Active and passive stretching for tfl muscles with application doses and positioning
Reading File
Checking Date & Time
Finding Sources
Finding Sources
Searching PubMed
"tensor fasciae latae" OR "iliotibial band" AND stretching
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
tensor fasciae latae TFL stretching technique
Finding Sources
Loading Image
Loading Image
Finding Sources
Finding Sources
Finding Sources
Here is a comprehensive clinical guide on active and passive TFL stretching, with positioning, application doses, and images.
Tensor Fasciae Latae (TFL) Stretching — Active & Passive Techniques
Anatomy Recap
The TFL originates from the outer iliac crest between the ASIS and the iliac tubercle, and inserts via the iliotibial (IT) band into the lateral tibial condyle (Gerdy's tubercle). It is innervated by the superior gluteal nerve and performs hip flexion, abduction, and internal rotation while stabilizing the knee in extension.
— Gray's Anatomy for Students
Because of this multi-planar action, effective stretching requires combining extension + adduction + external rotation of the hip simultaneously.
Functional Position for TFL Lengthening
To maximally elongate the TFL/IT band complex, the target limb must be placed in:
- Hip extension (opposing its flexion role)
- Hip adduction (opposing its abduction role)
- Hip external rotation (opposing its internal rotation role)
- Knee in neutral or slight flexion
Passive Stretching Techniques
Passive stretching means an external force (therapist, gravity, strap, wall) moves the limb to end range — the patient does not actively generate the stretch.
1. Supine Cross-Leg (Ober Test Position Stretch) — Therapist-Assisted
Positioning:
- Patient supine, hip at the edge of the table
- Target leg: therapist extends the hip to ~10–15°, adducts across the midline, and applies gentle external rotation
- Non-target leg: flexed at hip/knee, foot flat on table to stabilize the pelvis
- Therapist stabilizes the pelvis with one hand to prevent compensatory lateral pelvic tilt
Application Dose:
| Parameter | Recommendation |
|---|---|
| Hold duration | 30–60 seconds per repetition |
| Repetitions | 3–5 reps |
| Sets | 1–2 sets per session |
| Sessions/week | 5–7 days/week for tightness management |
| Total stretch time | 2–3 minutes/session |
Note: Evidence supports ≥30 seconds per static stretch hold to produce viscoelastic lengthening; longer holds (45–60 s) are preferred in patients with significant tightness (e.g., IT band syndrome).
2. Side-Lying Passive Gravity Stretch (Ober Stretch)
Positioning:
- Patient side-lying with the target limb on top
- Bottom leg hip flexed ~30° for stability
- Therapist (or gravity alone) allows the top limb to fall into adduction off the edge of the table while keeping the hip in extension
- Pelvis must remain neutral — do not allow trunk side-bend
- A rolled towel under the waist can maintain spine neutral
Application Dose:
| Parameter | Recommendation |
|---|---|
| Hold | 30–60 seconds |
| Reps | 3–5 |
| Sessions/week | 5–7 |
3. Standing Wall-Assisted Passive Stretch
Positioning:
- Patient stands sideways to a wall, target limb nearest the wall
- Target foot crossed behind and beyond the contralateral foot (hip adduction)
- Both hands on wall or hip; lean the trunk away from the target side (lateral flexion to the opposite side) — this further opens the lateral hip
- Keep both feet flat and knees soft
Application Dose:
| Parameter | Recommendation |
|---|---|
| Hold | 30–45 seconds |
| Reps | 3–5 per side |
| Frequency | Daily |
Active Stretching Techniques
Active stretching uses the patient's own muscle contraction (typically the antagonist) to create and maintain the stretch position, without external assistance. This improves neuromuscular control alongside flexibility.
1. Standing Active TFL Stretch (Cross-Leg + Lateral Trunk Lean)
This is the most clinically used active stretch for TFL/IT band.
Positioning (three progressions — see image below):
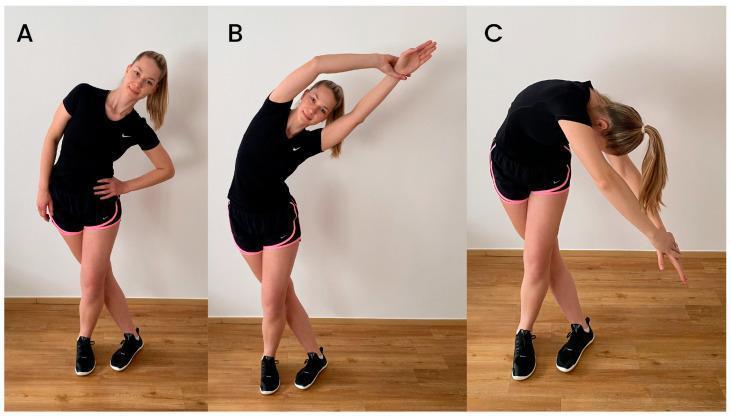
- A (Basic): Target limb crossed behind the stance leg; one hand on hip; actively lean the trunk toward the non-target side
- B (Intermediate): Same lower body; clasp hands and reach arms overhead, increasing lateral trunk flexion and stretch tension
- C (Advanced): Trunk rotated and flexed diagonally toward the floor — bilateral arm reach adds a kinetic chain component
Muscle generating stretch: Contralateral lateral flexors (quadratus lumborum, obliques) actively hold the lean position; no external force needed.
Application Dose:
| Parameter | Recommendation |
|---|---|
| Hold duration | 20–30 seconds per position |
| Reps | 3–5 per position per side |
| Progressions | Start with A; advance to B and C over 1–2 weeks |
| Frequency | Daily or 5×/week |
| Warm-up | Perform after 5–10 min light aerobic warm-up |
2. Active PNF Stretching — Contract-Relax (CR) Technique
PNF (proprioceptive neuromuscular facilitation) CR technique produces greater ROM gains than static stretching alone by exploiting autogenic inhibition.
Positioning:
- Patient supine or side-lying (same position as therapist-assisted passive stretch)
- TFL brought to its end range of extension + adduction + ER
Protocol:
- Therapist moves the limb to first point of resistance (TFL end range)
- Patient isometrically contracts the TFL (abduction + internal rotation) against therapist resistance for 6–10 seconds at 60–75% effort
- Patient relaxes completely for 2–3 seconds
- Therapist advances limb to new end range and holds for 20–30 seconds
- Repeat 2–4 cycles per session
Application Dose:
| Parameter | Recommendation |
|---|---|
| Contraction duration | 6–10 seconds |
| Relax/advance | 2–3 seconds |
| Passive hold after | 20–30 seconds |
| Cycles | 3–4 per session |
| Frequency | 3–5×/week (PNF is more demanding — recovery needed) |
3. Active Isolated Stretching (AIS) — Dynamic Active Stretch
Used in sports rehab; limb is moved actively to end range, held briefly, then released.
Positioning:
- Supine; target hip brought into full extension, adduction, ER by active contraction of opposing muscles (gluteus maximus, hip adductors, hip ER)
- Hold at end range for only 1–2 seconds, then release and repeat rhythmically
Application Dose:
| Parameter | Recommendation |
|---|---|
| Hold | 1–2 seconds only |
| Reps | 8–12 repetitions |
| Sets | 2–3 |
| Frequency | Daily; suitable as warm-up |
Myofascial Release — Foam Rolling (Adjunct)
Self-myofascial release (SMFR) targets the IT band/TFL fascia and complements stretching.
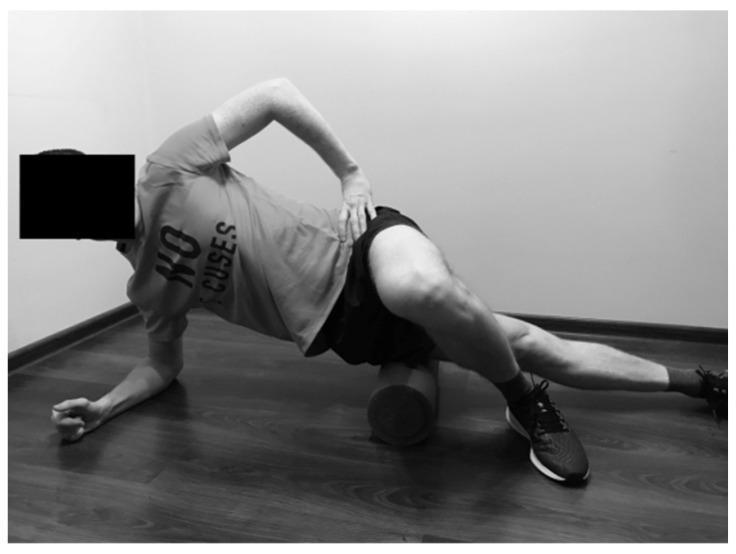
Positioning:
- Side-lying on foam roller; roller placed between iliac crest and knee on the lateral thigh
- Support on forearm and opposite foot (cross it in front for control)
- Slowly roll along the IT band from hip to just above the lateral knee
Application Dose:
| Parameter | Recommendation |
|---|---|
| Roll speed | Slow (1 cm/sec); pause 20–30 s on tender spots |
| Duration | 60–90 seconds per side |
| Frequency | Before and/or after stretching, daily |
Summary Dosing Table
| Technique | Type | Hold | Reps | Sets | Frequency |
|---|---|---|---|---|---|
| Supine therapist-assisted | Passive static | 30–60 s | 3–5 | 1–2 | 5–7×/week |
| Ober side-lying gravity | Passive static | 30–60 s | 3–5 | 1–2 | 5–7×/week |
| Standing cross-leg lean | Active static | 20–30 s | 3–5 | 1–2 | Daily |
| PNF contract-relax | Active PNF | 6–10 s contract + 20–30 s hold | 3–4 cycles | 1 | 3–5×/week |
| Active isolated (AIS) | Active dynamic | 1–2 s | 8–12 | 2–3 | Daily |
| Foam rolling (SMFR) | Myofascial | 60–90 s | — | 1 per side | Daily |
Clinical Pearls
- Pelvic stability is critical — all TFL stretches fail if the pelvis tilts laterally or anteriorly to compensate. Always cue/stabilize the pelvis first.
- The Ober test (side-lying passive hip adduction) is both the assessment and the passive stretch for TFL/IT band — a positive test (limb does not adduct to table) confirms tightness.
- In IT band syndrome, stretching alone has limited direct effect on the IT band (it is relatively inextensible); the benefit comes from lengthening the TFL muscle belly and its fascial proximal attachments.
- PNF > static stretching for immediate ROM gains per session; static stretching produces more durable long-term changes with daily practice.
- Stretching is most effective when the muscle is warm — perform after aerobic warm-up or heat application.
- A recent RCT (Unuvar et al., 2024 — PMID 39159925) found that myofascial release techniques significantly improved pain, ROM, and muscle strength in athletes with IT band tightness, supporting the combination of SMFR + stretching over stretching alone.
This is a shared conversation. Sign in to Orris to start your own chat.