Bone healing absolute and relative stability
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed to write a thorough, well-structured answer. Here it is:
Bone Healing: Absolute vs. Relative Stability
The Core Concept - Strain Theory
The mechanical environment at the fracture site is the primary determinant of how a fracture heals. The key variable is interfragmentary strain, defined as:
Strain (ε) = Change in fracture gap (ΔL) / Original fracture gap (L)
This elegant formula, developed by Perren, explains why two identical fractures can heal by completely different mechanisms depending on fixation:
| Strain Level | Tissue Formed | Type of Healing |
|---|---|---|
| 0% (no motion) | Bone directly | Primary (direct) bone healing |
| < 2% | Hard callus / lamellar bone | Direct cortical healing |
| 2% - 10% | Soft callus → endochondral ossification | Secondary (indirect) healing |
| > 10% | No bone formation possible | Fibrous tissue / nonunion risk |
- Miller's Review of Orthopaedics, 9th Ed.
A critical insight: stability determines strain, and strain determines the type of healing. This is why fixation technique is not just a mechanical decision - it is a biological one.
Absolute Stability
Definition
No motion at the fracture site under physiologic load. Strain is zero or near-zero.
Mechanism of Healing - Primary (Direct) Bone Healing
Bone heals without an intermediate callus phase. The process bypasses the inflammatory and repair stages and goes directly to remodeling. Osteoclastic cutting cones advance across the fracture interface, with trailing osteoblasts laying down lamellar bone - the same process as normal skeletal remodeling, just directed across a fracture line.
There are two subtypes:
- Contact healing - where fracture surfaces are in direct cortical apposition (gap < 0.01 mm), cutting cones bridge the gap and new osteons form directly across it.
- Gap healing - where a small residual gap exists (0.01 - 1 mm), lamellar bone fills the gap first (oriented perpendicular to the fracture line), followed later by secondary remodeling with longitudinally oriented osteons.
Key Clinical Features
- No periosteal callus - healing is radiographically invisible, making it difficult to confirm union on plain films.
- Slower overall healing - despite appearing more "controlled," primary bone healing is actually a slower process than secondary healing.
- Risk of refracture after plate removal - because healing is invisible radiographically, early hardware removal risks refracture through the original fracture site. Plate removal should be delayed up to 2 years.
- Technically demanding - achieving true absolute stability in clinical practice is difficult. Even in optimized animal models using two orthogonal compression plates, gap healing was seen at the cortex opposite the plates due to bending moments. Modern clinical studies aiming for absolute stability show callus in nearly all cases.
Implants That Provide Absolute Stability
- Compression plating (oval/dynamic compression plate holes) - applies compressive force across the fracture
- Lag screws - provide rigid interfragmentary compression; typically a neutralization plate is needed alongside to protect against deforming forces
- Lag screw + neutralization plate combination - the most reliable method for simple fractures
When to Choose Absolute Stability
- Simple (two-part) fracture patterns: transverse or short oblique diaphyseal fractures
- Intra-articular fractures - require anatomical reduction AND absolute stability to minimize posttraumatic arthritis risk
- Surgically accessible fractures where direct reduction can be achieved without extensive soft tissue stripping
- Rockwood and Green's Fractures in Adults, 10th Ed., 2025
Relative Stability
Definition
Controlled micromotion exists at the fracture site under physiologic load. The fixation splints but does not compress the fracture.
Mechanism of Healing - Secondary (Indirect) Bone Healing
This is the most common and most biologically robust form of fracture healing, proceeding through sequential tissue differentiation:
- Fracture hematoma - immediate (hours); provides growth factors (TGF-β, PDGF, BMP) and initial scaffold
- Fibrous/granulation tissue - days to weeks; strain can still be high, tissue is flexible
- Soft callus (fibrocartilage) - weeks; cartilage can tolerate higher strains than bone; periosteal callus forms preferentially and is biomechanically superior
- Hard callus - mineralization of cartilage template via endochondral ossification; strain decreasing as callus matures and widens
- Remodeling - lamellar bone replaces woven bone over months to years; Wolff's law directs architecture along stress lines
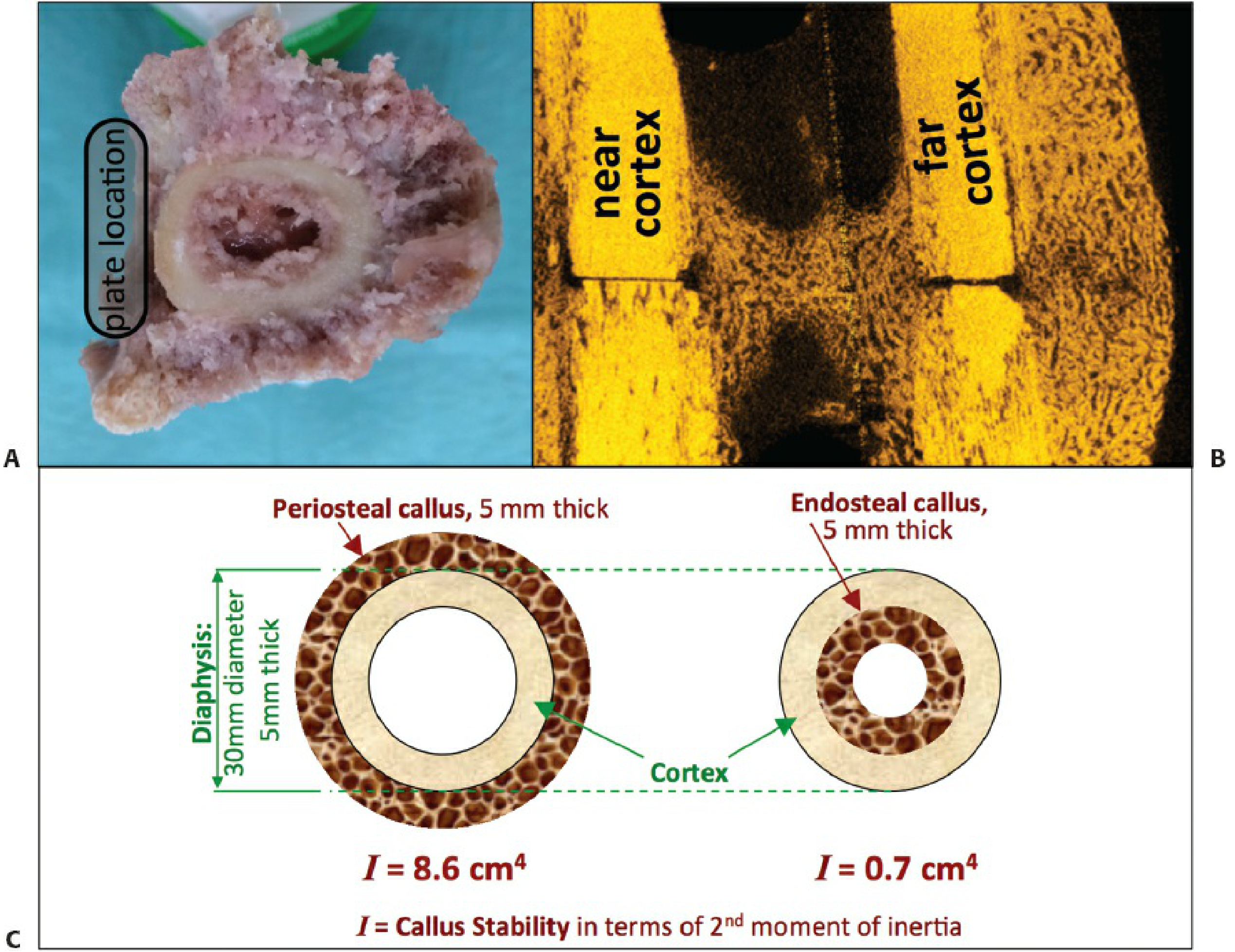
The periosteal callus response is highly efficient: a 5-mm thick periosteal callus provides 12 times more structural stability (I = 8.6 cm⁴) than a 5-mm thick endosteal callus (I = 0.7 cm⁴), because the periosteal callus forms at a greater distance from the neutral axis of the bone.
A self-reinforcing cycle operates: micromotion stimulates callus, callus reduces strain, reduced strain promotes further bone formation, increasing stability further.
Key Clinical Features
- Visible callus on X-ray - radiographic union is easier to confirm.
- Faster functional recovery overall in many fracture types.
- Fracture hematoma must be preserved - indirect reduction techniques are preferred; opening the fracture sacrifices the biology.
- Risk of hypertrophic nonunion if too much motion exists - the callus hypertrophies trying to spread force over a wider area but fails to bridge the gap.
- Risk of atrophic nonunion if fixation is too stiff with a residual fracture gap (no motion, no biology, no healing).
Implants That Provide Relative Stability
- Intramedullary (IM) nails - load-sharing, allow controlled axial and rotational micromotion
- External fixators - adjustable stiffness
- Bridge plates (spanning comminuted zones) - working length is long, construct flexibility allows callus
- Casts and fracture braces - simplest form; in vivo studies show tibial fractures brace-treated with 4 mm of interfragmentary motion still heal
When to Choose Relative Stability
- Comminuted fractures (metaphyseal or diaphyseal) - anatomical reduction of all fragments is not possible or biologically costly
- Fractures where soft tissue stripping for direct reduction would devascularize fragments
- Diaphyseal fractures amenable to IM nailing
- Polytrauma patients benefiting from minimal soft tissue dissection (damage control orthopaedics)
- Rockwood and Green's Fractures in Adults, 10th Ed.; Bailey and Love's Surgery, 28th Ed.
Choosing Between the Two: Surgical Decision Framework
| Factor | Absolute Stability | Relative Stability |
|---|---|---|
| Fracture pattern | Simple (transverse, oblique) | Comminuted, multifragmentary |
| Location | Articular, diaphyseal simple | Metaphyseal, diaphyseal comminuted |
| Soft tissue | Good; direct access possible | Compromised; preserve biology |
| Reduction | Anatomical, direct | Indirect preferred |
| Expected healing | No callus, slower, invisible on XR | Callus, faster visual confirmation |
| Implant examples | Lag screw ± plate, compression plate | IM nail, external fixator, bridge plate |
| Failure mode | Implant fatigue if delayed healing | Hypertrophic nonunion if too mobile |
When planning operative treatment, the surgeon targets either relative or absolute stability to induce endochondral or intramembranous ossification, respectively. Absolute stability requires removing the fracture hematoma to permit interfragmentary compression, while relative stability can often be achieved through indirect reduction while preserving the hematoma.
- Rockwood and Green's Fractures in Adults, 10th Ed., 2025 (Fig. 2-8)
Perren's Strain Theory - The Unifying Principle
The strain theory explains several clinical observations that were previously poorly understood:
- Why a simple transverse fracture fixed with a single bridge plate (long working length, some flexibility) can develop callus, while the same fracture fixed with compression plating heals without it.
- Why a comminuted fracture with many small fragments cannot be treated with compression plating - the geometry means strain will be very high at remaining gaps even with rigid fixation, causing nonunion.
- Why fracture gap size matters even under the same fixation: a larger gap under absolute stability leads to gap healing rather than contact healing; a larger gap under relative stability concentrates strain and may exceed the healing threshold.
The strain formula (ΔL/L) explains the paradox: a 1-mm motion at a 1-mm gap = 100% strain (no healing possible), while the same 1-mm motion at a 10-mm gap = 10% strain (soft callus forms). This is why comminuted fractures with larger effective gaps are more tolerant of motion.
- Miller's Review of Orthopaedics, 9th Ed.; Bailey and Love's, 28th Ed.
Summary
| Absolute Stability | Relative Stability | |
|---|---|---|
| Strain | 0-2% | 2-10% |
| Healing type | Primary (direct) | Secondary (indirect) |
| Ossification | Intramembranous | Endochondral |
| Callus | Absent | Present |
| Confirmation | Difficult (no callus) | Easy (visible callus) |
| Speed | Slower | Faster |
| Motion at site | None | Controlled micromotion |
This is a shared conversation. Sign in to Orris to start your own chat.