Epidemiology approach
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from Park's Textbook. Let me compile the full structured answer.
Epidemiological Study Designs
Source: Park's Textbook of Preventive and Social Medicine
Epidemiological study designs are broadly divided into three major categories: Descriptive, Analytical (Observational), and Experimental.
1. DESCRIPTIVE EPIDEMIOLOGY
Descriptive studies describe the distribution of disease in a population in terms of Person, Place, and Time. They do not test hypotheses - they generate them.
Uses:
- Provide data on the magnitude of disease (morbidity, mortality rates)
- Provide clues to disease aetiology and help formulate aetiological hypotheses
- Provide background data for planning and evaluating preventive/curative services
- Describe variations in disease occurrence by time, place, and person
Types:
- Case reports and case series
- Ecological (correlational) studies
- Cross-sectional surveys
2. ANALYTICAL EPIDEMIOLOGY
In contrast to descriptive studies that look at entire populations, analytical studies focus on the individual within the population. The object is not to formulate, but to test hypotheses. Although individuals are evaluated, the inference is to the population from which they are selected.
The two main analytical study designs are:
A. Case-Control Study (Retrospective)
A case-control study has three distinct features:
- Both exposure and outcome (disease) have already occurred before the start of the study
- The study proceeds backwards from effect to cause
- It uses a control or comparison group to support or refute an inference
Design (Fig. 8 from Park's):
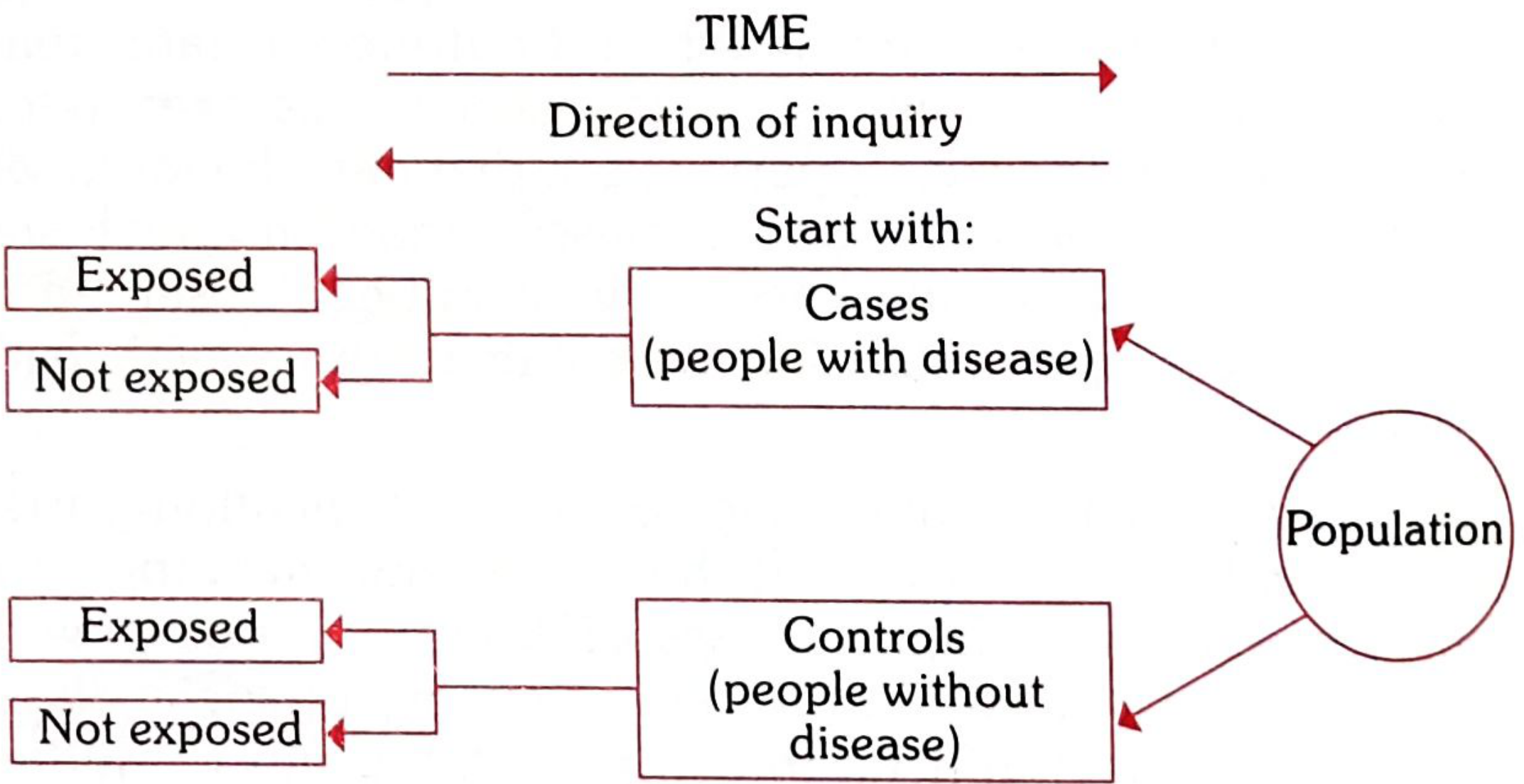
- Start with: Cases (people with disease) + Controls (people without disease), both drawn from the same population
- Ask: Were they exposed or not exposed in the past?
- Measure of association: Odds Ratio (OR) - an estimate of Relative Risk
When to use: Rare diseases, quick results needed, limited resources, generates or tests a specific hypothesis first.
B. Cohort Study (Prospective)
Design (Fig. 8 from Park's):
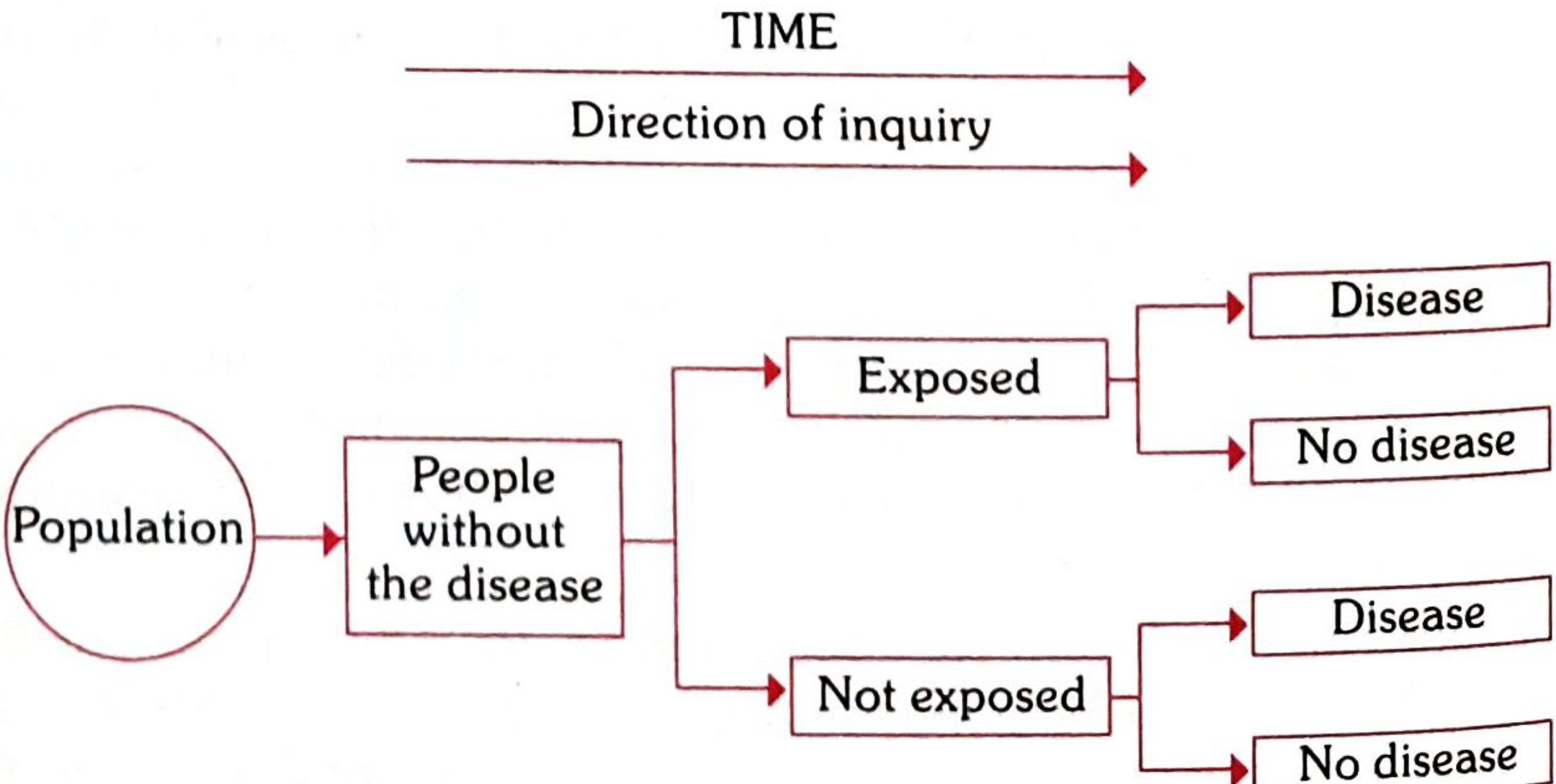
- Start with: People without the disease
- Divide into: Exposed vs Not Exposed
- Follow forward in time to see who develops disease
- Measure of association: Relative Risk (RR), Attributable Risk (AR), Incidence Rates
Comparison groups in cohort studies:
- Internal comparisons: Sub-groups within a single cohort classified by degree of exposure (e.g., cigarettes/day)
- External comparisons: An outside control group (e.g., smokers vs. non-smokers)
- General population rates: Experience of exposed group compared to general population rates
Classic example - Doll & Hill (1951): Sent questionnaires to 59,600 British doctors about smoking habits, formed two cohorts (smokers and non-smokers), followed for 4 years and 5 months. Results confirmed the association between smoking and lung cancer.
Classic example - Framingham Heart Study (1948): Followed residents of Framingham, Massachusetts, for 20 years to study relationships between risk factors (serum cholesterol, BP, weight, smoking) and cardiovascular disease.
Key Measures from Cohort Studies
| Measure | Formula | Meaning |
|---|---|---|
| Relative Risk (RR) | Incidence in exposed / Incidence in non-exposed | Strength of association; RR = 1 means no association |
| Attributable Risk (AR) | Incidence (exposed) - Incidence (non-exposed) | Portion of disease attributable to the exposure |
| Population-Attributable Risk | Incidence (total population) - Incidence (non-exposed) | Disease burden in the population due to the exposure |
Example (smoking & lung cancer, Doll & Hill):
- RR = 10 (smokers are 10x more likely to develop lung cancer)
- AR = (10 - 1) / 10 × 100 = 90% (90% of lung cancer in smokers is attributable to smoking)
Case-Control vs. Cohort: Key Differences
| Feature | Case-Control | Cohort |
|---|---|---|
| Direction | Effect → Cause (retrospective) | Cause → Effect (prospective) |
| Starting point | The disease | People exposed to risk factor |
| Test question | Does suspected cause occur more in cases vs. controls? | Does disease occur more in exposed vs. unexposed? |
| Use | First approach; exploratory; rare diseases | Testing a precisely formulated hypothesis |
| Sample size | Smaller | Larger |
| Time | Quick results | Long follow-up, delayed results |
| Measure | Odds Ratio (estimate of RR) | Incidence rates, RR, AR |
| Cost | Relatively inexpensive | Expensive |
3. EXPERIMENTAL EPIDEMIOLOGY
Experimental studies are similar in approach to cohort studies except the conditions are under the direct control of the investigator. The investigator deliberately applies or withdraws the suspected cause/intervention in an experimental group while making no change in a control group, then compares outcomes.
This sharply contrasts with observational studies (descriptive, case-control, cohort), where the epidemiologist only observes the natural course of events.
Aims:
- To provide scientific proof of aetiological/risk factors
- To measure effectiveness and efficiency of health services for prevention and treatment
Two types:
- Randomized Controlled Trials (RCTs) - strict random allocation
- Non-randomized/quasi-experimental trials - depart from strict randomization for practical reasons
Randomized Controlled Trial (RCT)
Design (Fig. 9 from Park's):
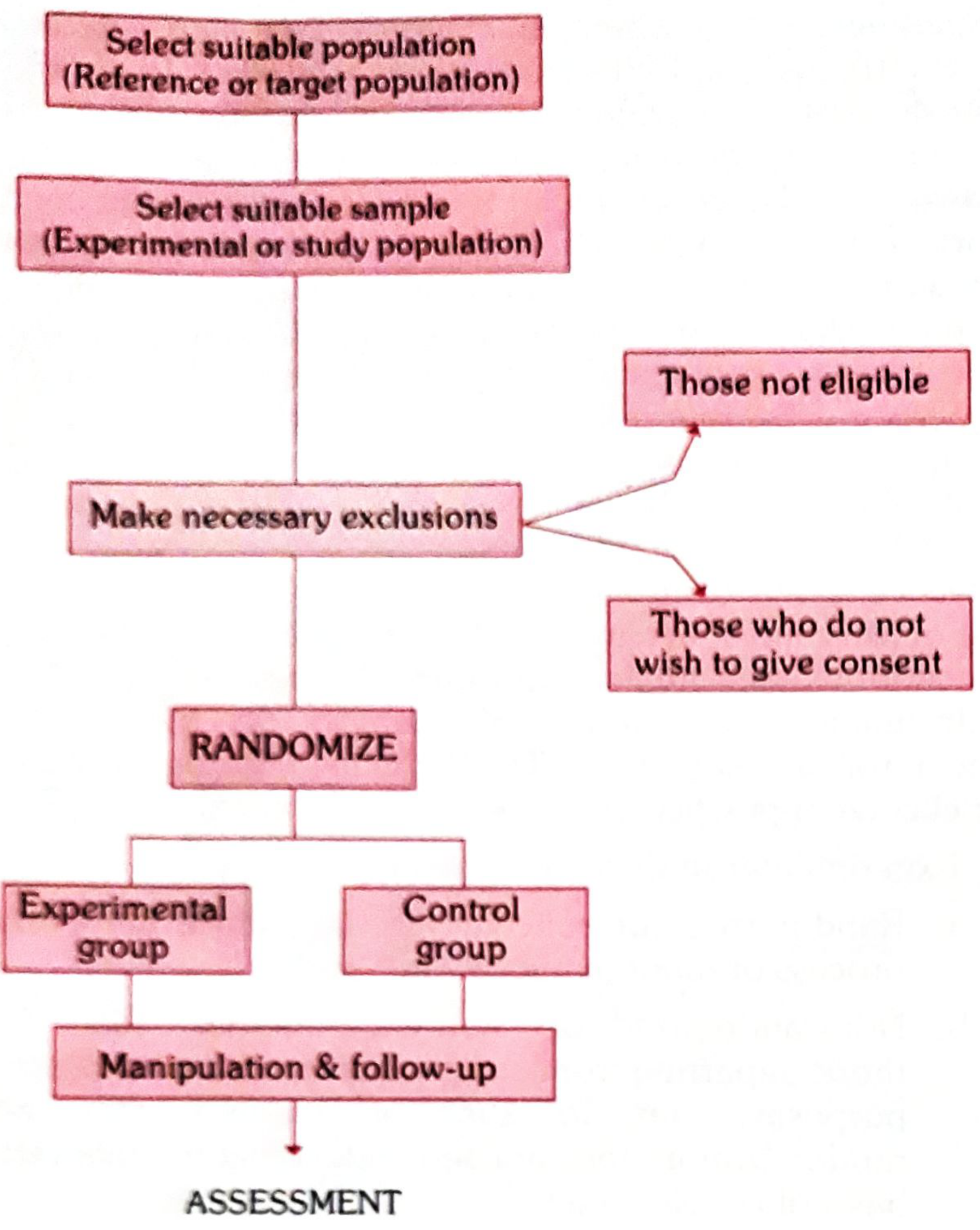
Basic steps in conducting an RCT:
- Drawing up a protocol (aims, objectives, selection criteria, sample size, allocation procedures, treatment schedule, evaluation plan)
- Selecting reference and experimental populations
- Randomization (ensures comparability of groups, eliminates selection bias)
- Manipulation or intervention (apply treatment/vaccine/preventive measure)
- Follow-up
- Assessment of outcome
Experimental studies carry all the advantages and disadvantages of cohort studies, plus three additional challenges: cost, ethics, and feasibility.
Sub-types of experimental studies (based on study design):
- Concurrent parallel: Two groups studied simultaneously - one receives intervention, other does not
- Cross-over: Each participant receives both the treatment and control at different times (serves as their own control)
Summary Hierarchy (Levels of Evidence)
Experimental
└── RCT (highest evidence for causation)
└── Non-randomized trials
Analytical (Observational)
└── Cohort Study (prospective)
└── Case-Control Study (retrospective)
└── Cross-Sectional Study
Descriptive
└── Ecological studies
└── Case reports / Case series
└── (lowest for establishing causation)
The progression in epidemiological investigation typically follows: Descriptive → Hypothesis generation → Case-Control (test hypothesis) → Cohort (confirm) → RCT (prove causation/efficacy).
- Park's Textbook of Preventive and Social Medicine, pp. 83-94
This is a shared conversation. Sign in to Orris to start your own chat.