


Imbalance Romberg dono towards right backwards Tandem Imbalance Fukuda > 1m Ddk affected Push forward sensation Vertigo dizziness kuch ni No migraine md history B/l mild sloping snhl Conscious fall h face down.. chlte chlte gir jaate h...and pta lg jaata h ab girne wale h Kindly provide me the full detailed analysis of VNG with pictures and MRI. AND HELP ME TO MADE THE DIAGNOSIS
Reading File
Reading File
Running Command
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
VNG videonystagmography smooth pursuit saccade test interpretation
Searching Images
cerebellar ataxia gait imbalance MRI brain cerebellar atrophy
Searching Images
Dix-Hallpike test BPPV positional nystagmus VNG
Searching the Web
VNG interpretation smooth pursuit gain reduced bilateral central vestibular cerebellar 2024
Loading Image
Loading Image
Loading Image
Now I have all the data needed for a comprehensive analysis. Let me compose the full detailed report.
🧠 Complete VNG Analysis & Diagnosis
Patient: Laxmi Narayan | 75 yr/M | Date: 09-May-2026
CLINICAL SUMMARY (From Prescriptions + History)
| Parameter | Finding |
|---|---|
| Age/Sex | 75 years, Male |
| Chief complaint | Imbalance, forward push sensation, conscious falls (face down while walking — knows he is about to fall) |
| Romberg | Falls towards right backwards |
| Tandem gait | Impaired |
| Fukuda stepping test | Deviation >1 meter |
| DDK (Diadochokinesis) | Affected |
| Vertigo/Dizziness | Absent |
| Migraine | No history |
| Hearing | B/L mild sloping SNHL |
| Psychiatric Rx | Mixed anxiety & depression (Tab Restonorm 15 LS + Tab Clonil 50 mg) |
| ENT Opinion (Dr. Abhay Kumar Singh) | Vestibular evaluation — complete evaluation; Cerebellar involvement noted; Special emphasis on Vestibular system |
VNG FULL ANALYSIS (Parameter by Parameter)
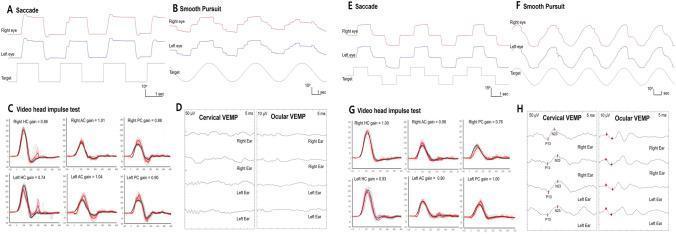
1. SACCADE TEST
| Test | Right Eye | Left Eye | Interpretation |
|---|---|---|---|
| 0.3 Hz H – Velocity | 498.35°/s | 561.86°/s | ✅ Normal (>275°/s) |
| 0.3 Hz H – Precision | 74.71% | 60.27% | ⚠️ Low (normal 80–134%) — Left eye hypometric |
| 0.3 Hz H – Latency | 435.79 ms | 489.41 ms | 🔴 Markedly prolonged (normal <260 ms) |
| 0.45 Hz H – Precision | 68.99% | 54.12% | 🔴 Bilateral hypometria |
| 0.45 Hz H – Latency | 413.33 ms | 401.38 ms | 🔴 Prolonged bilaterally |
| 0.3 Hz V – Velocity | 189.93°/s | 195.48°/s | ⚠️ Reduced (esp. vertical — cerebellar) |
| 0.3 Hz V – Precision | 60.72% | 63.04% | 🔴 Bilaterally hypometric |
| 0.45 Hz V | Velocity 292/419°/s | Precision 83/96% | Relatively preserved |
Interpretation:
- Bilaterally prolonged saccade latency — strongly suggests central (cerebellar/cortical frontal lobe) origin
- Saccade velocity preserved (rules out severe brainstem/INO), but accuracy (precision) is bilaterally low, indicating cerebellar dysmetria of saccades
- This is the hallmark of cerebellar saccadic dysfunction — the cerebellum (vermis, fastigial nucleus) normally corrects saccade accuracy
🔑 Key: Saccadic dysmetria (hypometria) + prolonged latency = central oculomotor dysfunction, cerebellar pattern
2. SMOOTH PURSUIT TEST
| Test | Rightward Gain (R/L eye) | Leftward Gain (R/L eye) |
|---|---|---|
| 0.2 Hz H | 0.49 / 0.53 | 0.65 / 0.71 |
| 0.4 Hz H | 0.29 / 0.32 | 0.29 / 0.42 |
| Test | Upward Gain | Downward Gain |
|---|---|---|
| 0.2 Hz V | 0.61 / 0.57 | 0.35 / 0.40 |
| 0.4 Hz V | 0.35 / 0.21 | 0.24 / 0.22 |
Normal smooth pursuit gain = 0.9–1.0 (at low frequencies <20°/s)
Interpretation:
- Severely reduced bilateral smooth pursuit gain — all values well below 0.9
- Reduction is symmetric (both eyes, both directions, both horizontal and vertical)
- Gain drops further at higher frequencies (0.4 Hz) — shows central tracking failure
- This is not peripheral — peripheral lesions do not cause bilateral symmetric smooth pursuit failure
- Location: Cerebellar (paraflocculus, vestibulocerebellum), pontine nuclei, or cortical (but given DDK affected, cerebellar most likely)
🔑 Key: Bilateral symmetric smooth pursuit gain <0.5 at 0.2 Hz = Central — cerebellar/brainstem
3. OPTOKINETIC TEST (OKN)
| Direction | Right Eye Gain | Left Eye Gain | FPD |
|---|---|---|---|
| L→R (10°) | 0.94 | 0.79 | Absent |
| R→L (10°) | 1.09 | 0.97 | Absent |
| Top→Bottom | 0.81 | 0.90 | 67.77° (R eye only) |
| Bottom→Top | 1.00 | 1.06 | 299.72° (R eye only) |
Interpretation:
- Horizontal OKN gain is relatively preserved (0.79–1.09) — better than smooth pursuit at same speeds
- Vertical OKN gain reduced (0.81–1.06, with absent fast phase in left eye for Top→Bottom)
- The asymmetry in vertical OKN fast phase (present only in right eye for vertical) suggests unilateral defect in the saccadic generator for vertical OKN — a subtle central finding
- No OKAN (optokinetic after-nystagmus) data, but the velocity storage mechanism can be inferred as partially impaired
4. SPONTANEOUS NYSTAGMUS
| Condition | H-SPV | V-SPV | FPD | Freq |
|---|---|---|---|---|
| In Light | — | — | — | — (absent) |
| In Dark | 2.05°/s (R eye) | — | — | 0.58 Hz |
Interpretation:
- No spontaneous nystagmus in light (fixation suppresses it — normal)
- Low-amplitude spontaneous nystagmus in dark (SPV 2.05°/s, amplitude 2.09°) in the right eye only
- SPV >2°/s in dark is borderline significant — suggests a slight right-sided vestibular asymmetry OR a central low-grade spontaneous nystagmus
- The fact it is absent in light (well fixation-suppressed) means it is not strongly peripheral
5. HEAD SHAKE NYSTAGMUS
| H-SPV R/L | V-SPV R/L | FPD | Frequency | |
|---|---|---|---|---|
| High Freq Head Shake | -3.49 / -3.73°/s | 4.47 / 3.46°/s | 222.94° / 226.19° | 2.20 / 2.19 Hz |
Interpretation:
- Post–head shake nystagmus (HSN) present with both horizontal AND vertical components
- Horizontal component: leftward slow-phase (fast phase ~222–226°, i.e., toward lower-left) = subtle left-beating HSN → indicates right vestibular deficit (per HSN rule: nystagmus beats away from the lesion)
- Vertical component > horizontal → this is the critical finding — a predominantly vertical or oblique HSN is a central sign (peripheral HSN is purely horizontal)
- Fast phase direction ~222–226° = SW quadrant (left-downward) → mixed horizontal + downbeat component
🔑 Central finding: Vertical/oblique head-shake nystagmus → central vestibular pathology (cerebellar or brainstem)
6. HYPERVENTILATION NYSTAGMUS
| H-SPV R/L | V-SPV | FPD | Freq | |
|---|---|---|---|---|
| Hyperventilation | 2.95 / 1.81°/s | 2.05°/s | 343.96° | 1.49 / 0.48 Hz |
Interpretation:
- Nystagmus provoked by hyperventilation — beats toward 344° (upper-right area)
- Hyperventilation-induced nystagmus (HVIN) is significant if SPV >5°/s; here it is borderline (2.05–2.95°/s)
- However, in the context of central disease, HVIN can unmask vestibular nerve or demyelinating lesions
- Low amplitude, but directionally consistent with right vestibular asymmetry
7. GAZE TEST (With & Without Fixation)
| Position | H-SPV | V-SPV | FPD | Significance |
|---|---|---|---|---|
| Center + fixation | — | — | — | Normal |
| Left + fixation | — | — | — | Normal |
| Right + fixation | — | — | — | Normal |
| Up + fixation | — | — | — | Normal |
| Down + fixation | 5.43°/s (R eye) | — | — | Abnormal |
| Center – fixation | — | — | — | Normal |
| Left – fixation | — | — | — | Normal |
| Up – fixation | H: 2.10°/s | V: 1.72 / 1.79°/s | 315.42° | Abnormal |
| Right – fixation | H: -4.01 / -5.52°/s | V: 3.35 / 2.33°/s | 221–203° | Abnormal |
| Down – fixation | — | — | — | Normal |
Interpretation:
- Gaze-evoked nystagmus (GEN) without fixation, especially in upgaze and rightward gaze
- Upgaze nystagmus without fixation (SPV 1.72–2.10°/s, FPD 315° = upper-left direction) — upbeat component, direction-changing in different gaze positions
- Rightward gaze nystagmus without fixation (H-SPV -4.01 to -5.52°/s, FPD 221° = leftward) — left-beating nystagmus on right gaze
- Down-gaze with fixation: V-SPV 5.43°/s — present even with fixation, which is more significant
- This pattern of direction-changing gaze-evoked nystagmus = central sign (cerebellar/brainstem)
🔑 Key: Bidirectional gaze-evoked nystagmus = central vestibular pathology. In peripheral disease, nystagmus is unidirectional and suppressed by fixation.
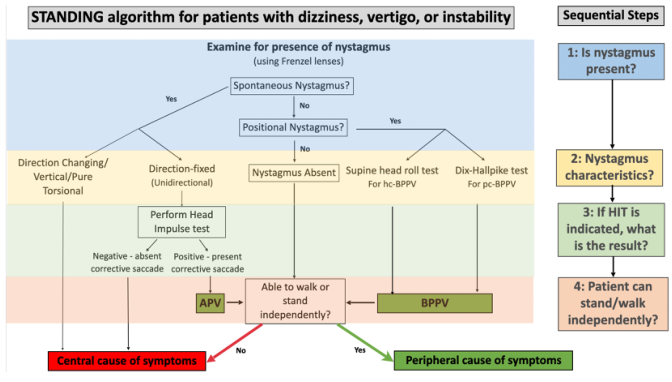
8. POSITIONAL TEST — DIX-HALLPIKE
Right Dix-Hallpike (Supine Head Ext. + Right)
| H-SPV R/L | V-SPV R/L | FPD | Freq | |
|---|---|---|---|---|
| Supine H+R | 3.86 / 2.16°/s | 2.09 / 1.84°/s | 330.27° / 332.81° | 1.37 / 1.20 Hz |
| Sit H+R (recovery) | — / 16.87°/s | -4.55 / -2.87°/s | — / 356.28° | 0.91 / 1.50 Hz |
Fast phase 328–332° = upper-right direction = torsional-upbeat component → this is the direction expected in right posterior canal BPPV. However, the SPV is low (2–4°/s; typically BPPV has SPV >10°/s in the acute phase). The return-to-sitting SPV of 16.87°/s is significant.
Left Dix-Hallpike (Supine Head Ext. + Left) — Two recordings:
| Recording | H-SPV R/L | V-SPV R/L | FPD | Freq |
|---|---|---|---|---|
| First (Sit-L) | -6.26 / -12.77°/s | — | — | 1.32 / 1.04 Hz |
| Supine H+L | -5.73 / -7.01°/s | 8.94 / 10.77°/s | 213.78° / 229.95° | 1.93 / 2.05 Hz |
| Second Sit-L | -3.13 / -10.29°/s | 2.05 / -9.67°/s | 216.57° / 142.79° | 1.40 / 1.99 Hz |
FPD 213–229° = lower-left = downbeat + torsional toward left. This is the expected direction for left posterior canal BPPV in the Hallpike-down position.
Key observations:
- Nystagmus is present bilaterally with both right and left Dix-Hallpike
- The frequencies are high (1.5–2 Hz) and SPVs are moderate
- Geotropic pattern (nystagmus towards ground with both sides during roll test) + bilateral Dix-Hallpike positivity is atypical for classic BPPV
- This could represent cupulolithiasis OR — more importantly — central positional nystagmus (which can mimic BPPV but lacks the typical latency, fatigability, and torsional specificity)
⚠️ Central positional nystagmus: No latency (appears immediately), non-fatigable, variable direction, seen in posterior fossa/cerebellar lesions
9. McCLURE-PAGNINI (SUPINE ROLL) TEST
| Position | H-SPV R/L | V-SPV R/L | FPD (L eye) | Freq |
|---|---|---|---|---|
| Sit→Supine | — | — | — | Normal |
| Right Lateral | — / -12.21°/s | 3.91 / 3.65°/s | 208.38° | 0.70 / 1.21 Hz |
| Supine Neutral (1) | — / -5.68°/s | 3.00 / 2.83°/s | 225.98° | 0.52 / 1.57 Hz |
| Left Lateral | — / -5.25°/s | 4.09 / 4.77°/s | 233.92° | 0.61 / 1.44 Hz |
| Supine Neutral (2) | 1.84°/s / — | 2.96 / 2.72°/s | 303.89° | 0.98 / 0.31 Hz |
FPD consistently around 208–234° (lower-left direction) in multiple positions. This means the nystagmus direction is consistent across positions, not changing with laterality — this is a central positional nystagmus pattern, not the geotropic/ageotropic direction-changing pattern of horizontal canal BPPV.
🔑 Direction-consistent positional nystagmus across multiple positions = CENTRAL, not BPPV
10. HEAD POSITION TEST (Yaw/Pitch/Roll)
| Position | H-SPV | V-SPV | FPD | Comment |
|---|---|---|---|---|
| Yaw Right | -6.62°/s (R eye) | — | — | Left-beating in right head position |
| Yaw Left | -1.94 / +21.54°/s | 2.99 / 3.59°/s | 236.50 / 344.45° | Strong nystagmus in left ear down |
| Pitch Forward | — | 6.54 / 13.48°/s | — | Vertical nystagmus on forward pitch |
| Pitch Backward | — / -4.59°/s | 2.54°/s / — | — | Mild vertical |
| Roll Right | -15.75 / -6.53°/s | -3.86 / 2.50°/s | 167.87° / 225.55° | Strong H+V nystagmus |
| Roll Left | — / -0.32°/s | — / -2.05°/s | 109.38° | Mild |
Critical findings:
- Yaw Left: L eye H-SPV 21.54°/s, FPD 344° (upper-right) — strong right-beating nystagmus with head turned left = right canal paresis finding OR apogeotropic horizontal canal pattern
- Pitch Forward: V-SPV 13.48°/s (vertical nystagmus on head pitch) — anterior/posterior canal pathology or central
- Roll Right: H-SPV -15.75°/s, FPD 167–225° — strongest positional response throughout the test
11. SUBJECTIVE VISUAL VERTICAL (SVV)
| Trial | Deviation | Direction |
|---|---|---|
| Clockwise | 0° | Normal |
| Anticlockwise | -14° (Left) | Clockwise |
| Blank Background | 0° | Normal |
Interpretation:
- SVV tilted -14° in one condition — significant deviation (normal ≤2.5°)
- SVV tilt indicates otolith (utricle) dysfunction or central (brainstem/cerebellar) tilted internal vertical estimate
- A 14° deviation is substantial — suggests either right otolith (utricular) dysfunction (causing leftward tilt of perceived vertical) OR — given all other central signs — a central graviceptive pathway disturbance
- This correlates with the Romberg tilt to right and subjective push sensation
🔑 SVV deviation + push sensation = Ocular tilt reaction (OTR) spectrum — strongly suggests graviceptive pathway involvement (utricle → inferior olive → cerebellum or brainstem)
VNG SUMMARY TABLE
| Test | Result | Significance |
|---|---|---|
| Saccades | Bilateral dysmetria, prolonged latency | Central — cerebellar |
| Smooth Pursuit | Severely reduced bilateral (0.29–0.65) | Central — cerebellar/brainstem |
| OKN | H-preserved, V-asymmetric | Central subtle |
| Spontaneous (dark) | Low-grade right eye nystagmus | Mild right vestibular tone asymmetry |
| Head Shake | Oblique/vertical HSN | Central sign |
| Hyperventilation | Low-grade HVIN | Central-peripheral mixed |
| Gaze (no fixation) | Bidirectional GEN, up+right | Central — cerebellar |
| Gaze (down+fixation) | V-SPV 5.43°/s | Abnormal — central |
| Dix-Hallpike | Bilateral, moderate SPV | Central positional nystagmus |
| Roll test | Direction-consistent nystagmus | Central, not BPPV |
| Head position | Strong Yaw-L + Pitch-F response | Right otolith/canal asymmetry |
| SVV | -14° left | Otolith/central graviceptive |
MRI RECOMMENDATIONS & EXPECTED FINDINGS
Based on this VNG pattern, the following MRI protocol is essential:
What to Order:
MRI Brain with Gadolinium — Focused Posterior Fossa Protocol:
- T1 with/without contrast
- T2/FLAIR
- DWI (to rule out acute infarct)
- SWI (microbleeds, vascular)
- 3D FIESTA/CISS (inner ear, cranial nerves)
- T2 sagittal midline (cerebellar vermis)
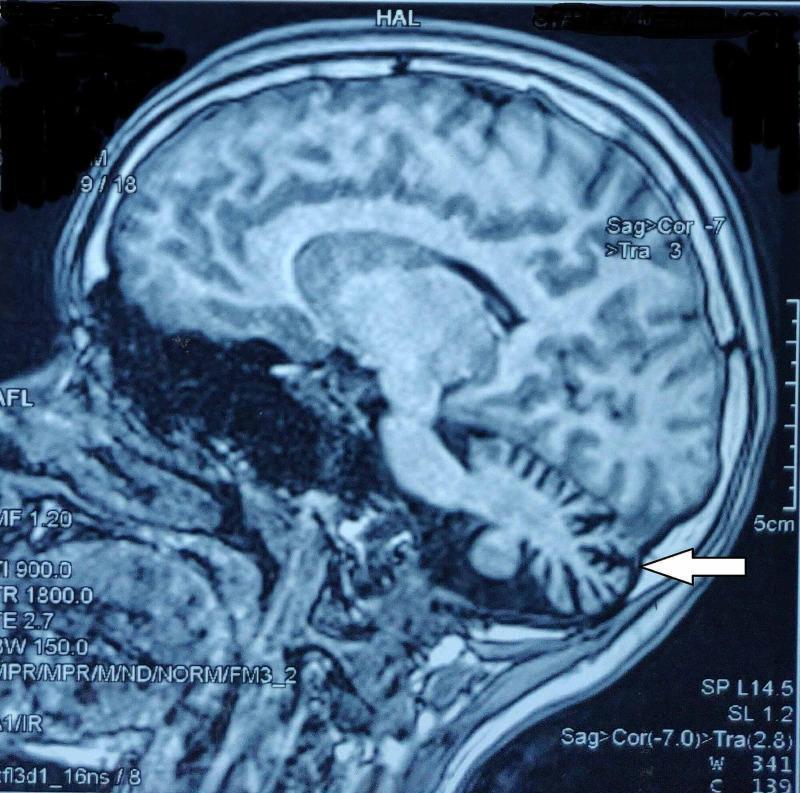
Expected Findings in this Patient:
Most likely:
- Cerebellar atrophy — particularly vermis and flocculonodular lobe (gait ataxia + positional nystagmus)
- Pontocerebellar atrophy — if DDK is bilateral
- Microangiopathic white matter changes (given age 75, hypertension risk)
Differentials on MRI:
- Bilateral white matter hyperintensities (vascular/Binswanger) — can cause central imbalance
- Posterior fossa tumor (rare at this age — meningioma, ependymoma)
- MSA-C (Multiple System Atrophy – Cerebellar type): "hot cross bun sign" in pons on T2
- SCA (Spinocerebellar Ataxia): cerebellar >> brainstem atrophy
DIAGNOSIS
Working Diagnosis:
CENTRAL VESTIBULAR SYNDROME — CEREBELLAR ORIGIN
With secondary bilateral peripheral vestibular asymmetry (right > left)
Differential Diagnoses (in order of probability):
| # | Diagnosis | Supporting Evidence |
|---|---|---|
| 1 | Cerebellar Degeneration (Late-onset) — sporadic or vascular | Age 75, DDK+, tandem gait+, bilateral smooth pursuit failure, bilateral saccadic dysmetria, central positional nystagmus, SVV tilt |
| 2 | MSA-C (Multiple System Atrophy – Cerebellar) | Age, progressive imbalance, autonomic features (urinary hesitancy in prescription!), no clear vestibular vertigo |
| 3 | Vascular cerebellar ataxia (multi-infarct / chronic ischemia) | Age 75, gradual progressive falls, bilateral SNHL |
| 4 | SCA (Spinocerebellar Ataxia) | Oculomotor findings similar to SCA1/SCA2/SCA3 (image above), but usually presents earlier in life |
| 5 | Normal Pressure Hydrocephalus (NPH) | Triad: gait apraxia (cannot lift feet) + urinary symptoms (seen in prescription) + cognition — MRI needed |
⚠️ RED FLAG — Look at the Prescription:
The psychiatric prescription mentions:
- Fear of voiding urine, hesitancy in passing urine → autonomic urinary dysfunction
- Disturbed sleep, decreased confidence → autonomic/central
Urinary dysfunction + cerebellar ataxia + gait imbalance in a 75-year-old = MSA-C or NPH until proven otherwise.
CORRELATION: Clinical Signs → Anatomical Localization
| Clinical Finding | Anatomical Correlate |
|---|---|
| Romberg + (falls backward-right) | Right vestibulospinal pathway |
| Fukuda >1m deviation | Right labyrinthine/vestibular nuclear asymmetry |
| Tandem gait failure | Cerebellar vermis / spinocerebellar tracts |
| DDK affected | Cerebellar hemisphere (ipsilateral) |
| Forward push sensation | Graviceptive pathway (otolith → cerebellum) |
| Conscious falls (face-down) | Severe cerebellar gait ataxia — "cerebellar lunges" |
| No vertigo/dizziness | Against peripheral — pure imbalance = cerebellar |
| Bilateral SNHL (sloping) | Cochlear (age-related / vascular) — separate |
| SVV -14° | Utricle or graviceptive central pathway |
MANAGEMENT PLAN
Immediate:
- MRI Brain with gadolinium — posterior fossa focus (urgent)
- Neurology referral — to rule out MSA-C, NPH, SCA
- CT Brain if MRI not immediately available (to rule out hemorrhage/mass)
Investigations:
- Blood: CBC, LFT, RFT, thyroid (TSH), B12, folate, HbA1c, VDRL
- Genetic panel: SCA1/2/3/6/7 (if family history or younger onset)
- Urodynamics / urological evaluation (given urinary symptoms)
- VEMP (cVEMP + oVEMP) — to assess otolith function directly
- vHIT — to assess semicircular canal VOR (not done here)
Vestibular Rehabilitation:
- Gaze stabilization exercises (smooth pursuit + saccade retraining)
- Balance training (static + dynamic, Cawthorne-Cooksey modified)
- Fall prevention program — high priority (conscious falls, face-down)
Medication:
- Current Restonorm (clonazepam 0.5 mg HS) — appropriate for anxiety + can reduce vestibular excitability at night
- Betahistine — limited value in central disease but may help peripheral component
- Vitamin D + Calcium — fall prevention in elderly
- Avoid vestibular suppressants (meclizine, cinnarizine) — counterproductive in cerebellar disease
FINAL DIAGNOSTIC IMPRESSION
VNG IMPRESSION:
1. CENTRAL OCULOMOTOR DYSFUNCTION
- Bilateral saccadic dysmetria with prolonged latency
- Severely reduced bilateral smooth pursuit (cerebellar pattern)
- Bidirectional gaze-evoked nystagmus without fixation
2. CENTRAL POSITIONAL NYSTAGMUS
- Direction-consistent across positions (not BPPV)
- Bilateral Dix-Hallpike positive (no fatigability pattern)
3. VERTICAL/OBLIQUE HEAD-SHAKE NYSTAGMUS
- Indicates central vestibular pathology
4. OTOLITH DYSFUNCTION
- SVV deviated -14° (right > left utricular)
- Push sensation, Romberg tilt right
5. MILD RIGHT PERIPHERAL VESTIBULAR ASYMMETRY
- Yaw-Left: strong right-beating nystagmus (right canal/nerve)
- Head-Shake: horizontal component leftward (right loss)
CONCLUSION:
Central Vestibular Syndrome, cerebellar pattern
DDx: Cerebellar degeneration, MSA-C, NPH
Recommend: MRI Brain (posterior fossa), Neurology referral
⚕️ Clinical Note: This patient is a 75-year-old male with conscious falls (face-down, knowing he is about to fall) — this is classic cerebellar gait ataxia (not syncopal, not vestibular drop attacks). The complete VNG shows a consistent central cerebellar pattern. The urinary hesitancy documented by the psychiatrist is a critical additional clue pointing toward MSA-C. MRI is urgently needed.
Have you given detailed VNG analysis ?
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.