11.Short note on pathogenesis of complications in diabetes mellitus.*** Give sufficient answer from Robbins textbook pathology to write in exam endocrine chapter
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a thorough exam answer. Let me compile a comprehensive, well-structured answer directly from Robbins.
Pathogenesis of Complications in Diabetes Mellitus
(Robbins Pathologic Basis of Disease & Robbins Basic Pathology)
Introduction
The morbidity associated with long-standing diabetes of either type (T1D or T2D) is due to damage of large- and medium-sized muscular arteries (diabetic macrovascular disease) and small vessels (diabetic microvascular disease) caused by chronic hyperglycemia. Complications most often first appear 15-20 years after onset of hyperglycemia. Their severity is related to both the degree and duration of hyperglycemia.
"The long-term effects of diabetes, rather than acute metabolic complications, are responsible for most of the morbidity and mortality of this disease."
- Robbins Pathologic Basis of Disease
Overview of Complications
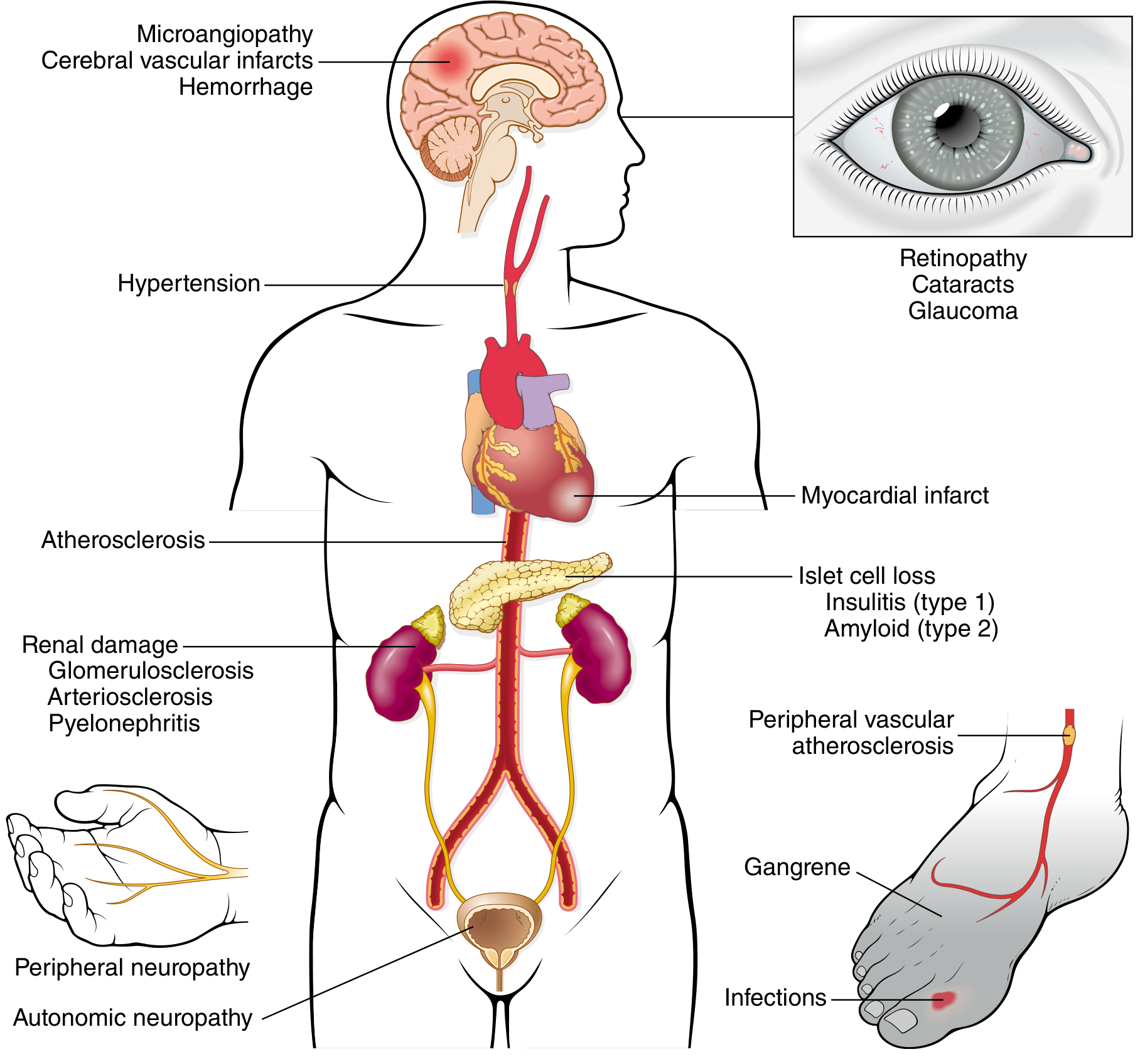
Complications are divided into:
- Macrovascular disease: Accelerated atherosclerosis → myocardial infarction, stroke, lower limb ischemia/gangrene
- Microvascular disease: Retinopathy, nephropathy, neuropathy
PATHOGENESIS - Four Core Mechanisms
Persistent hyperglycemia (glucotoxicity) causes end-organ damage through at least four distinct biochemical mechanisms. In each, increased metabolic flux due to hyperglycemia generates harmful intermediates.
1. Formation of Advanced Glycation End Products (AGEs)
- AGEs form via nonenzymatic reactions between glucose-derived metabolites (glyoxal, methylglyoxal, 3-deoxyglucosone) and the amino groups of intracellular/extracellular proteins
- Rate of AGE formation is accelerated by hyperglycemia
- AGEs bind to a specific receptor called RAGE (Receptor for AGE), expressed on inflammatory cells (macrophages, T cells), endothelium, and vascular smooth muscle
Detrimental effects of AGE-RAGE signaling:
- Release of TGF-β → excess basement membrane deposition
- Release of VEGF → neovascularization (diabetic retinopathy)
- Generation of reactive oxygen species (ROS) in endothelial cells
- Increased procoagulant activity on endothelial cells and macrophages
- Enhanced proliferation of vascular smooth muscle cells and extracellular matrix synthesis
Direct cross-linking effects:
- Cross-linked proteins trap other plasma proteins (e.g., LDL gets trapped in large-vessel walls → accelerates atherosclerosis; albumin gets trapped in capillary walls → basement membrane thickening of microangiopathy)
2. Activation of Protein Kinase C (PKC)
- Intracellular hyperglycemia stimulates de novo synthesis of diacylglycerol (DAG) from glycolytic intermediates
- DAG activates protein kinase C (PKC) - an important intracellular signal transduction pathway
Downstream effects of PKC activation:
- Production of VEGF (pro-angiogenic) - neovascularization in retinopathy
- Production of TGF-β (pro-fibrogenic) - increased extracellular matrix and basement membrane deposition (microangiopathy)
- Production of PAI-1 (plasminogen activator inhibitor-1) - procoagulant effect on vascular endothelium
Note: Effects of AGEs and activated PKC overlap - both contribute to diabetic microangiopathy.
3. Oxidative Stress and Disturbances in Polyol Pathways
- In tissues that do not require insulin for glucose transport (nerves, lens, kidneys, blood vessels), persistent hyperglycemia causes excess intracellular glucose
- This glucose is metabolized by aldose reductase to sorbitol (a polyol) and then to fructose
- This reaction consumes NADPH as a cofactor
- NADPH is also required by glutathione reductase to regenerate reduced glutathione (GSH) - a key antioxidant
- Progressive depletion of NADPH compromises GSH regeneration → increased oxidative stress
- Sorbitol accumulation in the lens contributes to cataract formation
4. Hexosamine Pathway Overload
- Hyperglycemia induces flux of glycolytic intermediates through the hexosamine pathway (generating fructose-6-phosphate)
- This results in cell damage, enhanced oxidative stress, and ultimately contributes to insulin resistance and vascular complications
MORPHOLOGY OF CHRONIC COMPLICATIONS
A. Diabetic Macrovascular Disease
- Accelerated atherosclerosis affecting aorta, large/medium arteries
- Results in: myocardial infarction (2-4x greater risk), stroke, lower extremity ischemia, gangrene
- Patients with diabetes have a 2-4x greater incidence of coronary artery disease and 4-fold higher risk of dying from cardiovascular complications
- Myocardial infarction is almost as common in females with diabetes as in males (unlike the general population)
- Contributing factors: hypertension (present in ~75% of T2D), dyslipidemia (high TG, high LDL, low HDL)
B. Diabetic Microangiopathy
- Diffuse thickening of basement membranes is the most consistent morphologic feature
- Seen in capillaries of: skin, skeletal muscle, retina, renal glomeruli, renal medulla
- Also in nonvascular structures: renal tubules, Bowman capsule, peripheral nerves
- Despite thickening, capillaries are leakier than normal to plasma proteins
- Underlies retinopathy, nephropathy, and neuropathy
C. Diabetic Nephropathy
Kidneys are prime targets - renal failure is second only to myocardial infarction as a cause of death in diabetes. Three lesions:
1. Glomerular lesions:
- Capillary basement membrane thickening - best appreciated by electron microscopy; begins ~2 years after onset of T1D; ~30% increase by 5 years
- Diffuse mesangial sclerosis - diffuse increase in mesangial matrix; PAS-positive deposits; progressive obliteration of glomeruli
- Nodular glomerulosclerosis (Kimmelstiel-Wilson lesion) - oval/spherical deposits of laminated matrix material in the periphery of the glomerulus; pathognomonic for diabetic nephropathy; associated with heavy proteinuria
2. Renal vascular lesions:
- Arteriolosclerosis - affects both afferent AND efferent arterioles (efferent arteriolar hyalinosis is virtually diagnostic of diabetes)
3. Pyelonephritis:
- More common and severe in diabetics
- Includes papillary necrosis (necrotizing papillitis) - much more prevalent in diabetics
Clinical progression: Microalbuminuria (>30 mg/day) → macroalbuminuria (>300 mg/day) → end-stage renal disease
D. Diabetic Ocular Complications
Retinopathy (most profound):
- Background/preproliferative retinopathy: microaneurysms, hard exudates, dot-blot hemorrhages, macular edema
- Proliferative retinopathy: neovascularization attributable to hypoxia-induced VEGF expression; can lead to vitreous hemorrhage and retinal detachment
- Leading cause of adult blindness in the United States
- 60-80% of patients develop some form of retinopathy
Other ocular complications:
- Cataracts - hyperglycemia → sorbitol accumulation in lens → acquired lens opacification
- Glaucoma - increased intraocular pressure → optic nerve damage
E. Diabetic Neuropathy
- Prevalence: up to 50% of diabetic patients overall; up to 80% of those with disease >15 years
- Can affect: central nervous system, peripheral sensorimotor nerves, autonomic nervous system
Types:
- Distal symmetric polyneuropathy (most common) - "glove-and-stocking" pattern; begins in lower extremities, later involves upper extremities; both motor and sensory function affected
- Autonomic neuropathy - bowel and bladder dysfunction, erectile dysfunction, orthostatic hypotension
- Mononeuropathy - sudden foot-drop, wrist-drop, isolated cranial nerve palsies
F. Infections
- Increased susceptibility to skin infections, tuberculosis, pneumonia, and pyelonephritis
- Cause ~5% of diabetes-related deaths
- In patients with diabetic neuropathy, a trivial toe infection may initiate a cascade: gangrene → bacteremia → pneumonia → death
Summary Table
| Mechanism | Key Mediator | Main Complication |
|---|---|---|
| AGE formation | RAGE signaling, TGF-β, VEGF | Microangiopathy, retinopathy, atherosclerosis |
| PKC activation | DAG, VEGF, TGF-β, PAI-1 | Retinopathy, microangiopathy |
| Polyol pathway | Sorbitol, NADPH depletion, oxidative stress | Cataracts, neuropathy |
| Hexosamine pathway | Fructose-6-phosphate, oxidative stress | Vascular complications, insulin resistance |
Key Concepts (Robbins)
- Long-term complications of diabetes involve four potential mechanisms from sustained hyperglycemia: AGE formation, PKC activation, polyol pathway disturbances, and hexosamine pathway overload
- Long-term complications include macroangiopathy (atherosclerosis, ischemic heart disease, lower extremity ischemia) and microangiopathy (retinopathy, nephropathy, neuropathy)
- HbA1c should be maintained below 7% to reduce risk of chronic complications
- Kimmelstiel-Wilson nodules = pathognomonic for diabetic nephropathy
- Efferent arteriolar hyalinosis = virtually diagnostic of diabetes
- Renal failure is #2 cause of death in diabetes (after MI)
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (pp. 1022-1027); Robbins & Kumar Basic Pathology (pp. 749-752)
This is a shared conversation. Sign in to Orris to start your own chat.