Alpha blockers
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have rich content. Let me compile the comprehensive answer.
Alpha Blockers (Alpha-Adrenoceptor Antagonist Drugs)
Classification
Alpha blockers are classified by receptor selectivity and reversibility:
| Category | Drugs | Reversibility |
|---|---|---|
| Non-selective (α1 + α2) | Phentolamine, Phenoxybenzamine | Reversible / Irreversible |
| Selective α1 | Prazosin, Terazosin, Doxazosin | Reversible |
| Selective α1A (uro-selective) | Tamsulosin, Alfuzosin, Silodosin | Reversible |
Mechanism of Action
Alpha blockers occupy alpha-adrenoceptors and prevent their activation by catecholamines (norepinephrine, epinephrine).
- Reversible blockers (phentolamine, prazosin): dissociate from receptors; their block can be overcome by high agonist concentrations. Duration depends mainly on the drug's plasma half-life.
- Irreversible blockers (phenoxybenzamine): covalently bind by forming a reactive ethyleniminium intermediate. The block cannot be surmounted regardless of agonist concentration. Restoration of receptor responsiveness requires synthesis of new receptors, which may take several days -- important when a patient needs urgent surgery.
Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 245-246
Cardiovascular Effects
Because arteriolar and venous tone are largely maintained by alpha receptors on vascular smooth muscle, alpha blockade causes:
- Decreased peripheral vascular resistance and blood pressure
- Venous dilation - splanchnic capacitance veins dilate, reducing venous return
- Orthostatic hypotension - blocking sympathetically-mediated vasoconstriction prevents the normal compensation for postural changes (gravitational pooling of blood)
- Reflex tachycardia - baroreflex activation; beta receptors are unopposed, compensatory heart rate increase
Epinephrine reversal: When both alpha and beta receptors exist in vasculature, alpha blockers unmask the beta2 vasodilator effect of epinephrine. A pressor dose of epinephrine can be converted to a depressor response -- this is "epinephrine reversal."
Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 246
Individual Drugs
Non-Selective Alpha Blockers
Phenoxybenzamine
- Irreversible, non-selective alpha blocker
- Covalently binds alpha receptors
- Use: Pre-operative management of pheochromocytoma (blocks catecholamine surges)
- Administer for 1-2 weeks before surgical removal; prevents hypertensive crises
- Effects persist days (until new receptors are synthesized)
- ADRs: Orthostatic hypotension, reflex tachycardia, nasal congestion, inhibition of ejaculation
Phentolamine
- Reversible, non-selective alpha blocker
- Uses: Pheochromocytoma (acute hypertensive crises), prevention/treatment of dermal necrosis from norepinephrine extravasation, hypertensive emergencies
- Short-acting; given IV for acute use
- ADRs: Tachycardia, arrhythmias, GI stimulation (due to unopposed parasympathetics + alpha2 blockade enhancing NE release)
Selective α1 Blockers
Prazosin, Terazosin, Doxazosin
- Competitive (reversible) selective α1 blockers
- Relax both arterial and venous smooth muscle
- Unlike non-selective blockers, cause minimal reflex tachycardia (α2 receptors on presynaptic terminals remain intact, limiting norepinephrine release)
- Minimal change in cardiac output, renal blood flow, or GFR
Key pharmacological difference: Unlike phenoxybenzamine/phentolamine, these agents do NOT block presynaptic α2 receptors, so the feedback inhibition of NE release is preserved.
| Drug | Half-life | Duration | Notes |
|---|---|---|---|
| Prazosin | ~3 hrs | Short | Prototype; 3x daily dosing |
| Terazosin | ~12 hrs | Intermediate | Once daily |
| Doxazosin | ~22 hrs | Long | Longest acting; fecal excretion |
Therapeutic Uses:
- Hypertension - not first-line (inferior cardiovascular outcomes vs other antihypertensives, e.g., ALLHAT trial findings)
- Benign Prostatic Hyperplasia (BPH) - relax smooth muscle of bladder neck and prostate
- May produce modest improvement in lipid profiles and glucose metabolism
First-dose effect: The initial dose can produce an exaggerated orthostatic hypotensive response leading to syncope. Minimized by:
- Starting at 1/3 to 1/4 of normal dose
- Giving first dose at bedtime
Lippincott Illustrated Reviews: Pharmacology, p. 257-259
Uro-Selective α1A Blockers (for BPH)
| Drug | Key Feature |
|---|---|
| Tamsulosin | High α1A selectivity; minimal BP effect |
| Alfuzosin | Moderate selectivity |
| Silodosin | Highest α1A selectivity; most uro-selective |
These agents are more selective for α1A receptors in the prostate and bladder (than α1B in blood vessels), so they improve urinary flow with less pronounced hypotension.
Mechanism in BPH: Blockade of α1A receptors decreases tone in smooth muscle of the bladder neck and prostate, improving urine outflow and reducing symptoms.
Lippincott Illustrated Reviews: Pharmacology, p. 257-258
Adverse Effects (Class-Wide)
| Effect | Mechanism |
|---|---|
| Orthostatic hypotension | Venous dilation, impaired sympathetic vasoconstriction on standing |
| Reflex tachycardia | Baroreflex response (more with non-selective blockers) |
| First-dose syncope | Exaggerated hypotension - especially with prazosin |
| Nasal congestion | Nasal mucosal vasodilation |
| Inhibition of ejaculation | Block of α1 receptors in vas deferens (phenoxybenzamine > others) |
| Floppy iris syndrome | Intraoperative - iris billows during eye surgery; particularly tamsulosin |
| Additive hypotension | With vasodilators, nitrates, PDE-5 inhibitors (e.g., sildenafil) |
| Dizziness, drowsiness, fatigue | CNS effects |
Lippincott Illustrated Reviews: Pharmacology, p. 259
Clinical Uses - Summary
| Indication | Drug of Choice | Notes |
|---|---|---|
| Pheochromocytoma (pre-op) | Phenoxybenzamine | Start weeks before surgery; irreversible block needed |
| Pheochromocytoma (acute crisis) | Phentolamine IV | Rapid-acting reversible |
| Hypertension | Doxazosin / Terazosin | Not first-line; used as add-on |
| BPH | Tamsulosin, Alfuzosin, Silodosin | First-line; uro-selective preferred |
| NE extravasation necrosis | Phentolamine (local) | Injected around the site |
| PTSD nightmares | Prazosin | Off-label, reduces nightmare frequency |
Key Exam Points
- Epinephrine reversal = classic alpha blocker pharmacology exam concept
- Phenoxybenzamine is the only irreversible alpha blocker
- First-dose syncope is specific to selective α1 blockers (prazosin > others); minimized by bedtime dosing at low starting dose
- Floppy iris syndrome is most associated with tamsulosin - patients must inform their ophthalmologist before cataract surgery
- Alpha blockers are NOT first-line for hypertension (inferior outcomes per ALLHAT trial)
- Doxazosin has the longest duration; fecal excretion (unlike others which are urinary)
- ALLHAT trial showed doxazosin inferior to chlorthalidone for cardiovascular outcomes in hypertension
Microscopic image of atherscolisid in pathology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the key images. Let me compile the comprehensive answer with the microscopic images and their detailed explanations.
Atherosclerosis - Microscopic Pathology
1. Atherosclerotic Plaque - Histology (Coronary Artery Cross-Section)
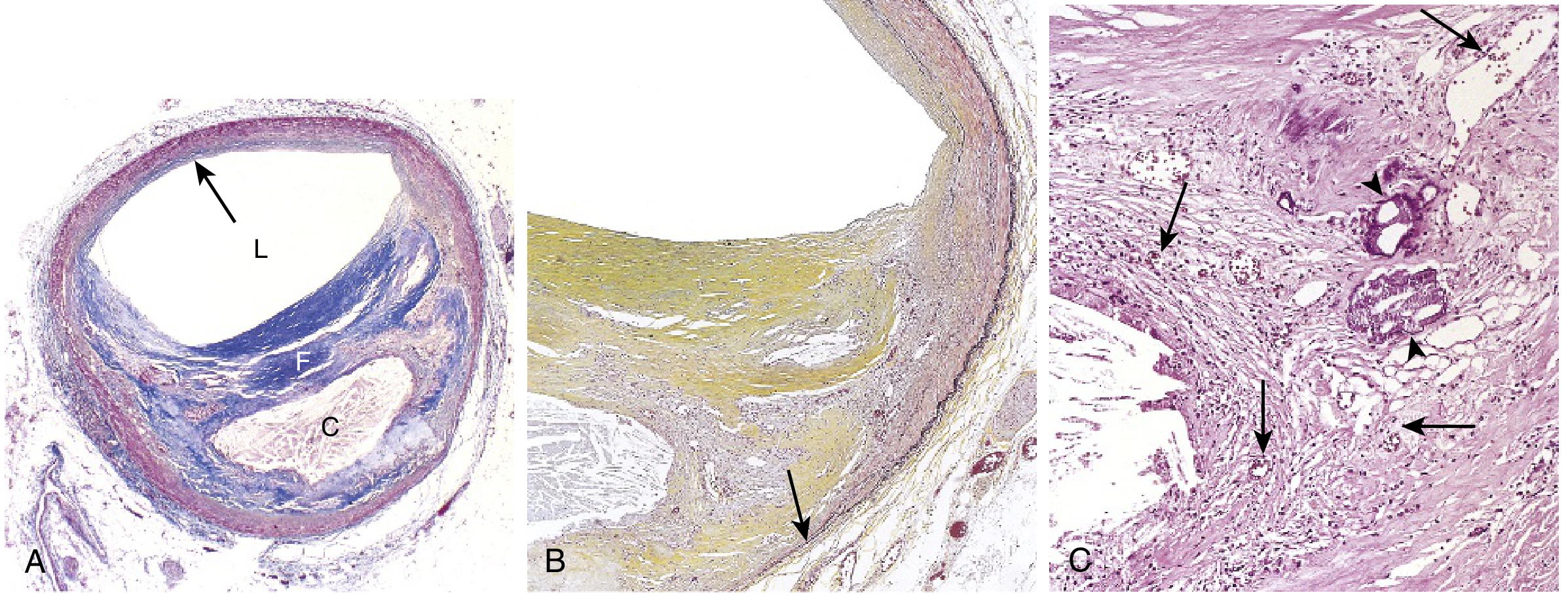
What you see in this image (A, B, C):
-
(A) Low power - Masson trichrome stain:
- L = Lumen (narrowed due to eccentric plaque)
- F = Fibrous cap (blue stain = dense collagen)
- C = Central necrotic/lipid core (pale, acellular)
- Arrow = area of vessel wall that is unaffected (eccentric lesion - key feature)
- The plaque occupies one side of the vessel; the opposite wall is relatively normal
-
(B) Medium power - elastin stain (black):
- Internal and external elastic membranes are attenuated and disrupted under the plaque
- Media of artery is thinned at the site of maximal plaque (arrow)
- Yellow staining = collagen-rich fibrous cap
-
(C) High power - junction of fibrous cap and necrotic core:
- Scattered inflammatory cells (lymphocytes, macrophages)
- Calcification = basophilic deposits (arrowheads)
- Neovascularization = small new blood vessels within the plaque (small arrows)
- Empty spaces = cholesterol clefts (cholesterol crystals washed out during processing)
Robbins & Kumar Basic Pathology, p. 319
2. Plaque Rupture and Thrombosis (Histology)
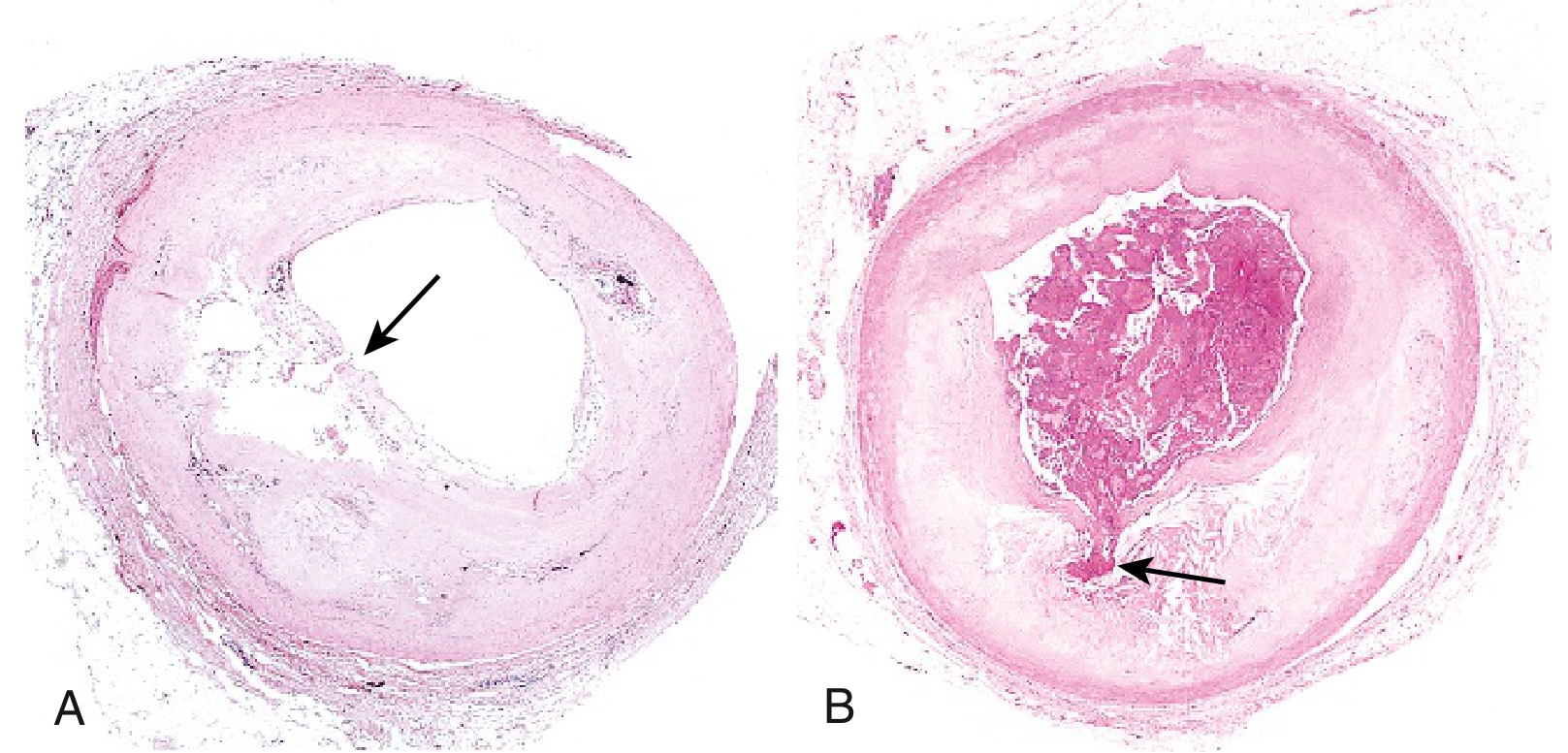
- (A) Plaque rupture without superimposed thrombus - arrow points to site of cap disruption
- (B) Acute coronary thrombosis superimposed on a ruptured plaque - the thrombus (dark pink mass) completely occludes the lumen; arrow shows site of fibrous cap rupture - this is the morphology of fatal myocardial infarction
Robbins & Kumar Basic Pathology, p. 322
3. Atheromatous Plaque - Structural Diagram
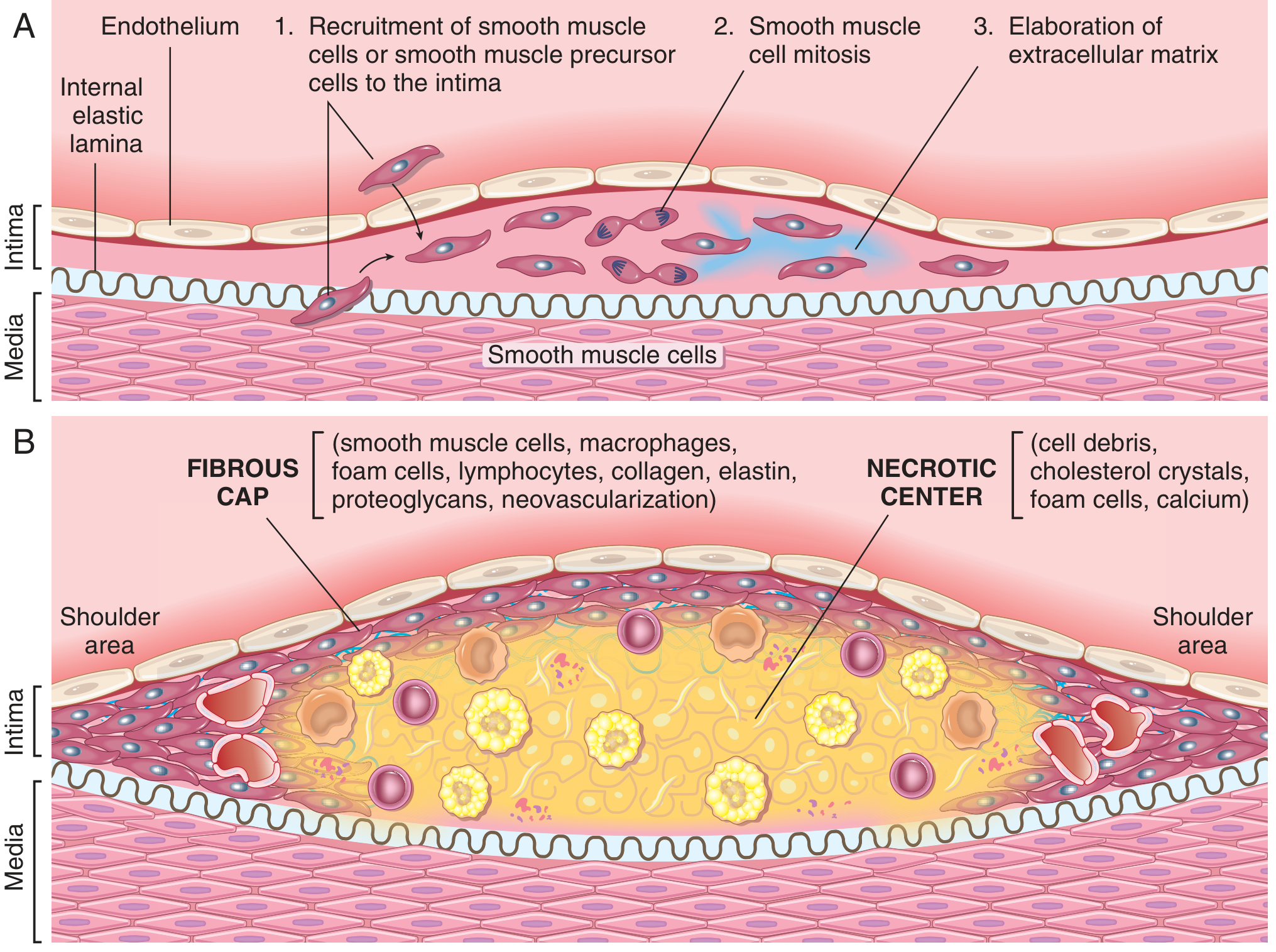
This labeled diagram shows the microscopic components of a mature atherosclerotic plaque:
Fibrous cap contains:
- Smooth muscle cells (SMCs)
- Macrophages and foam cells
- Lymphocytes
- Collagen, elastin, proteoglycans
- Neovascularization
Necrotic center contains:
- Cell debris
- Cholesterol crystals
- Foam cells (lipid-laden macrophages)
- Calcium deposits
Shoulder area (most vulnerable to rupture): Densest concentration of macrophages and T cells; thin cap here is where plaque rupture most commonly occurs.
Robbins & Kumar Basic Pathology, p. 314
4. Pathogenesis - Inflammasome Activation and Foam Cell Formation
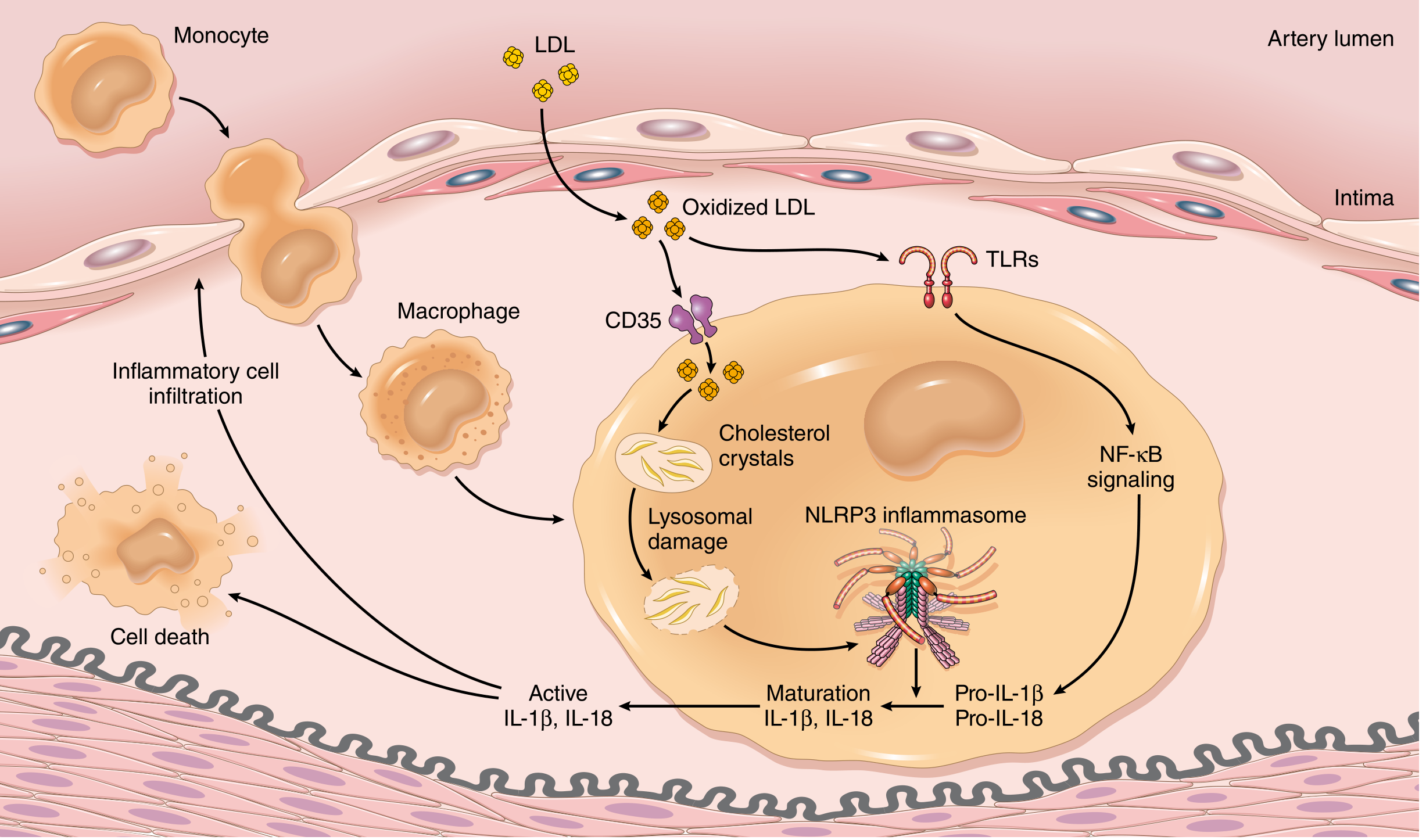
Key microscopic events shown:
- Monocytes adhere to damaged endothelium and differentiate into macrophages in the intima
- LDL enters the intima and is oxidized → taken up by macrophages via scavenger receptors
- Cholesterol crystals form within macrophages → activate the NLRP3 inflammasome
- This releases IL-1β and IL-18 → sustains chronic inflammation
- Lipid-laden macrophages = foam cells (the hallmark early lesion = fatty streak)
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 469
5. Natural History of Atherosclerosis - Summary Diagram
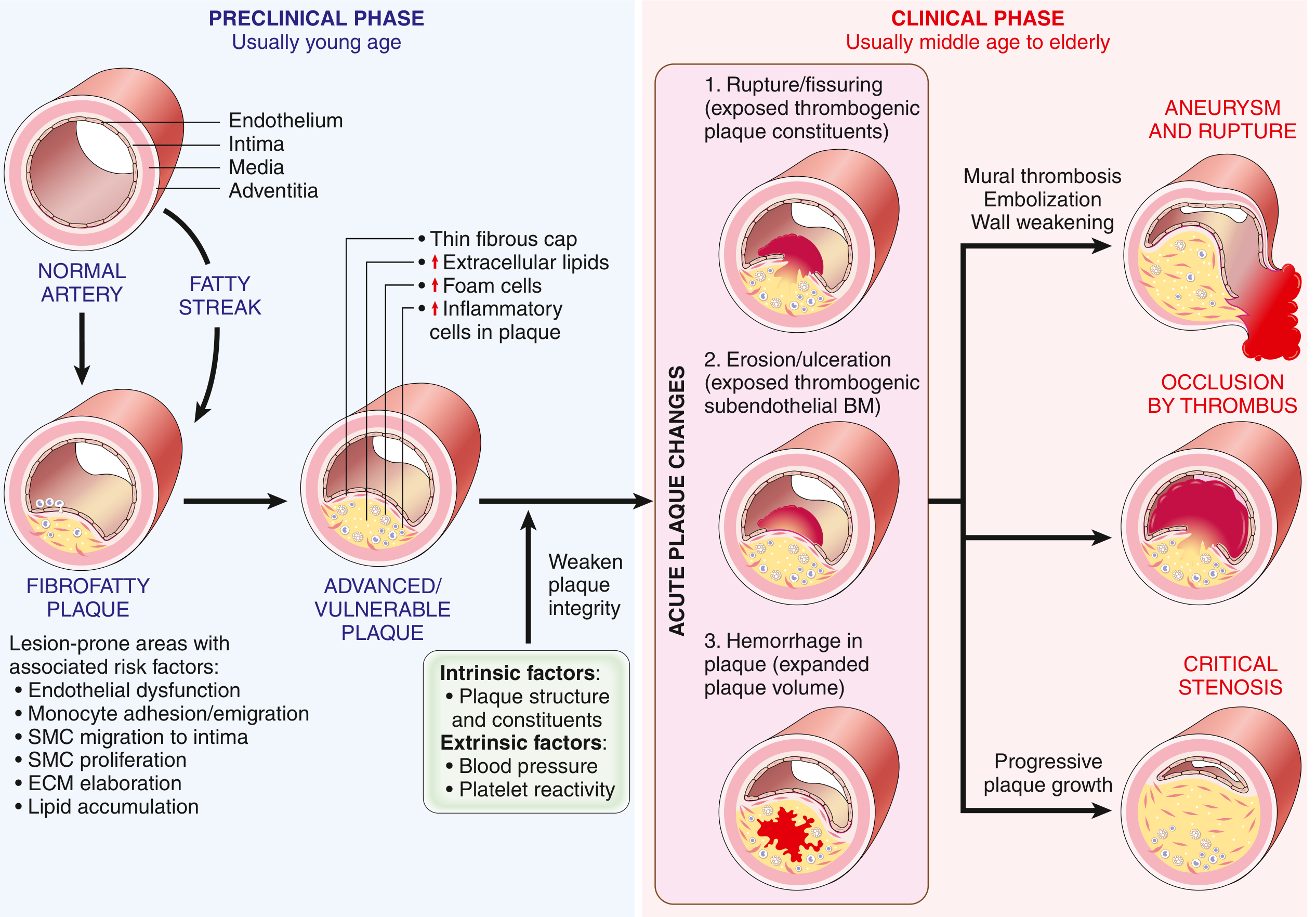
The progression from normal to clinical disease:
| Stage | Microscopic Features | Clinical Phase |
|---|---|---|
| Normal artery | Intact endothelium, normal intima | Asymptomatic |
| Fatty streak | Subendothelial foam cells, lipid deposits | Preclinical |
| Fibrofatty plaque | SMC migration to intima, ECM synthesis, lipid core | Preclinical |
| Advanced/vulnerable plaque | Thin cap, large lipid core, foam cells, inflammation | Subclinical or angina |
| Acute plaque changes | Rupture, erosion, or hemorrhage into plaque | Acute MI, stroke, sudden death |
Key Microscopic Features to Remember
| Feature | Significance |
|---|---|
| Foam cells | Lipid-filled macrophages; hallmark of fatty streak |
| Fibrous cap | Dense collagen + SMCs covering the necrotic core |
| Cholesterol clefts | Empty needle-shaped spaces (cholesterol dissolved in processing) |
| Calcification | Dystrophic calcium deposits in advanced plaques |
| Neovascularization | New capillaries within plaque - may bleed and cause intraplaque hemorrhage |
| Shoulder region | Most inflammatory, thinnest cap - highest rupture risk |
| Eccentric lesion | Plaque involves only part of the vessel circumference (cross-section appears asymmetric) |
Robbins & Kumar Basic Pathology, p. 319-322
This is a shared conversation. Sign in to Orris to start your own chat.