Give me DNB Distinction type answer for Laryngeal nerve supply with vocal cord palsy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Waiting for the answer
I have all the information needed from the textbooks. Here is the comprehensive DNB Distinction-level answer:
Nerve Supply of the Larynx with Vocal Cord Palsy
NERVE SUPPLY OF THE LARYNX
The larynx receives its nerve supply entirely from two branches of the vagus nerve (CN X):
- Superior Laryngeal Nerve (SLN)
- Recurrent Laryngeal Nerve (RLN)
I. SUPERIOR LARYNGEAL NERVE (SLN)
Origin & Course
- Arises from the inferior (nodose) ganglion of the vagus nerve
- Descends medial to the internal carotid artery
- Divides into internal and external branches 2–3 cm above the superior pole of the thyroid gland, near the level of the hyoid bone
Branches
| Branch | Type | Function |
|---|---|---|
| Internal branch | Sensory (GVA + SVA) | Pierces the thyrohyoid membrane; sensation to supraglottic larynx, glottis (above vocal cords), lower pharynx, base of tongue, epiglottic taste buds |
| External branch | Motor (branchial efferent) | Supplies cricothyroid muscle and inferior pharyngeal constrictor; increases vocal fold tension → high-frequency phonation |
Clinical pearl: The external branch travels along the inferior constrictor and has a close relationship with the superior thyroid pole vessels. In ~15–20% of cases, it crosses directly over thyroid parenchyma, placing it at risk during ligation of the superior thyroid pole. — KJ Lee's Essential Otolaryngology
II. RECURRENT LARYNGEAL NERVE (RLN)
Motor Nucleus
- Nucleus ambiguus (in medulla oblongata)
Function
- Motor (branchial efferent): All intrinsic laryngeal muscles except cricothyroid
- Sensory (GVA): Laryngeal mucosa below vocal cords, subglottis, upper trachea, upper oesophagus
- Parasympathetic: Lower pharynx, larynx, trachea, upper oesophagus
Muscles Supplied by RLN
| Muscle | Action |
|---|---|
| Posterior cricoarytenoid (PCA) | Sole abductor of vocal cord |
| Lateral cricoarytenoid (LCA) | Adductor |
| Thyroarytenoid (TA/vocalis) | Adductor, shortens/relaxes cord |
| Interarytenoid (IA) | Adductor; receives bilateral innervation |
| Aryepiglottis | Adductor |
Note: The interarytenoid muscle receives bilateral innervation from both RLNs — clinically significant in unilateral palsy. — KJ Lee's Essential Otolaryngology
III. COURSE OF THE RLN (Left vs Right — Key Exam Distinction)
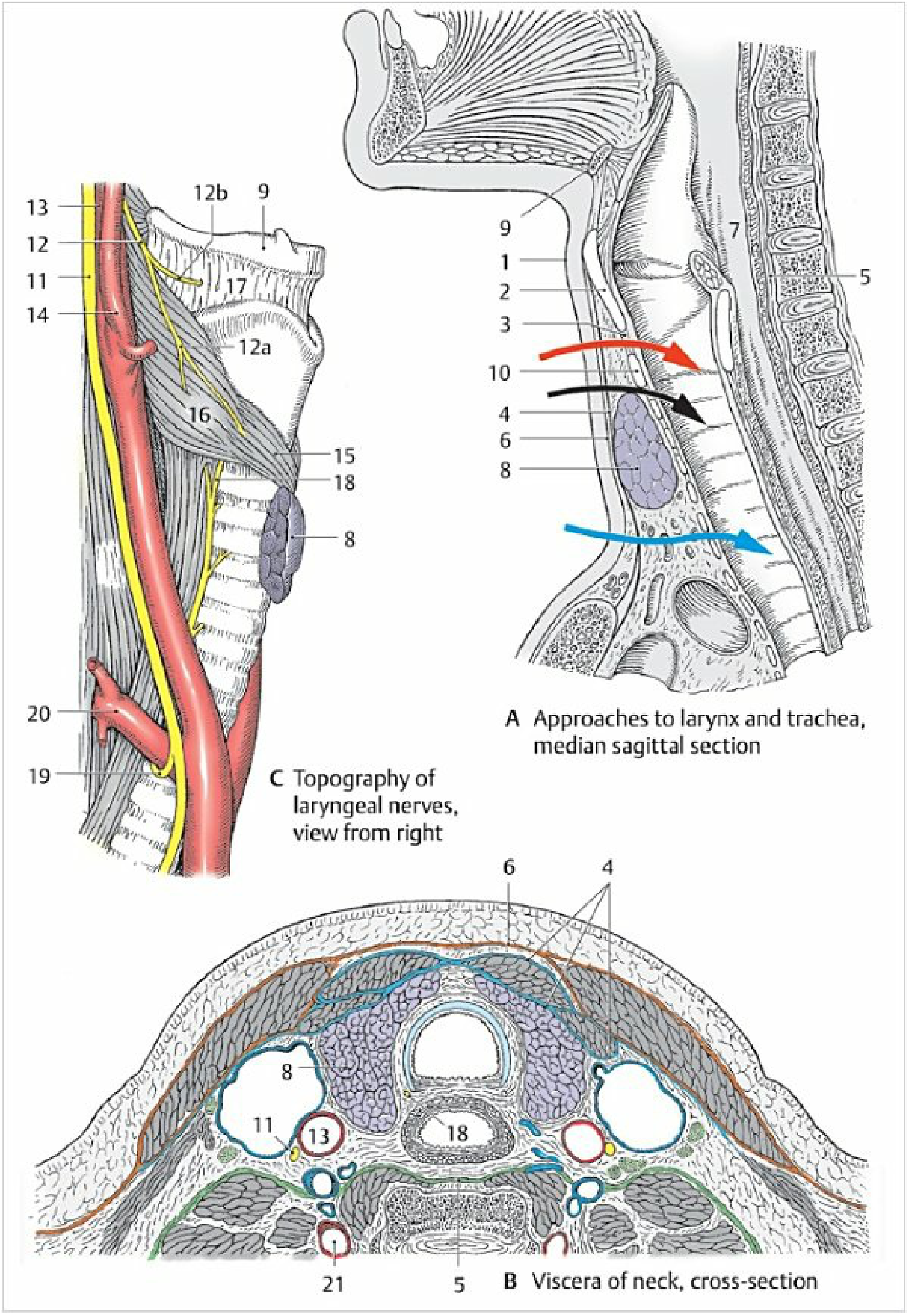
Topography of laryngeal nerves — Color Atlas of Human Anatomy
| Feature | Left RLN | Right RLN |
|---|---|---|
| Loops around | Arch of aorta (at ligamentum arteriosum) | Right subclavian artery |
| Course in neck | Paratracheal, tracheoesophageal groove, straight | More oblique, lateral to medial trajectory |
| Length | Longer (more susceptible to injury) | Shorter |
| Site of looping | Mediastinum (intrathoracic) | Root of neck (cervical) |
| Final entry | Larynx near cricothyroid joint | Larynx near cricothyroid joint |
Embryological Basis
- RLN is the nerve of the 6th pharyngeal arch
- Left: 6th arch artery → ductus arteriosus (ligamentum arteriosum) — nerve loops around it
- Right: 6th arch artery disappears → nerve loops around the 4th arch derivative (subclavian artery)
Non-recurrent RLN
- Occurs in ~0.5–1% on the right side; extremely rare (~0.04%) on left
- Associated with aberrant retroesophageal right subclavian artery (arteria lusoria)
- Surgically critical — can be injured during thyroidectomy if not anticipated
IV. INTRALARYNGEAL NEURAL CONNECTIONS (High-yield for Distinction)
| Structure | Description |
|---|---|
| Galen's nerve | Communicating branch between SLN and RLN (motor + sensory) |
| Human communicating nerve | Arises from external branch SLN → pierces cricothyroid membrane (motor + sensory) |
| Interarytenoid nerve | Bilateral RLN branches traverse interarytenoid muscle |
V. VOCAL CORD PALSY
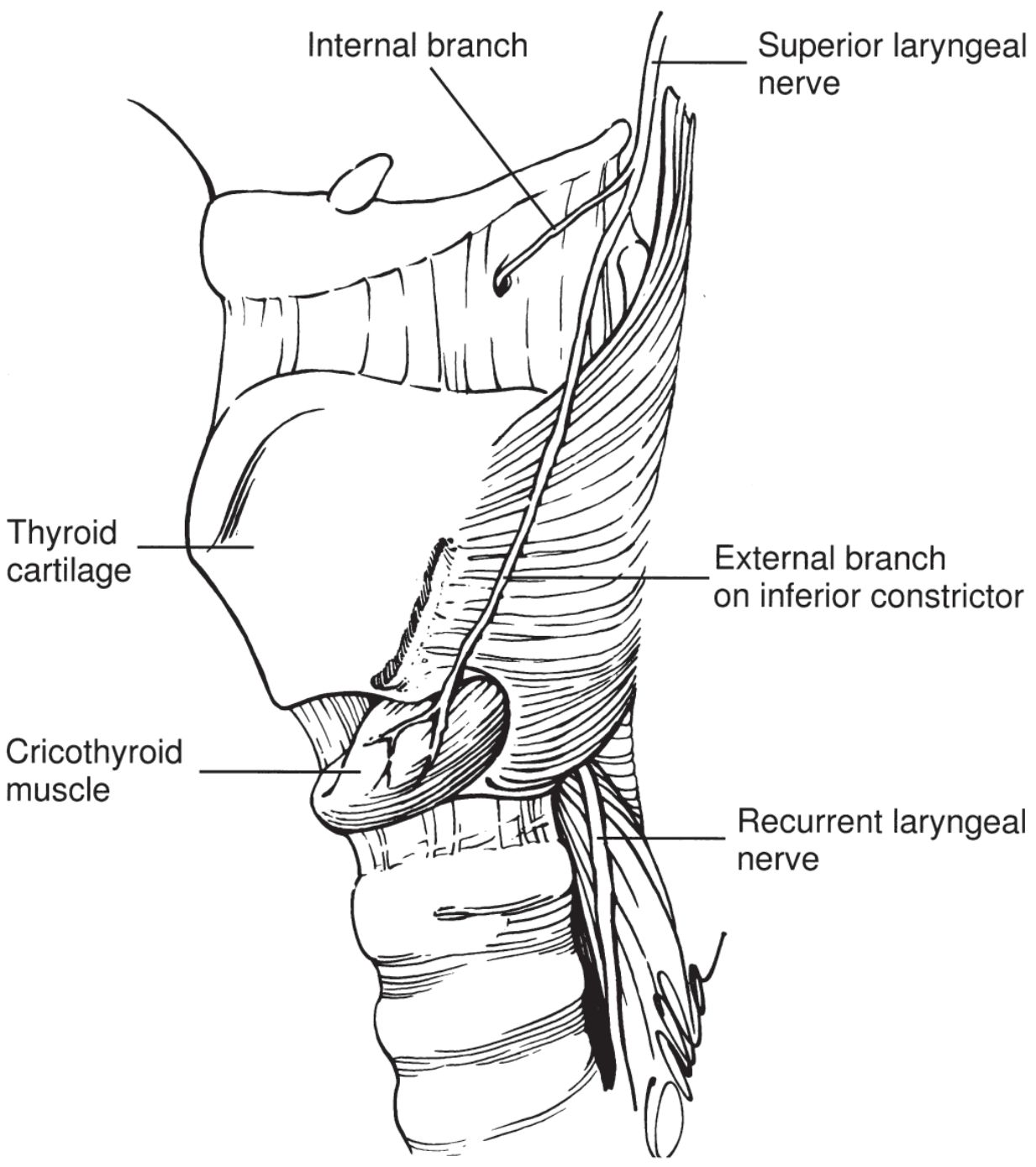
Laryngeal nerve supply — KJ Lee's Essential Otolaryngology
A. Semon's Law (Abductor Predominance of Injury)
In progressive/compressive lesions of the RLN:
- Abductors are paralysed first (PCA — most sensitive to pressure/ischaemia)
- Adductors are involved later
- This is because abductor fibres run more superficially in the nerve trunk
"The adductor muscles of the larynx tend to be affected first with peripheral recurrent laryngeal nerve injury (Semon's law)." — Localization in Clinical Neurology, 8e
B. Vocal Cord Position (Wagner-Grossman Theory)
| Nerve Injured | Position of Cord | Mechanism |
|---|---|---|
| RLN alone | Paramedian (cadaveric position) | Cricothyroid (SLN intact) keeps cord tense and slightly adducted |
| SLN alone | Near midline, slight lateral | Loss of cricothyroid tension |
| Both RLN + SLN | Cadaveric (intermediate) — fully abducted midway | Complete denervation, cord at rest |
| Complete vagus | Cadaveric (intermediate) | Same |
C. Unilateral vs Bilateral RLN Palsy
Unilateral RLN Palsy
- Hoarseness (flaccid dysphonia) — most common presentation
- Breathiness, short phrases, reduced loudness
- Diplophonia — two simultaneous pitch levels (unequal vibration frequency of two cords)
- Mild inspiratory stridor on contextual speech
- On laryngoscopy: paralysed cord lies near midline (paramedian); normal cord crosses to meet it on phonation
- Airway usually not compromised (intact interarytenoid adduction)
Bilateral RLN Palsy
- Acute: Inspiratory stridor + respiratory distress → may require tracheostomy
- Mechanism: Cricothyroids (SLN intact) pull cords together → severe midline approximation
- Chronic: Less severe airway compromise due to compensatory laryngeal muscle atrophy
- Voice: Weak but relatively clear (cords close enough to vibrate)
- Most common cause: Thyroidectomy
D. Effects of Laryngeal Nerve Injury — Summary Table
| Nerve | Side | Effect |
|---|---|---|
| SLN | Unilateral | Minimal — slight hoarseness, loss of high pitch |
| SLN | Bilateral | Hoarseness, easy voice fatigue |
| RLN | Unilateral | Hoarseness |
| RLN | Bilateral (acute) | Stridor, respiratory distress |
| RLN | Bilateral (chronic) | Aphonia |
| Vagus (CN X) | Unilateral | Hoarseness |
| Vagus (CN X) | Bilateral | Aphonia, no airway compromise (flaccid midposition) |
Morgan & Mikhail's Clinical Anesthesiology, 7e
E. Causes of Vocal Cord Palsy (by Level of Lesion)
| Level | Left RLN | Right RLN |
|---|---|---|
| Brainstem/skull base | CVA, tumour, MS, syringobulbia | Same |
| Neck | Thyroidectomy, neck dissection, trauma | Thyroidectomy, cervical spine surgery |
| Thorax (left > right) | Lung cancer (aortopulmonary window), aortic aneurysm, mediastinal LN, mitral stenosis | Apical right lung cancer, subclavian aneurysm |
| Idiopathic | 25–33% have no identifiable cause | Same |
Left cord palsy with no obvious neck cause → chest X-ray is mandatory (aortopulmonary window pathology) Right cord palsy → apical lordotic view to exclude right apical lung cancer — Gray's Anatomy for Students
F. Special Syndromes
- Rowland Payne Syndrome: RLN paralysis + phrenic + vagal nerve palsy + preganglionic Horner syndrome — caused by breast cancer extending behind carotid sheath at C6 level
- Ortner's Syndrome (Cardiovocal syndrome): Left RLN palsy from cardiovascular cause (aortic aneurysm, enlarged pulmonary artery in mitral stenosis/Eisenmenger)
G. Management of Vocal Cord Palsy
| Situation | Management |
|---|---|
| Unilateral (voice problem) | Voice therapy; vocal fold medialization (thyroplasty type I); injection laryngoplasty |
| Bilateral (acute airway) | Tracheostomy; lateralization procedures (arytenoidectomy, cordotomy) |
| RLN reinnervation | Ansa cervicalis–RLN anastomosis → improves cord tone/bulk (motion rarely returns; laryngeal synkinesis occurs) |
| Observation | If idiopathic/post-viral — spontaneous recovery in up to 2–12 weeks |
SUMMARY MNEMONIC
"SLN = Sensation Largely (+ 1 motor) / RLN = Rest of the motors"
- SLN internal = Sensation above cords (supraglottic)
- SLN external = 1 muscle only: Cricothyroid (Change pitch)
- RLN = All other intrinsic muscles + sensation below cords
- PCA = only Abductor — "PCA = Pull Cords Apart"
- Bilateral RLN injury (acute) → stridor (not aphonia) because SLN-innervated cricothyroids remain active and approximate cords
Sources: KJ Lee's Essential Otolaryngology; Cummings Otolaryngology Head & Neck Surgery; Localization in Clinical Neurology 8e; Morgan & Mikhail's Clinical Anesthesiology 7e; Gray's Anatomy for Students; Color Atlas of Human Anatomy Vol. 2
This is a shared conversation. Sign in to Orris to start your own chat.