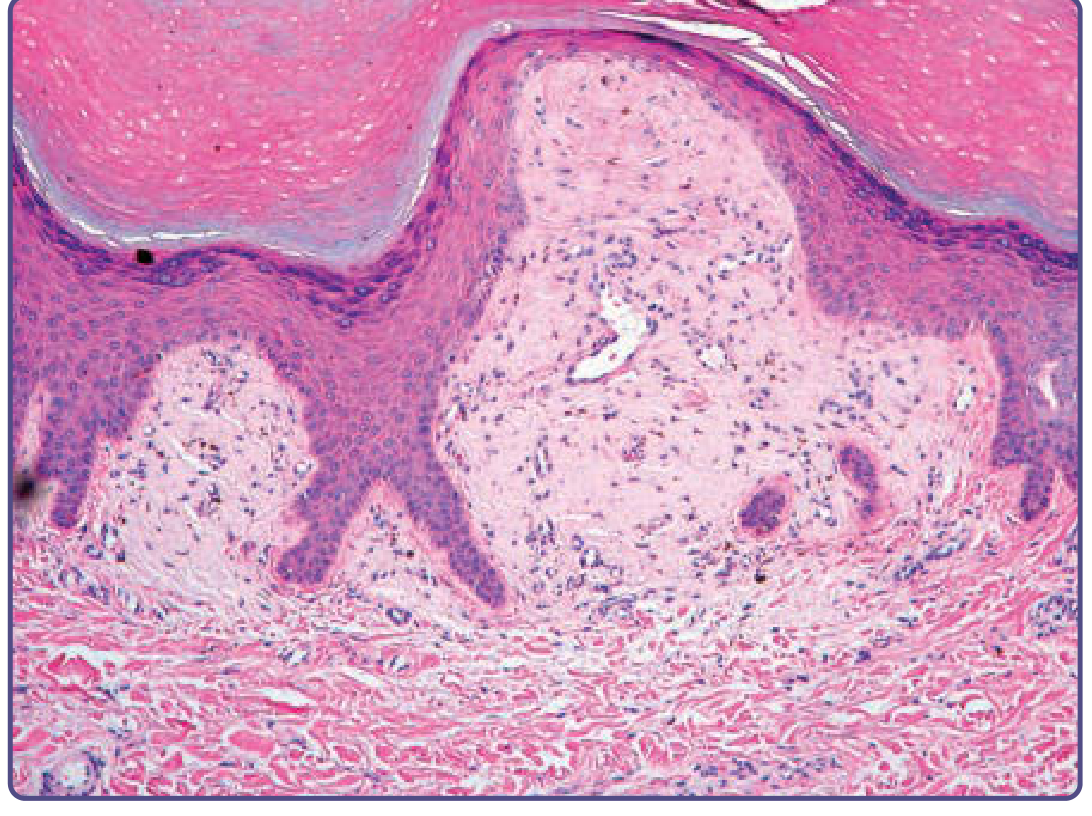
Macular and Lichen Amyloidosis
- Amyloid deposits restricted to the upper (papillary) dermis
- In lichen amyloidosis: amyloid expands dermal papillae, displaces elongated rete ridges laterally
- Overlying epidermis: hyperkeratosis and acanthosis (from chronic rubbing)
- Focal necrotic keratinocytes in basal cell layer
- Melanophages present within/adjacent to amyloid deposits (explains hyperpigmentation)
- Sparse perivascular lymphohistiocytic infiltrate
- Microscopic (rarely macroscopic) bullae may be seen (analogous to lichen planus)
Nodular Amyloidosis
- Amyloid diffusely infiltrates the dermis, subcutis, and blood vessel walls
- Nearly universal perivascular infiltrate of plasma cells (usually monoclonal)
- Immunostaining for light chain deposition helps diagnosis
Histopathologic Features - Summary Table
| Feature | Macular/Lichen | Nodular |
|---|---|---|
| Location | Papillary dermis | Dermis + subcutis + vessels |
| Amyloid protein | Keratin (CK5) | AL (immunoglobulin light chains) |
| Plasma cells | Absent | Present (monoclonal) |
| Pigment incontinence | Present | Uncommon |
Confirmatory Stains
- Antikeratin antibodies (MNF 116): Confirm keratin origin in macular/lichen forms
- DIF: IgM in globular pattern (passive absorption, not specific deposition) in keratin-derived forms
- Amyloid P component immunostaining: Stains all forms of amyloid
XII. SECONDARY CUTANEOUS AMYLOIDOSIS
Amyloid deposits found histologically within pre-existing skin lesions:
- Most common: seborrheic keratoses and basal cell carcinomas
- Also: dermatofibromas, melanocytic nevi, pilomatricomas, trichoepitheliomas, sweat gland tumors, Bowen disease, porokeratosis
- Also after PUVA therapy
- Clinical significance: histologic epiphenomenon - no clinical implications
Special entity - Hypotrichosis simplex of the scalp (HYPT2): A form of secondary cutaneous amyloidosis. Autosomal dominant. Progressive loss of scalp hair by 3rd decade. Mutations in corneodesmosin gene - truncated proteins accumulate as amyloid around hair follicles and papillary dermis.
XIII. SYSTEMIC AMYLOIDOSIS WITH SKIN SIGNS
AL (Primary Systemic) Amyloidosis
- Skin involvement in ~25-40%
- Amyloid composed of immunoglobulin light chains, usually lambda (λ) subtype (75-80%)
- Cutaneous features:
- Shiny, smooth, firm, flat-topped waxy papules (translucent vesicle-like appearance)
- Periorbital purpura - "Raccoon eyes" sign / "Pinch purpura" (precipitated by coughing, Valsalva, proctoscopy, tape removal)
- Macroglossia (enlarged, firm tongue)
- Nail dystrophy, alopecia
- Lesions around eyes, nose, mouth, mucocutaneous junctions
- Petechiae, purpura, ecchymoses - especially axillae, eyelids, anogenital regions
- Oral: rubbery swellings of mucosa, hemorrhagic papules, xerostomia
XIV. DIFFERENTIAL DIAGNOSIS
For Macular Amyloidosis
- Notalgia paresthetica (key DDx - also rippled hyperpigmentation on upper back; early lesions lack amyloid on biopsy)
- Postinflammatory hyperpigmentation
- Pityriasis versicolor
- Atrophic lichen planus
- Erythema dyschromicum perstans (ashy dermatosis)
- Drug-induced pigmentation
For Lichen Amyloidosis
- Lichen simplex chronicus - no amyloid on biopsy
- Hypertrophic lichen planus - lichenoid infiltrate, vacuolar degeneration; no amyloid
- Prurigo simplex/nodularis
- Papular mucinosis
- Pretibial myxedema
- Pemphigoid nodularis
- Epidermolysis bullosa pruriginosa
- Lichen ruber moniliformis
For Nodular Amyloidosis
- Primary systemic amyloidosis (must be excluded)
- Cutaneous lymphoid hyperplasia
- Sarcoidosis
- Colloid milium
XV. TREATMENT
General Principle
No treatment is curative or uniformly effective. Treatment must focus on breaking the itch-scratch-itch cycle.
Treatment of Macular and Lichen Amyloidosis
| Evidence Level | Treatment |
|---|---|
| First-line | Reduce friction; identify cause of rubbing; occlusion |
| Topical | High-potency topical corticosteroids; intralesional steroids (small areas) |
| Topical adjuncts | Tacrolimus 0.1% ointment; calcipotriol; tar |
| Phototherapy | PUVA (marginally better for pruritus); UVB; Re-PUVA (with retinoids) |
| Systemic (refractory) | Oral retinoids (acitretin, alitretinoin); amitriptyline (for pruritus); thalidomide; cyclosporin; low-dose cyclophosphamide (50 mg/day); systemic corticosteroids; dupilumab (recent evidence) |
| Physical | Dermabrasion (effects lasting ≥5 years); CO2 laser; Erbium:YAG laser |
| Laser for pigmentation | 532-nm Q-switched Nd:YAG laser for macular amyloidosis pigmentation |
Treatment of Nodular Amyloidosis
- Physical removal: shave excision and destruction of base
- Surgical excision, cryotherapy, electrodesiccation, CO2 laser
- Caution: local recurrences are common
- Rare recurrences may lack amyloid and show features of primary cutaneous marginal zone lymphoma
- Regular systemic follow-up for plasma cell dyscrasia
XVI. HIGH-YIELD EXAM POINTS (EXAMINER'S PERSPECTIVE)
- Most common form of primary cutaneous amyloidosis = Lichen amyloidosis
- Amyloid protein in macular/lichen forms = Keratin 5 (keratinocyte-derived)
- Amyloid protein in nodular amyloidosis = AL (immunoglobulin light chains)
- Congo red stain under polarized light = Apple-green birefringence
- Potassium permanganate test differentiates AA from AL - AA loses birefringence; AL/cutaneous forms retain it
- Genes in familial PLCA: OSMR (PLCA1), IL-31RA (PLCA2), GPNMB (PLCA3 - dyschromic amyloidosis)
- MEN 2A association: Lichen amyloidosis + upper back lesions + codon 634 RET mutation
- Nodular amyloidosis - 7% risk of systemic progression; association with Sjogren syndrome (25%)
- Rippled pattern - best seen by stretching the skin (macular amyloidosis)
- Dermabrasion - effective for lichen amyloidosis on limbs with effects lasting >5 years
- Dupilumab - recent evidence for lichen amyloidosis (IL-31 pathway link)
- "Pinch purpura" / "Raccoon eyes" = classic skin sign of AL (primary systemic) amyloidosis
- Secondary cutaneous amyloidosis = histologic finding only, no clinical implication
- DIF in keratin-derived amyloidosis: IgM in globular pattern (passive absorption, not specific)
- Histology - lichen amyloidosis: Amyloid in papillary dermis + widened papillae + displaced rete ridges + melanophages + hyperkeratosis
Sources: Andrews' Diseases of the Skin (Clinical Dermatology), Dermatology 2-Volume Set 5e, Fitzpatrick's Dermatology Volumes 1-2
This is a shared conversation. Sign in to Orris to start your own chat.