A 7 year boys has complain of breathless
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have strong clinical content. Let me compile the comprehensive answer.
Breathlessness in a 7-Year-Old Boy - Clinical Approach
Breathlessness (dyspnea) in a school-age child has a broad differential. The most common cause is bronchial asthma, but several other conditions must be excluded through careful history, examination, and targeted investigations.
Differential Diagnosis
The key differentials to consider (in order of likelihood at this age):
| Cause | Key Features |
|---|---|
| Bronchial Asthma | Expiratory wheeze, episodic, nocturnal/exertional, family/atopic history |
| Pneumonia | Fever, cough, rales/ronchi, focal chest signs, asymmetric exam |
| Bronchiolitis | Younger children usually; viral prodrome, wheeze |
| Croup (laryngotracheobronchitis) | Barky cough, inspiratory stridor, worse at night |
| Foreign body inhalation | Sudden onset, history of choking, focal/unilateral wheeze |
| Congenital cardiac disease / Myocarditis | Murmur, hepatomegaly, weight loss, sweating, pulmonary edema |
| Gastroesophageal reflux | Positional, feeding-related |
| Anemia / Metabolic | Pallor, no wheeze, systemic features |
| Pulmonary hypertension | Rare; right heart failure signs |
"The differential diagnosis for childhood asthma includes bronchiolitis, laryngotracheobronchitis (croup), pneumonia, cardiac disorders (e.g., myocarditis), and gastroesophageal reflux." - ROSEN's Emergency Medicine
History to Elicit
- Onset: Acute vs. chronic/recurrent?
- Triggers: Exercise, cold air, allergens, smoke, URIs?
- Time pattern: Nocturnal? Episodic? Continuous?
- Associated symptoms: Fever, cough (barky vs. productive), runny nose, rash, weight loss, sweating during feeds?
- Past history: Previous similar episodes? Eczema, allergic rhinitis?
- Family history: Asthma, atopy, allergies?
- Choking episode: Possibility of foreign body aspiration?
Examination
Vital Signs
Use the Pediatric Asthma Score to classify severity (from Harriet Lane Handbook):
| Component | Mild (1) | Moderate (2) | Severe (3) |
|---|---|---|---|
| Respiratory rate (6-10 yr) | ≤26 | 27-30 | ≥31 |
| O2 saturation | >95% room air | 90-95% room air | <90% or any O2 needed |
| Retractions | None/intercostal | Intercostal + substernal | + supraclavicular |
| Work of breathing | Speaks in full sentences | Partial sentences/short cry | Single words/grunting |
| Auscultation | Normal/end-expiratory wheeze | Expiratory wheeze | Inspiratory + expiratory wheeze/diminished sounds |
Key Examination Points
- Auscultation: Wheeze (expiratory = asthma), stridor (croup/upper airway), rales (pneumonia/pulmonary edema), diminished breath sounds (severe bronchospasm, effusion, foreign body)
- Cardiac exam: Murmur, hepatomegaly (cardiac cause)
- Skin: Eczema, urticaria (atopy)
- Symmetry: Unilateral reduced air entry suggests foreign body or effusion
- Pulse oximetry: Mandatory
Investigations
First Line:
- Pulse oximetry (immediate)
- Peak Expiratory Flow Rate (PEFR) if age >5 and cooperative (best of 3 attempts, standing)
- Chest X-ray: Not routine for all wheezing children. Indicated if: history of choking, focal chest signs, extreme distress, subcutaneous emphysema, or cardiac etiology suspected
If severe or uncertain:
- ABG: For severe bronchospasm with signs of respiratory failure. A PaCO2 ≥40 mmHg in a hypoxic child with retractions = impending respiratory failure
- CBC, CRP (if infection suspected)
- ECG/Echo (if cardiac cause considered)
Management - Likely Asthma (Most Common)
Mild Exacerbation
- Salbutamol (albuterol) SABA via MDI + spacer or nebulizer every 20 minutes for the first hour
- MDI + spacer is as effective as nebulization (per meta-analyses)
- Oral corticosteroids if: prior home SABA use, no prompt response to SABA
Moderate Exacerbation
- Repeated SABA (every 20 min x3)
- Systemic corticosteroids: Oral prednisolone 1-2 mg/kg/day (max 40-60 mg)
- Ipratropium bromide nebulized (anticholinergic, add-on)
- Oxygen to maintain SpO2 >95%
Severe/Impending Failure
- Continuous nebulized SABA
- IV/IM magnesium sulfate
- IV corticosteroids
- NIPPV (BiPAP) for cooperative patient to avoid intubation
- Intubation (last resort): Indications - severe airway obstruction, refractory hypoxemia, impending respiratory arrest
- Ventilator strategy: Slow rates, prolonged expiratory phase, minimal PEEP (to avoid air trapping)
- Escalation to PICU
Red Flags Requiring Urgent Escalation
- SpO2 <90% despite oxygen
- Unable to speak
- Silent chest (no wheeze = no airflow)
- Cyanosis
- Altered consciousness
- Normalizing PaCO2 in a distressed child (sign of fatigue and impending arrest)
Key Teaching Point
A "calm" child who suddenly appears to relax with decreased respiratory effort in acute asthma may be developing hypercarbia and altered mental status from respiratory fatigue - this is a medical emergency, not improvement.
Sources: ROSEN's Emergency Medicine, The Harriet Lane Handbook 23rd ed, The Harriet Lane Handbook Pediatric Asthma Score (Table 1.7)
Has 3-4 time in a month
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have the full classification table and the stepwise management chart for ages 5-11. Here is the complete, focused answer:
Asthma Classification & Management: 3-4 Episodes/Month in a 7-Year-Old
Step 1: Classify Severity (Ages 5-11, NAEPP)
With breathlessness 3-4 times per month, this boy falls into the Mild Persistent category:
| Component | Intermittent | Mild Persistent | Moderate Persistent | Severe |
|---|---|---|---|---|
| Symptoms | ≤2 days/week | >2 days/week but not daily | Daily | Throughout the day |
| Nighttime awakenings | ≤2×/month | 3-4×/month | >1×/week | Often 7×/week |
| SABA use | ≤2 days/week | >2 days/week but not daily | Daily | Several times/day |
| Activity interference | None | Minor limitation | Some limitation | Extremely limited |
| FEV1 | >80%, FEV1/FVC >85% | >80%, FEV1/FVC >80% | 60-80% | <60% |
3-4 episodes/month = >2 days/week but not daily → Mild Persistent Asthma, Step 2
Harriet Lane Handbook 23rd ed., Asthma Severity Classification Table (5-11 years)
Step 2: Investigations to Confirm
- Spirometry - FEV1, FVC, FEV1/FVC ratio; reversibility test (≥12% improvement after SABA = positive)
- Peak Flow (PEFR) - baseline and variability (>20% diurnal variation supports asthma)
- Chest X-ray - usually normal or shows hyperinflation; rules out alternative diagnoses
- Allergy testing - skin prick test or serum specific IgE (identify triggers: dust mites, animal dander, pollen, mold)
- CBC - eosinophilia supports atopic/allergic asthma
- FeNO (Fractional exhaled Nitric Oxide) - elevated (>25 ppb) supports eosinophilic airway inflammation
- Sweat chloride test - if cystic fibrosis is in the differential
Step 3: NAEPP Stepwise Management (Ages 5-11 years)
This boy = Step 2 (Mild Persistent)
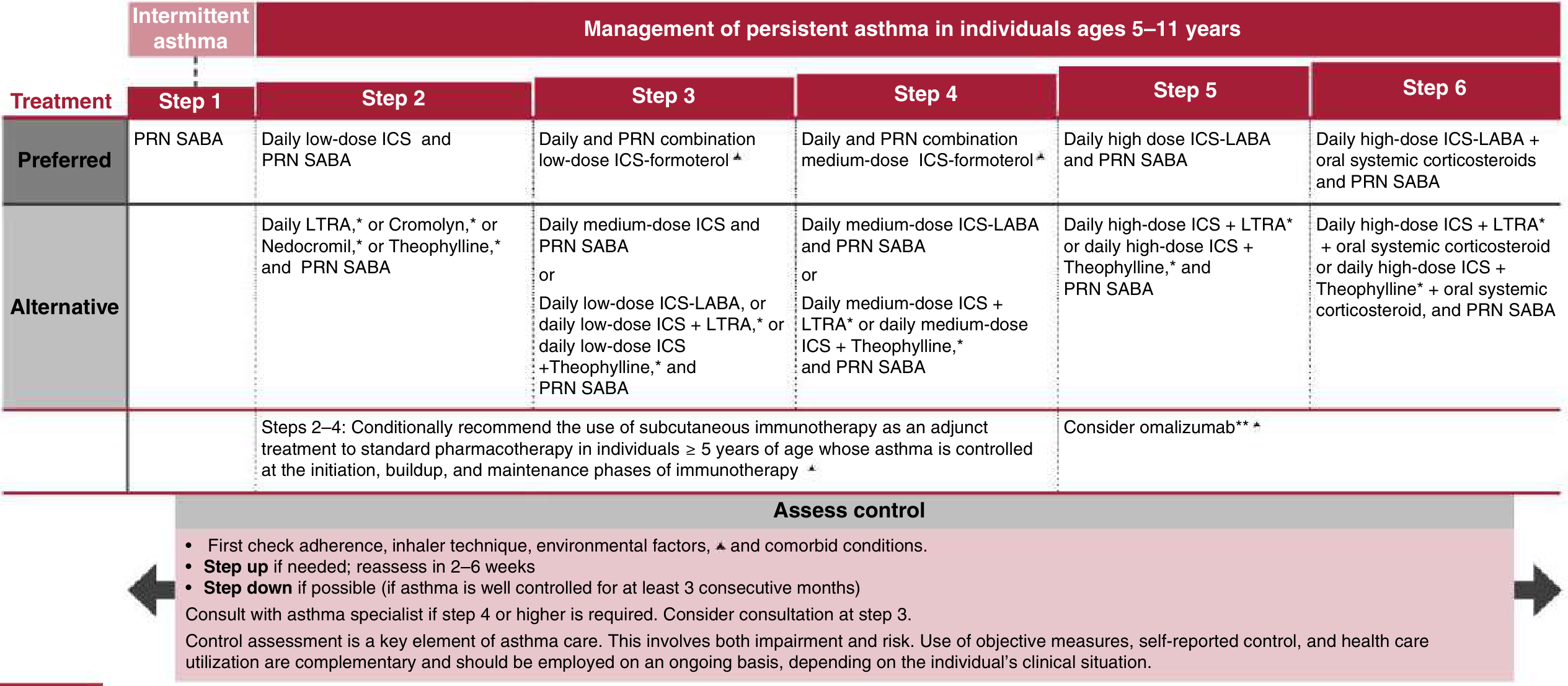
| Step | Preferred Treatment | Alternative |
|---|---|---|
| Step 1 (Intermittent) | PRN SABA only | - |
| Step 2 ← This patient | Daily low-dose ICS + PRN SABA | Daily LTRA or Cromolyn + PRN SABA |
| Step 3 | Daily low-dose ICS-formoterol (combined reliever/controller) | Medium-dose ICS + PRN SABA |
| Step 4 | Medium-dose ICS-formoterol | Medium-dose ICS-LABA + PRN SABA |
| Step 5 | High-dose ICS-LABA + PRN SABA | + Theophylline or LTRA |
| Step 6 | High-dose ICS-LABA + oral corticosteroids | - |
Specific Step 2 Prescription for This Child:
- Controller (daily): Inhaled corticosteroid (ICS) - e.g., Fluticasone 100 mcg/day or Budesonide 200 mcg/day via MDI + spacer
- Reliever (PRN): Salbutamol (albuterol) SABA via MDI + spacer as needed
- SABA use >2 days/week for symptoms = signal to step up
Step 4: Non-Pharmacological Management (Every Step)
- Trigger identification and avoidance: Dust mites, pets, mold, cockroach, smoke, cold air, exercise
- Impermeable mattress/pillow covers (if dust mite sensitized, as part of multicomponent strategy)
- Allergen immunotherapy: Conditionally recommended (Steps 2-4) in children ≥5 years with controlled asthma and confirmed allergen sensitization
- Asthma Action Plan: Written plan for parents - what to do in green/yellow/red zones
- Inhaler technique education: Critical - poor technique is the most common cause of poor control
- Immunizations: Up to date including influenza and COVID-19
Step 5: Follow-Up & Step-Down
- Reassess in 2-6 weeks after starting controller therapy
- Step down if well controlled for ≥3 consecutive months
- Step up if not controlled (reassess adherence, technique, and triggers first)
- Refer to specialist if Step 3 or higher is required
GINA Symptom Control Quick Check (ask at every visit):
In the past 4 weeks:
- Daytime symptoms >2 times/week? ✓
- Any night waking due to asthma?
- Reliever needed >2 times/week?
- Any activity limitation?
| Score | Control Level |
|---|---|
| 0 of 4 | Well controlled |
| 1-2 of 4 | Partly controlled |
| 3-4 of 4 | Uncontrolled |
Sources: Harriet Lane Handbook 23rd ed. (NAEPP EPR-3 + 2020 Focused Updates); Murray & Nadel's Respiratory Medicine (GINA)
This is a shared conversation. Sign in to Orris to start your own chat.