Cerebellopontine angle in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
"cerebellopontine angle" AND (tumor OR schwannoma OR meningioma)
Searching the Web
cerebellopontine angle anatomy tumors management RGUHS ENT 20 marks
Finding Sources
Searching PubMed
"vestibular schwannoma" AND (radiosurgery OR "watchful waiting" OR microsurgery)
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
CEREBELLOPONTINE ANGLE (CPA) - Comprehensive 20-Mark Answer
Sources: Scott-Brown's Vol 2, Cummings Otolaryngology, Shambaugh Surgery of the Ear, Adams & Victor's Neurology, Bradley & Daroff's Neurology, Bailey & Love's Surgery, Harrison's Internal Medicine; supplemented by recent PubMed evidence (2023-2026)
DIAGRAM 1: ANATOMY OF THE CEREBELLOPONTINE ANGLE
(Scott-Brown's Vol 2, Figure 111.12 - reproduced below)
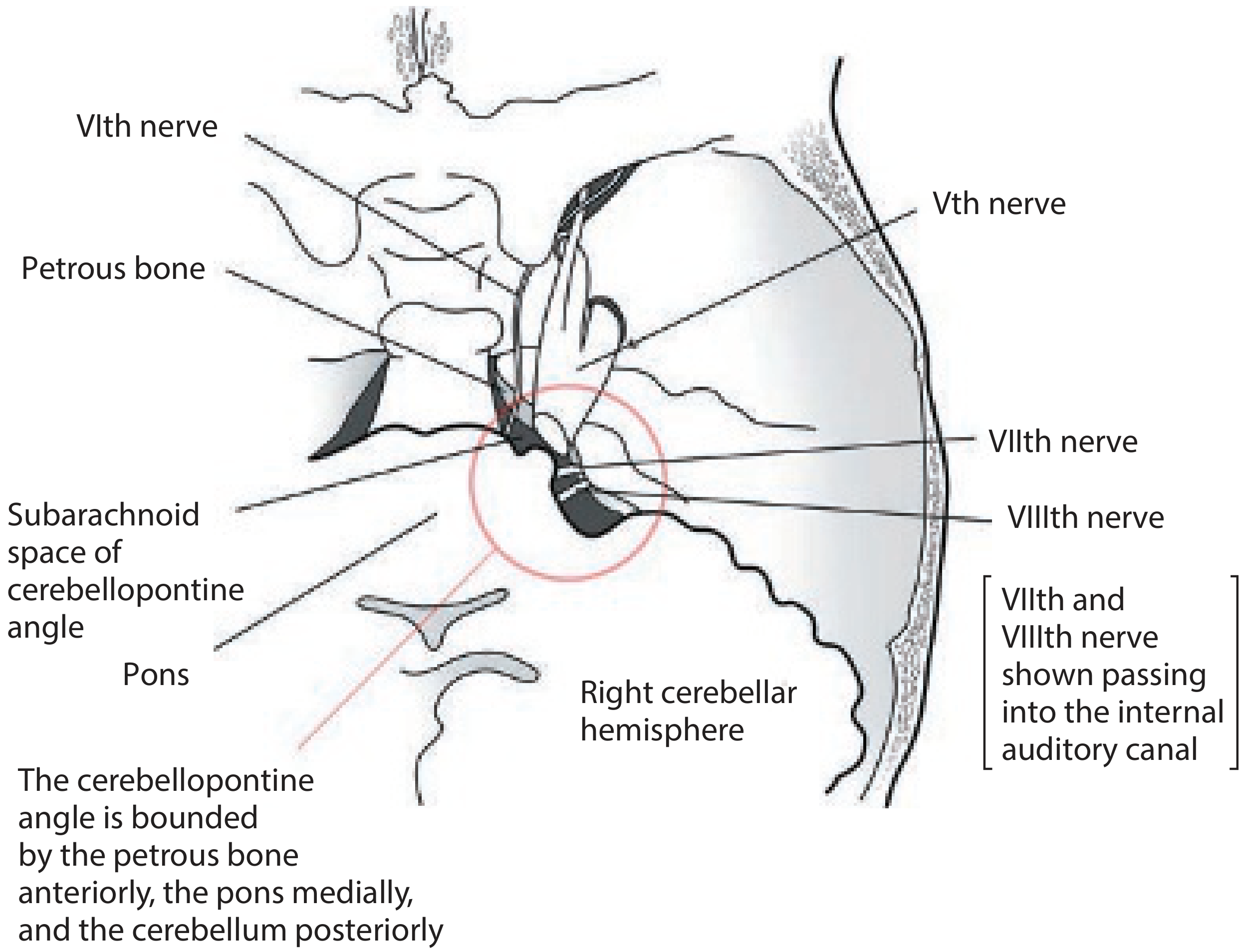
Fig. The CPA is bounded by the petrous bone anteriorly, the pons medially, and the cerebellum posteriorly. CN VII and VIII pass into the internal auditory canal. CN V is the superior boundary; CN IX, X, XI form the inferior boundary.
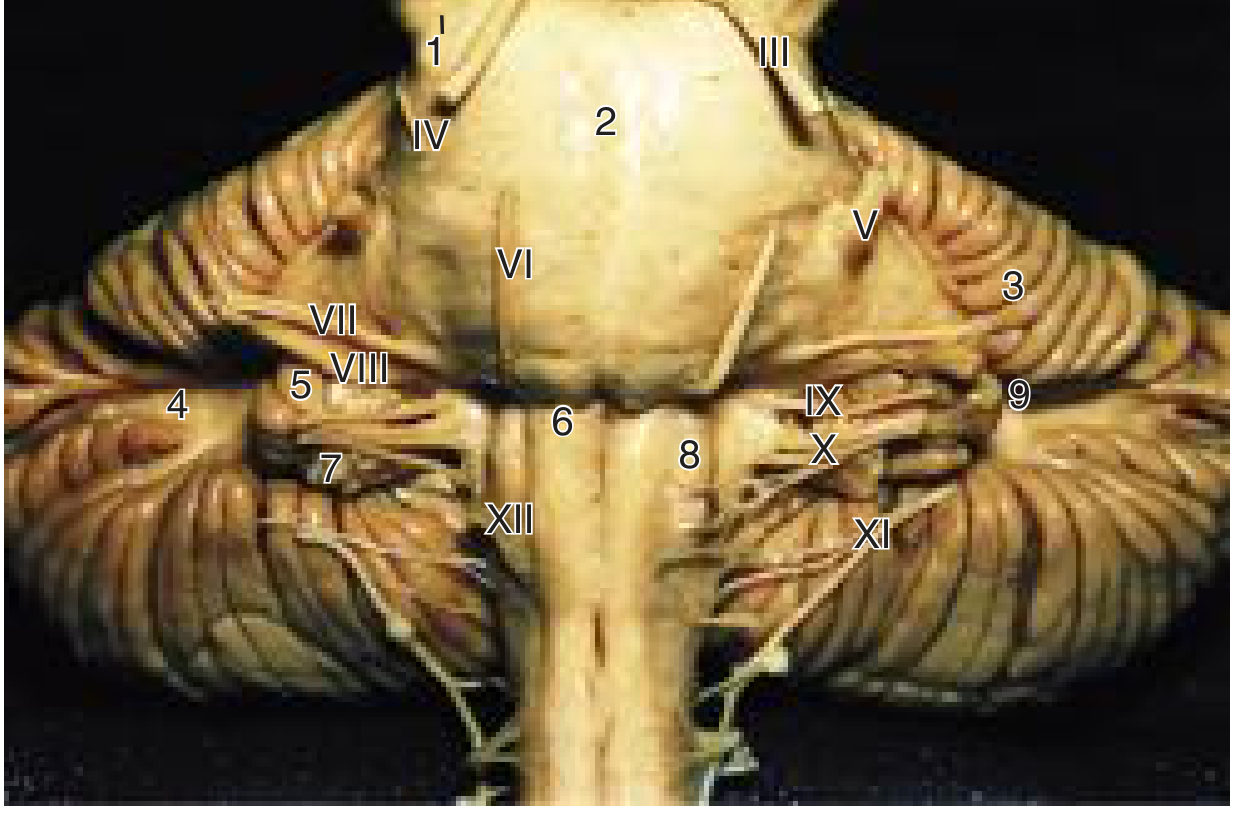
Fig. Anterior (rostral) view of the brainstem: CN VI, VII, VIII exit at the pontomedullary sulcus; CN V at the mid-pons; CN IX, X, XI at the medulla. (Cummings Otolaryngology)
1. DEFINITION AND OVERVIEW
The cerebellopontine angle (CPA) is a triangular cistern in the posterior cranial fossa containing a complex interface between the central and peripheral nervous systems. It is filled with CSF (the CPA cistern) and is one of the most surgically challenging regions in the skull base.
[Cummings Otolaryngology, p. 3425] The CPA is delimited as follows:
- Anteriorly - CN VI and the lateral aspect of the clivus
- Laterally - the medial surface of the petrosa (petrous bone)
- Medially - middle cerebellar peduncle, pons, and ventral surface of cerebellum
- Superiorly - CN V (trigeminal nerve)
- Inferiorly - CN IX, X, and XI
- Posteriorly - the cerebellar flocculus
2. ANATOMICAL CONTENTS
┌─────────────────────────────────────────────────┐
│ CONTENTS OF THE CPA CISTERN │
├─────────────────────────────────────────────────┤
│ NERVES (traversing the cistern): │
│ • CN V - Trigeminal (superior) │
│ • CN VI - Abducens (anteromedial) │
│ • CN VII - Facial nerve │
│ • CN VIII - Vestibulocochlear (VII lies 1-2mm │
│ anteroinferior to VIII) │
│ • CN IX, X, XI - Lower (inferior boundary) │
│ │
│ ARTERIES: │
│ • AICA (Anterior Inferior Cerebellar Artery) │
│ - Pre-meatal, meatal, and post-meatal segs │
│ - Loops into the IAC in 40% of cases │
│ • Labyrinthine (internal auditory) artery │
│ - Branch of AICA or PICA (basilar rarely) │
│ │
│ VEINS: │
│ • Petrosal vein (of Dandy) │
│ • Drains into superior petrosal sinus │
└─────────────────────────────────────────────────┘
[Scott-Brown's Vol 2, p. 4844] CN VII lies 1 to 2 mm anteroinferior to CN VIII as they travel from the bulbopontine sulcus toward the IAC, both following a lateral and ascending course.
3. INTERNAL AUDITORY CANAL (IAC)
The IAC measures approximately 1.2 to 1.4 cm from the porus acusticus to the fundus.
FUNDUS OF IAC (cross-section - 4 quadrants)
════════════════════════════════════════════
Superior compartment │ Superior compartment
ANTERIOR │ POSTERIOR
───────────────────── │ ─────────────────────
FACIAL NERVE (VII) │ SUPERIOR VESTIBULAR N.
+ Nervus intermedius │
════════════ BILL'S BAR (vertical crest) ══════
─ ─ ─ ─ ─ ─ FALCIFORM/TRANSVERSE CREST ─ ─ ─ ─
Inferior compartment │ Inferior compartment
ANTERIOR │ POSTERIOR
───────────────────── │ ─────────────────────
COCHLEAR NERVE (VIII) │ INFERIOR VESTIBULAR N.
[Cummings, p. 2797] "Bill's bar" - named after William House - is the vertical crest separating facial nerve (anterosuperior) from superior vestibular nerve (posterosuperior). The falciform (transverse) crest separates superior from inferior compartments.
4. CLASSIFICATION OF CPA LESIONS
┌──────────────────────────────────────────────────────────────┐
│ CLASSIFICATION OF CPA LESIONS │
│ (Cummings / Scott-Brown / Adams & Victor) │
├──────────────────────────────────────────────────────────────┤
│ COMMON (>95%) │
│ 1. Vestibular Schwannoma (Acoustic Neuroma) - 80-90% │
│ 2. Meningioma - ~10-18% │
│ 3. Epidermoid cyst (Primary Cholesteatoma) - ~2.5% │
├──────────────────────────────────────────────────────────────┤
│ LESS COMMON │
│ 4. Facial nerve schwannoma - ~1% │
│ 5. Arachnoid cyst │
│ 6. Paraganglioma/Glomus jugulare - up to 10% │
│ (when secondary tumors counted) │
│ 7. Trigeminal schwannoma │
│ 8. Dermoid cyst / Lipoma │
│ 9. PICA/AICA aneurysm or vascular loop │
│ 10. Pontine glioma (age 5-15 yrs) │
│ 11. Cerebellar medulloblastoma │
│ 12. Metastases (lung, breast, melanoma) │
│ 13. Pilocytic astrocytoma (rare in adults) │
│ 14. NF2-related bilateral schwannomas │
└──────────────────────────────────────────────────────────────┘
[Cummings, p. 3428]: "Acoustic neuromas account for more than 90% of CPA neoplasms. Remaining primary tumors: meningiomas 3%, primary cholesteatomas 2.5%, facial nerve schwannomas 1%."
5. VESTIBULAR SCHWANNOMA - DETAILED DESCRIPTION
5a. Pathology and Origin
- Benign schwannoma of CN VIII - predominantly arises from the inferior vestibular nerve (not at the Obersteiner-Redlich zone as once thought - Xenellis & Linthicum)
- Arise from Schwann cells in a collagenous matrix; circumscribed, displacing but not invading neural tissue
- Gross appearance: yellow to gray; cystic variants may show hemorrhage/necrosis
- Histology: Antoni A (compact spindle cells in palisades = Verocay bodies) and Antoni B (loose myxoid) patterns
[Shambaugh Surgery of the Ear, p. 3346]: First observed at autopsy in 1777; Sir Charles Bell published first clinical case report.
5b. Natural History and Growth
[Cummings, p. 3429]:
- Average growth rate: 0.2 cm/year (range: spontaneous regression to >2 cm/year)
- Three phases of growth:
- Compression of IAC - acoustic and facial nerve compression
- Cisternal phase - displacement of CN VII, VIII, AICA
- Brainstem compression - 4th ventricle shift at 2-3 cm; hydrocephalus with further growth; trigeminal compression at ~3 cm
KOOS GRADING (Tumor Staging)
┌────────────────────────────────────────────────────────┐
│ KOOS GRADING SYSTEM FOR VESTIBULAR │
│ SCHWANNOMA │
├──────┬───────────────────────────────────────────────┤
│Grade │ Description │
├──────┼───────────────────────────────────────────────┤
│ I │ Intracanalicular (confined to IAC) │
├──────┼───────────────────────────────────────────────┤
│ II │ Into CPA, <2 cm, no brainstem contact │
├──────┼───────────────────────────────────────────────┤
│ III │ Into CPA, 2-3 cm, brainstem contact but │
│ │ no displacement │
├──────┼───────────────────────────────────────────────┤
│ IV │ >3 cm, brainstem displacement, 4th ventricle │
│ │ compression │
└──────┴───────────────────────────────────────────────┘
6. CPA SYNDROME - CLINICAL FEATURES
[Scott-Brown's Vol 2, p. 4846-4871; Localization in Clinical Neurology, p. 2057-2063]
┌──────────────────────────────────────────────────────────────┐
│ CPA SYNDROME - CLINICAL FEATURES │
├────────────────────────┬─────────────────────────────────────┤
│ NERVE INVOLVED │ SYMPTOMS / SIGNS │
├────────────────────────┼─────────────────────────────────────┤
│ CN VIII (Cochlear) │ Unilateral SNHL (progressive) │
│ │ Tinnitus (high-pitched) │
│ │ Poor speech discrimination │
│ │ Absent/abnormal ABR (Wave V delay) │
├────────────────────────┼─────────────────────────────────────┤
│ CN VIII (Vestibular) │ Imbalance (NOT true vertigo) │
│ │ Gradual - centrally compensated │
├────────────────────────┼─────────────────────────────────────┤
│ CN VII (Facial) │ Facial hemispasm (early) │
│ │ Facial palsy (late/large tumors) │
│ │ Loss of taste (anterior 2/3 tongue) │
├────────────────────────┼─────────────────────────────────────┤
│ CN V (Trigeminal) │ Impaired corneal reflex (EARLIEST │
│ │ sensitive sign of CPA tumor) │
│ │ Facial numbness, trigeminal neuralgia│
├────────────────────────┼─────────────────────────────────────┤
│ CN VI (Abducens) │ Diplopia (large tumors) │
├────────────────────────┼─────────────────────────────────────┤
│ CN IX, X, XI │ Dysphagia, hoarseness │
│ (Lower cranial nerves) │ (indicates very large tumors or │
│ │ jugular foramen involvement) │
├────────────────────────┼─────────────────────────────────────┤
│ Cerebellum/Brainstem │ Ataxia, nystagmus, headache │
│ compression │ Raised ICP, hydrocephalus │
│ │ (late - Koos grade IV) │
└────────────────────────┴─────────────────────────────────────┘
Key point [Scott-Brown's]: Gradual SNHL is the rule; facial palsy as a presenting symptom suggests cholesteatoma or meningioma rather than vestibular schwannoma. Impaired corneal reflex is the most sensitive early sign of CPA tumor extension.
7. INVESTIGATIONS - DIAGNOSTIC FLOWCHART
SUSPECTED CPA LESION
(Unilateral SNHL + tinnitus ± imbalance)
│
▼
┌───────────────────┐
│ PURE TONE AUDIOMETRY│
│ + Speech Discrimination│
│ (PTA + SDS) │
└─────────┬─────────┘
│
▼
┌──────────────────────────┐
│ IMPEDANCE AUDIOMETRY │
│ - Tympanogram (Type A) │
│ - Acoustic reflexes: │
│ Absent ipsilateral reflex│
│ = CN VIII lesion │
│ (retrocochlear pattern)│
└──────────┬───────────────┘
│
▼
┌──────────────────────────┐
│ ABR (BERA) │
│ - Prolonged I-III, I-V │
│ interpeak latency │
│ - Wave V absent │
│ - Interaural delay >0.3ms│
│ (Screening tool) │
└──────────┬───────────────┘
│
Abnormal ABR or high suspicion
│
▼
┌──────────────────────────────────────────┐
│ MRI BRAIN WITH GADOLINIUM │
│ (GOLD STANDARD - Cummings p. 2111) │
│ │
│ T1+Gd: Enhancing lesion in IAC/CPA │
│ T2/CISS: Shows tumor vs CSF detail │
│ DWI: Epidermoid shows RESTRICTED │
│ DIFFUSION (bright on DWI) │
└──────────────────────────────────────────┘
│
▼
┌──────────────────────────────────────────────────────────┐
│ IMAGING FEATURES (Cummings Table 179.2) │
├──────────────┬────────────────┬───────────────────────── │
│ Feature │ Schwannoma │ Meningioma │ Epidermoid│
├──────────────┼────────────────┼─────────────┼───────────│
│ Location │ Centered on IAC│ Eccentric │ Anterolat │
│ IAC widening │ YES │ NO │ NO │
│ Bone change │ IAC enlargement│ Hyperostosis│ Erosion │
│ T1 Gd │ Marked enhance │ Moderate │ None │
│ T2 │ Iso/hyperint │ Variable │ Hyperint │
│ DWI │ Normal │ Normal │ BRIGHT │
│ Dural tail │ Absent │ PRESENT │ Absent │
└──────────────┴────────────────┴─────────────┴───────────┘
HRCT Temporal Bone: Shows IAC widening, bony erosion patterns. Less sensitive than MRI but important for surgical planning.
OAEs (DPOAEs): Normal OAEs with abnormal ABR = retrocochlear lesion (CPA) rather than cochlear. (Shambaugh case study - miliary TB causing CPA disorder)
8. MANAGEMENT - COMPREHENSIVE FLOWCHART
CPA TUMOR DIAGNOSED ON MRI
│
┌──────┴────────┐
│ │
Vestibular Other CPA
Schwannoma lesions
│
▼
MULTIDISCIPLINARY TEAM DECISION
(Neurotologist + Neurosurgeon + Radiation Oncologist)
│
┌───────┼───────────┐
│ │ │
▼ ▼ ▼
OBSERVE RADIOSURGERY MICROSURGERY
(Watch & (SRS/SRT)
Scan)
│
├── Indications: ├── Indications: ├── Indications:
│ • Age >70 yrs │ • Koos I-III │ • Any size
│ • Small tumor │ • <3 cm │ • Young patient
│ • Elderly/unfit │ • No hydrocephalus │ • Large (Koos IV)
│ • No/slow growth │ • Residual/recurrent │ • Hearing preservation goal
│ │ │ • Cystic schwannoma
├── Protocol: ├── Types: │
│ Serial MRI: │ • Gamma Knife (GK) │
│ 6-monthly x2 yrs │ • CyberKnife │
│ then annually │ • Fractionated SRT │
│ │ Dose: 12-13 Gy (GK) │
└──────────────────────────────────────────────── ┘
9. SURGICAL APPROACHES - COMPARISON TABLE
[Cummings Table 178.4; Shambaugh Surgery of the Ear]
┌────────────────┬──────────────────────┬───────────────────┬──────────────────────┐
│ APPROACH │ INDICATIONS │ ADVANTAGES │ DISADVANTAGES │
├────────────────┼──────────────────────┼───────────────────┼──────────────────────┤
│TRANSLABYRINTHINE│ Any size CPA tumor │ Wide exposure; │ Permanent hearing │
│ │ (large, medium, small)│ no cerebellum │ loss (sacrifices │
│ │ Non-serviceable │ retraction; facial│ labyrinth); fat graft│
│ │ hearing │ nerve ID at both │ needed │
│ │ │ CPA end and fundus│ │
├────────────────┼──────────────────────┼───────────────────┼──────────────────────┤
│RETROSIGMOID │ Any size; good or │ Hearing │ Cerebellar retraction│
│(Suboccipital/ │ poor hearing; │ preservation │ needed; limited IAC │
│Posterior fossa)│ Meningioma; Koos III│ possible; useful │ visualization medially│
│ │ - IV │ for all pathology │ Headache (post-op) │
├────────────────┼──────────────────────┼───────────────────┼──────────────────────┤
│MIDDLE FOSSA │ Intracanalicular/ │ Hearing │ Small tumors ONLY; │
│ │ small tumors; │ preservation; │ temporal lobe │
│ │ GOOD hearing; │ best facial nerve │ retraction; elderly │
│ │ Koos I-II │ preservation │ not tolerated well │
│ │ │ for small tumors │ │
├────────────────┼──────────────────────┼───────────────────┼──────────────────────┤
│EXTENDED MIDDLE │ Petroclival tumors; │ Improved access │ Complex; SPS ligation│
│FOSSA │ substantial CPA ext.│ to posterior fossa│ required; temporal │
│ │ with serviceable │ │ lobe retraction │
│ │ hearing │ │ │
└────────────────┴──────────────────────┴───────────────────┴──────────────────────┘
[Shambaugh, p. 4024]: "A relative advantage of the translabyrinthine approach over the middle fossa and suboccipital approaches is the avoidance of cerebellar or temporal lobe retraction."
10. MENINGIOMA OF THE CPA
[Cummings, p. 3431]
- 3% of CPA tumors; 10-18% of all intracranial tumors
- Origin: arachnoid villi cells, attached to dura mater
- Gross: globular mass adherent to dura, psammoma body speckles
- Key imaging difference from schwannoma:
- Eccentric to IAC (does NOT widen the IAC)
- Dural "tail" sign
- Hyperostosis in 25%
- Homogeneous marked enhancement
- Obtuse bone-tumor angle
11. EPIDERMOID CYST (PRIMARY CHOLESTEATOMA)
[Adams & Victor's Neurology, p. 514; Cummings]
- Arises from ectodermal rests during neural tube closure (3rd-5th week of embryogenesis)
- "Pearly white" appearance - desquamating squamous epithelium
- Classically fills and insinuates around structures ("cauliflower" shape)
- DWI imaging - restricted diffusion (bright) - pathognomonic; distinguishes from arachnoid cyst
- Treatment: surgical excision (tends to recur if capsule not removed)
- Fifth nerve involvement may be the first symptom (unlike schwannoma)
12. DIFFERENTIAL DIAGNOSIS - FLOWCHART
CPA MASS LESION
│
├─── IAC centered + enlarges IAC → VESTIBULAR SCHWANNOMA
│
├─── Eccentric to IAC + dural tail + hyperostosis → MENINGIOMA
│
├─── Bright on DWI + T2 hyperintense + non-enhancing → EPIDERMOID
│
├─── CSF intensity on all sequences + non-enhancing → ARACHNOID CYST
│
├─── Extends to jugular foramen + pulsatile tinnitus → GLOMUS JUGULARE
│
├─── Fat density on CT + T1 bright → LIPOMA
│
├─── Bilateral CPA tumors + family history → NF2
│
├─── Rapid onset + known malignancy → METASTASIS
│
└─── Age 5-15 yrs + brainstem origin → PONTINE GLIOMA/
MEDULLOBLASTOMA
13. COMPLICATIONS OF CPA SURGERY
INTRAOPERATIVE:
• Facial nerve injury (most feared - target: HB Grade I-II)
• Hearing loss
• CSF leak
• Vascular injury (AICA, basilar artery, petrosal vein)
• Lower cranial nerve injury (IX, X, XI) - large tumors
POSTOPERATIVE:
• CSF rhinorrhoea/otorrhoea (fat graft, fibrin glue)
• Meningitis (aseptic or bacterial)
• Hydrocephalus
• Persistent headache (retrosigmoid approach)
• Facial weakness (HB grading used to assess)
• Cerebellar/brainstem contusion
• Pneumocephalus
House-Brackmann (HB) Scale used to grade facial nerve function post-surgery:
- HB Grade I = Normal; HB Grade VI = Complete paralysis
14. RECENT ADVANCES (2023-2026) - RGUHS CONTEXT
a. V-REX Randomized Clinical Trial (JAMA 2023) [PMID: 37526718]
- First RCT comparing upfront radiosurgery vs. wait-and-scan for small/medium vestibular schwannomas
- Found no significant difference in tumor control at short-term; supports watch-and-wait as the initial strategy for small tumors
- A landmark practice-changing trial published in JAMA 2023
b. Clinical Practice Guideline on Vestibular Schwannoma (2024) [PMID: 38346489]
- New systematic review-based guideline recommending individualized management
- Strengthens the role of stereotactic radiosurgery for Koos I-III tumors
- Emphasizes tumor growth monitoring with volumetric MRI
c. Endoscopic-Assisted CPA Surgery
- Endoscopic assistance allows visualization of hidden tumor remnants behind cranial nerves and in IAC fundus without full translabyrinthine exposure
- Reduces residual tumor rates
- Used as a "second-look" intraoperative tool
d. Medical Therapy (Bevacizumab for NF2) [PMID: 41052835]
- Anti-VEGF therapy (bevacizumab) for NF2-associated bilateral schwannomas
- Shown to reduce tumor volume and improve hearing in NF2 patients
- Not indicated for sporadic unilateral schwannoma
e. SMARCB1 and LZTR1 Gene Mutations (Schwannomatosis)
- [Cummings, p. 3430]: Schwannomatosis - multiple schwannomas without NF2 criteria; associated with SMARCB1 and LZTR1 gene loci on chromosome 22
f. Intraoperative Neuromonitoring (IONM)
- Continuous facial nerve EMG monitoring and ABR monitoring during CPA surgery
- Reduces permanent facial nerve injury rates significantly
- Direct electrical stimulation at the brainstem end identifies the nerve before dissection
g. Robotic Radiosurgery (CyberKnife)
- Frameless fractionated stereotactic radiotherapy
- Allows dose fractionation (5 fractions = 25 Gy total) vs. single-fraction Gamma Knife
- Suitable for tumors >3 cm and tumors near cochlea
h. Pilocytic Astrocytoma of CPA in Adults [PMID: 39524593]
- Rare but increasingly recognized CPA lesion in adults
- Systematic review 2024 confirms surgical resection is treatment of choice; good prognosis
15. SUMMARY TABLE - KEY POINTS FOR RGUHS EXAM
| Topic | Key Fact |
|---|---|
| Most common CPA tumor | Vestibular schwannoma (80-90%) |
| Origin | Inferior vestibular nerve near Scarpa's ganglion |
| Earliest sign of CPA tumor | Impaired corneal reflex (CN V compression) |
| Commonest symptom | Progressive unilateral SNHL + tinnitus |
| Gold standard investigation | MRI brain with gadolinium + CISS sequences |
| DWI bright lesion | Epidermoid cyst (restricted diffusion) |
| Dural tail sign | Meningioma |
| IAC widening on CT | Vestibular schwannoma |
| Hearing preservation surgery | Middle fossa or retrosigmoid approach |
| Approach with NO cerebellum retraction | Translabyrinthine |
| Bilateral CPA tumors | NF2 (neurofibromatosis type 2) |
| ABR finding | Prolonged interpeak latency (I-III, I-V), absent Wave V |
| Koos Grade IV treatment | Microsurgery (not SRS) |
| Facial nerve grading | House-Brackmann Scale |
| Recent landmark RCT | V-REX Trial (JAMA 2023) - watch vs. radiosurgery |
BIBLIOGRAPHY / REFERENCES
- Scott-Brown's Otorhinolaryngology HNS Vol 2 - Chapter 111: The CPA Syndrome (pp. 4844-4871)
- Cummings Otolaryngology HNS - Chapter 179: Vestibular Schwannoma and Other CPA Tumors (pp. 3425-3450)
- Shambaugh Surgery of the Ear - Chapter 6: Vestibular Schwannoma (pp. 3346-5443)
- Adams & Victor's Principles of Neurology 12e - Chapter on Other Tumors of the CPA (p. 514)
- Bradley & Daroff's Neurology in Clinical Practice - CPA Tumors (p. 4402-4404)
- Bailey & Love's Short Practice of Surgery 28e - Vestibular Schwannoma (pp. 5070-5091)
- Harrison's Internal Medicine 22e - Vestibular Schwannoma (p. 983)
- Dhingra's Diseases of ENT - CPA anatomy and acoustic neuroma management
- Hazarika's Textbook of ENT - CPA lesions (standard RGUHS reference)
- Zakir Hussain's ENT - CPA syndrome (RGUHS-aligned Indian textbook)
- Lassaletta L et al. Clinical practice guideline on the management of vestibular schwannoma. Acta Otorrinolaringol Esp. 2024 [PMID: 38346489]
- Dhayalan D et al. V-REX Randomized Clinical Trial. JAMA. 2023 [PMID: 37526718]
- Bruzzaniti P et al. Cerebellopontine angle pilocytic astrocytoma in adults: systematic review. Surg Neurol Int. 2024 [PMID: 39524593]
- Evans DG, Plotkin SR. Medical therapy for vestibular schwannoma. Handb Clin Neurol. 2025 [PMID: 41052835]
Note for RGUHS students: The examiners expect you to quote Dhingra (6th/7th ed), Hazarika, and Scott-Brown's together. The CPA syndrome = unilateral SNHL + absent corneal reflex + ± facial palsy is the classic triad to memorize. Surgical approach selection (translabyrinthine vs. middle fossa vs. retrosigmoid) is a high-yield comparison question. The V-REX trial (JAMA 2023) is the most important recent advance for this topic.
This is a shared conversation. Sign in to Orris to start your own chat.