incision and drainage procedure
Reading File
Finding Sources
Searching the Web
incision and drainage procedure technique abscess 2024
Reading File
Reading File
Searching Images
incision and drainage abscess technique
Reading File
Reading File
Reading File
Loading Image
Incision and Drainage (I&D)
Overview
Incision and drainage (I&D) is the definitive treatment for cutaneous and soft tissue abscesses. Antibiotics alone are insufficient — drainage is required. It is one of the most commonly performed procedures in emergency departments and outpatient clinics.
Indications
- Fluctuant abscess with a palpable pocket of purulence
- Abscess that has "pointed" (localized to a single area)
- Failed conservative management (e.g., warm compresses)
- Significant pain or expanding cellulitis around the abscess
- Hordeolum, Bartholin gland abscess, pilonidal abscess, perianal abscess
Contraindications / When to Refer
- Pulsatile mass at the site — suggests vascular etiology; do not incise
- Proximity to major vessels or nerves (e.g., femoral triangle, neck)
- Large, deep abscesses requiring OR drainage under general anesthesia
- Foreign body suspected at the site
- Hand infections near tendon sheaths — hand surgery referral
- Periorbital/orbital abscesses — ophthalmology referral
- Dental abscesses involving deep fascial spaces — ENT/oral surgery
Equipment
- No. 11 scalpel blade (preferred) or No. 15
- 1% or 2% lidocaine with epinephrine (1:100,000)
- 25–27 gauge needle for anesthesia
- Curved hemostat (Kelly clamp)
- Culture swab
- Irrigation syringe (20–35 mL) with saline or tap water
- Iodoform or plain gauze packing strip
- Sterile drape, gloves, mask, eye protection
Anesthesia
- Inject 1–2% lidocaine with epinephrine into the dome of the abscess, holding the needle parallel to the skin surface — blanching confirms spread
- For very large or deep abscesses, field block of the surrounding tissue improves anesthesia (anesthesia is harder to achieve in inflamed/acidic tissue)
- Consider procedural sedation for children or very painful abscesses
Step-by-Step Technique
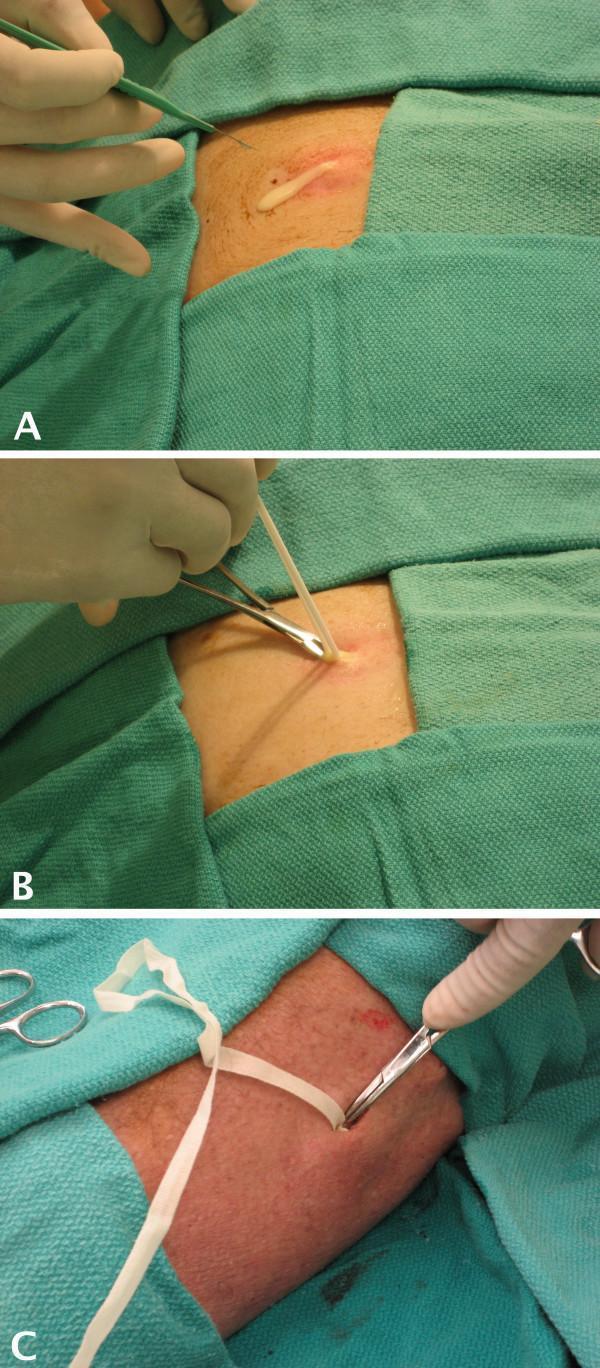
Sequential steps: (A) scalpel incision with pus drainage, (B) hemostat exploration and culture swab, (C) wound packing with gauze strip
| Step | Action |
|---|---|
| 1 | Identify and confirm the abscess. Bedside ultrasound is helpful — distinguishes cellulitis from a drainable collection and reduces treatment failure |
| 2 | Anesthetize the dome with lidocaine + epinephrine, parallel needle technique |
| 3 | Incise with No. 11 blade over the full length of the cavity — linear incision oriented along skin tension lines (Langer's lines) where possible |
| 4 | Culture purulent drainage (optional but recommended for MRSA-endemic areas, immunocompromised patients, or treatment failures) |
| 5 | Break loculations with a curved hemostat inserted into the cavity; sweep in multiple directions to ensure all pockets are opened |
| 6 | Irrigate the cavity copiously with normal saline or tap water via syringe |
| 7 | Pack the cavity loosely with iodoform gauze or plain gauze wick — keep the incision open; avoid overpacking |
| 8 | Dress with absorbent gauze; arrange follow-up in 1–3 days for recheck and packing removal |
Key Technical Points
- Linear incision is preferred. Avoid cruciate (X-shaped) incisions — the flap tips can necrose, leaving a poor scar.
- A "stab" incision alone is typically inadequate — the incision must span the full length of the cavity for adequate drainage.
- The scalpel is used only to incise the skin; do not use it deep within the cavity.
- In cosmetically sensitive areas (face) or under high skin tension, a stab incision or needle aspiration may be attempted first, with reassessment in 24–48 hours.
- Conform the incision to skin creases or natural folds whenever possible.
Packing: Current Evidence
Packing has been a traditional mainstay, but its routine use is controversial:
- Packing has not been proven to significantly improve outcomes over non-packing in most simple abscesses
- Some emergency physicians still pack larger cavities to prevent premature closure and allow continued drainage
- Follow-up in 1–3 days is essential regardless
Adjunct Antibiotics
- MRSA (particularly community-acquired MRSA) is now the predominant organism in cutaneous abscesses
- Antibiotics are generally not required for simple, uncomplicated abscesses after successful I&D in immunocompetent patients
- Antibiotics are indicated for:
- Surrounding cellulitis > 2 cm from the abscess margin
- Systemic signs (fever, lymphangitis)
- Immunocompromised state
- Failure to respond to I&D alone
- Preferred agents: TMP-SMX or doxycycline (covers CA-MRSA)
Special Locations
| Location | Notes |
|---|---|
| Peritonsillar abscess | Needle aspiration first; I&D with No. 11 blade no deeper than 8 mm to avoid carotid artery; suction immediately available |
| Bartholin gland abscess | Word catheter insertion preferred over simple I&D to reduce recurrence |
| Pilonidal abscess | Incise at dome, align with gluteal cleft; close follow-up required for definitive surgical management |
| Perianal abscess | Incise close to the anus to shorten any resulting fistula tract |
| Hordeolum | Eyelid abscess — refer if near lacrimal punctum; use chalazion clamp for stabilization |
Aftercare / Patient Instructions
- Remove/change packing at 24–48 hour follow-up
- Wound heals by secondary intention
- Warm soaks 2–3×/day after packing is removed
- Return immediately for worsening erythema, fever, or new fluctuance
- Recurrence of abscess in the same location should raise suspicion for: foreign body, underlying osteomyelitis, Crohn's disease (perianal), or hidradenitis suppurativa (axilla/groin)
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine (9780323354783); Pfenninger and Fowler's Procedures for Primary Care (9780323052672)
steps of intercostal drainage
Finding Sources
Searching the Web
intercostal chest tube drainage procedure steps technique 2024
Finding Sources
Searching Images
intercostal chest tube insertion safe triangle technique
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive textbook content. Let me compile the full answer.
Intercostal Drainage (Tube Thoracostomy / Chest Drain Insertion)
Indications
| Condition | Notes |
|---|---|
| Pneumothorax | Tension, large, symptomatic, or secondary |
| Hemothorax | Traumatic or spontaneous |
| Hemopneumothorax | Combined air + blood |
| Empyema | Infected pleural collection |
| Malignant pleural effusion | Symptomatic, recurrent |
| Chylothorax / Hydrothorax | Non-infectious fluid |
| Post-thoracic surgery | Prophylactic drainage |
Anatomy: The Triangle of Safety
The tube must be inserted within the Triangle of Safety to avoid injury to vital structures:
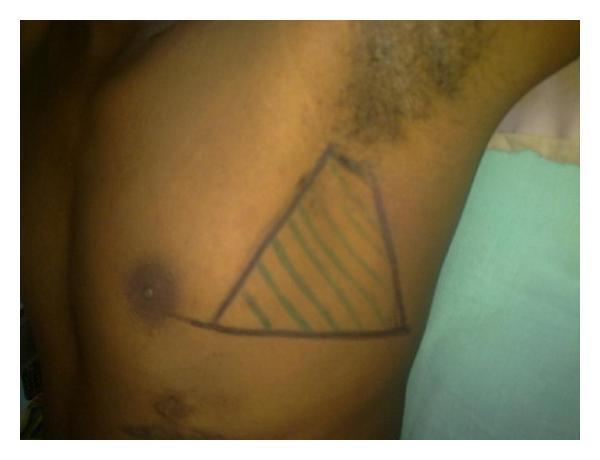
- Anterior border: Lateral edge of pectoralis major
- Posterior border: Anterior border of latissimus dorsi
- Inferior border: Horizontal line at the level of the nipple (5th intercostal space)
- Apex: Below the axilla
Preferred insertion site: 4th or 5th intercostal space, mid-axillary line
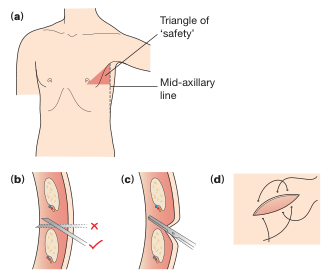
Critical rule: Always enter the pleural space over the superior border of the lower rib — the neurovascular bundle (intercostal artery, vein, nerve) runs in the groove on the undersurface of the upper rib.
Equipment
- Chest drain tube (28–32 Fr for fluid; 20–28 Fr for air; 14 Fr pigtail for simple pneumothorax)
- Scalpel with No. 15 blade
- Kelly clamp (curved hemostat)
- 1% lidocaine (plain) + 10 mL syringe + 21 and 25 gauge needles
- Chlorhexidine or povidone-iodine for skin prep
- Sterile drapes, gloves, gown, mask, eye protection
- Underwater seal drainage system (Bülau drain) or dry suction system
- Heavy non-absorbable suture (0 or 1-0 silk/prolene)
- Vaseline gauze-free sterile dressing
Patient Positioning
- Supine with ipsilateral arm raised above the head (abducted and externally rotated) to open up the intercostal spaces
- Head of bed elevated 30–45°
- Identify and mark the insertion site
Step-by-Step Procedure (Open / Blunt Dissection Technique)
Step 1 — Consent, Monitoring, and Analgesia
- Explain procedure and obtain informed consent
- Attach SpO₂ monitor and IV access; consider IV analgesia/sedation (opioid ± benzodiazepine)
- Pre-oxygenate if needed
Step 2 — Positioning and Skin Prep
- Position the patient as above, arm raised
- Clean the skin with chlorhexidine in wide circles; allow to dry
- Apply sterile drapes, exposing only the insertion site
Step 3 — Local Anaesthesia
- Raise a skin wheal with 1% lidocaine using a 25 G needle
- Switch to 21 G needle; infiltrate subcutaneous tissue, periosteum of the rib, and the intercostal muscles
- Walk the needle just over the top of the lower rib as you advance
- Aspirate as you advance — a rush of air or fluid confirms entry into the pleural space
- Inject lidocaine into the parietal pleura (most painful layer)
- Allow adequate time for analgesia to take effect (2–3 minutes)
Step 4 — Skin Incision
- Make a 2–3 cm transverse incision at the selected intercostal space (4th/5th ICS, mid-axillary line)
- Incision should be at least as wide as the tube diameter
- Optionally, make the skin incision one intercostal space below the intended pleural entry point to create a subcutaneous tunnel
Step 5 — Blunt Dissection and Pleural Entry
- Using a Kelly clamp, dissect bluntly through subcutaneous fat and intercostal muscles in a controlled, spreading motion
- Direct the clamp over the top of the rib to avoid the neurovascular bundle
- Apply firm, controlled pressure to pop through the parietal pleura — a rush of air or fluid confirms entry
- Spread the clamp to widen the opening before tube insertion
- Digital sweep: Insert a gloved finger into the pleural space to:
- Confirm pleural entry (not intra-parenchymal)
- Clear any clots or adhesions
- Palpate the lung to ensure it is not adherent
Step 6 — Tube Insertion
- Clamp the distal end of the tube with another Kelly clamp
- Using a clamp on the proximal end, guide the tube into the pleural space
- For pneumothorax: Direct tube apically (anterosuperiorly)
- For fluid (effusion/hemothorax): Direct tube basally and posteriorly
- Advance until all drainage holes are within the thorax
- Typical depth: 8–12 cm from the skin surface (mark at insertion)
- Confirm position: fogging of tube on respiration, drainage of fluid or air
Step 7 — Connect to Drainage System
- Connect tube to the underwater seal drain (Bülau bottle)
- Keep the bottle erect, ~100 cm below chest level
- Check for swinging of the fluid column with respiration (confirms patency)
- Check for bubbling (confirms air leak/pneumothorax drainage)
- Apply suction: −20 cm H₂O for standard drainage; −5 cm H₂O for fluid-only drainage
Step 8 — Secure the Tube
- Secure with a heavy non-absorbable suture (0-silk) anchored to the skin
- Place a mattress or purse-string suture around the wound for closure when the tube is removed
- Apply sterile occlusive dressing (no Vaseline gauze — increases infection risk)
Step 9 — Post-Procedure
- Chest X-ray immediately to confirm:
- Correct tube position (all drainage holes in pleural space — the radiopaque stripe should be unbroken)
- Resolution of pneumothorax or drainage of effusion
- Document drainage output (volume, color, character) at regular intervals
Tube Removal Criteria
| Condition | Removal Criteria |
|---|---|
| Pneumothorax | No air leak for 24 h AND lung fully expanded on CXR |
| Effusion / hemothorax | Output < 100–150 mL/24 h AND no residual collection on CXR |
| Post-surgery | As per surgical team protocol |
Removal technique: Ask patient to perform Valsalva (or remove at end-expiration); remove tube quickly while an assistant closes the wound with the pre-placed suture simultaneously; apply occlusive dressing.
Seldinger (Pigtail Catheter) Technique — Alternative
Used for small/simple pneumothorax or uncomplicated effusions:
- Anesthetize and confirm pleural entry with needle aspiration
- Thread a guidewire through the needle into the pleural space
- Remove needle; dilate track with serial dilators
- Thread pigtail catheter over guidewire
- Remove guidewire; connect to drainage system
Advantages: Less pain, smaller scar. Disadvantage: May kink; inadequate for large hemothorax or tension pneumothorax.
Complications
| Category | Examples |
|---|---|
| Insertional | Lung laceration, hemothorax from intercostal vessel injury, diaphragm/liver/spleen perforation |
| Positional | Subcutaneous placement, tube in fissure, drain kinked |
| Infective | Empyema, wound infection (15–20% overall complication rate) |
| Removal | Pneumothorax recurrence, air entrainment on removal |
Sources: Gray's Anatomy for Students (9780323934237); Sabiston Textbook of Surgery (9780443124341); Current Surgical Therapy 14e (9780323796835); Roberts and Hedges' Clinical Procedures in Emergency Medicine (9780323354783)
steps of modified radical neck dissection
Finding Sources
Searching the Web
modified radical neck dissection steps surgical technique
Reading File
Searching Images
modified radical neck dissection anatomy levels lymph nodes surgical
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.