Describe the role of capnography in anaesthesia
Reading File
Finding Sources
Finding Sources
Searching PubMed
capnography anaesthesia monitoring
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have rich content from multiple authoritative anaesthesia textbooks. Here is a comprehensive answer:
Capnography in Anaesthesia
Capnography is the continuous measurement and graphical display of CO2 concentration in respiratory gases, typically expressed as end-tidal CO2 (EtCO2). It is considered one of the most important monitors in anaesthesia practice and is mandatory during all anaesthetic procedures.
1. Principle of Measurement
Capnographs exploit the Beer-Lambert law: CO2 absorbs infrared light in proportion to its concentration. Two main designs are in clinical use:
- Sidestream (diverting): Gas is continuously aspirated from the breathing circuit (up to 250 mL/min) into a sample cell within the monitor. Advantages include lightweight airway attachments and use in non-intubated patients, but the aspiration represents a small circuit "leak" and the tubing is prone to water precipitation causing obstruction and false readings.
- Mainstream (in-line): The sensor sits directly within the breathing circuit, giving faster response with no aspiration lag. It adds weight to the circuit connection and can only be used in intubated patients.
The normal PaCO2-EtCO2 gradient is 2-5 mmHg, reflecting alveolar dead space (ventilated but not perfused alveoli). Any increase in this gradient points to reduced pulmonary perfusion.
- Morgan and Mikhail's Clinical Anesthesiology, 7e, p.226-227
2. The Normal Capnogram Waveform
The capnogram trace has a characteristic shape with three expiratory phases:
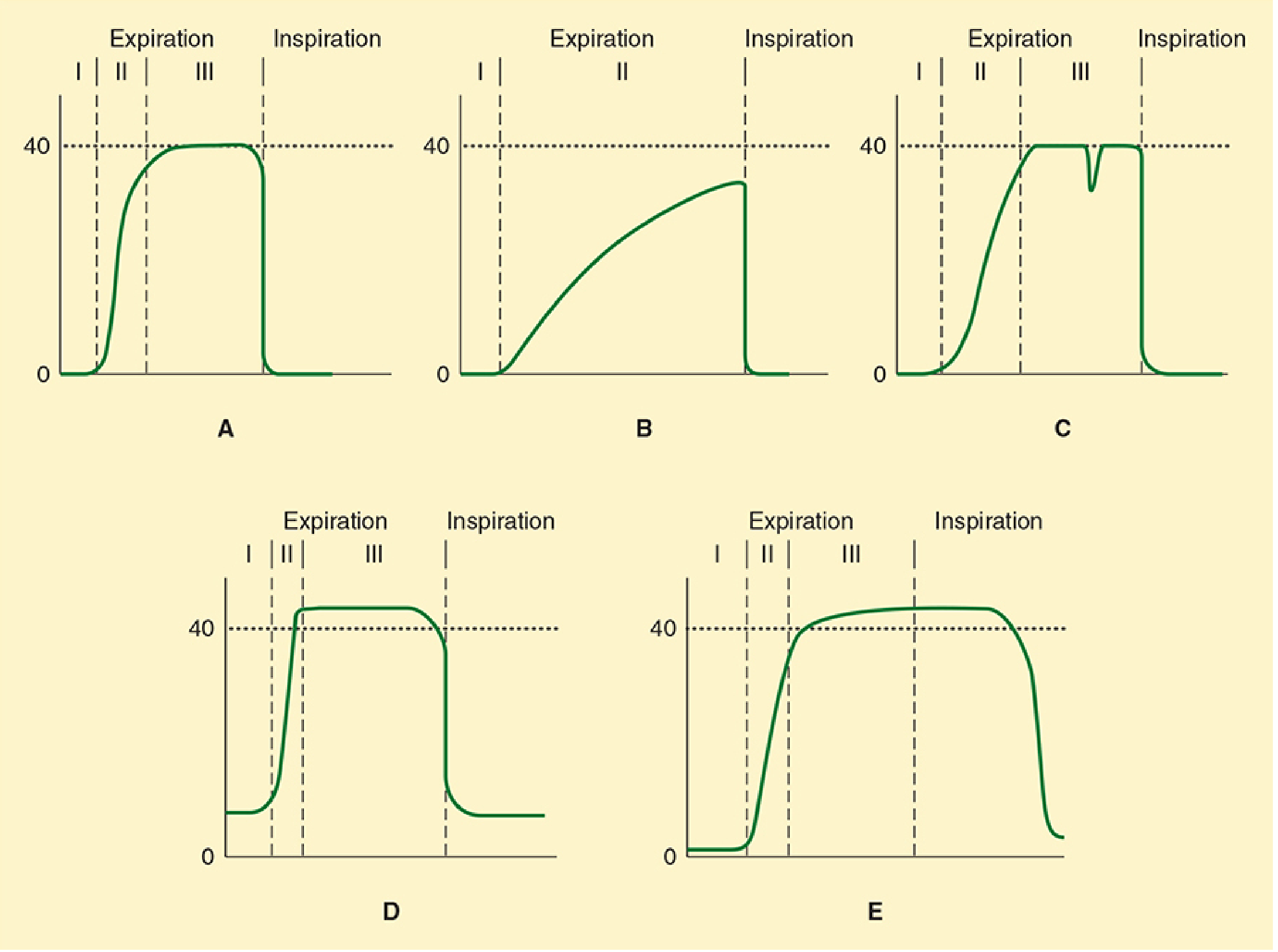
Figure (A-E from Morgan & Mikhail):
- Phase I - Anatomical dead space gas; CO2 near zero
- Phase II - Rapid rise as dead space mixes with alveolar gas
- Phase III - Alveolar plateau; the peak value is EtCO2 (normally ~35-40 mmHg)
- Inspiratory downstroke: sharp return to baseline as fresh gas is inhaled
Normal EtCO2 is approximately 35-45 mmHg (4.7-6 kPa).
3. Core Roles in Anaesthesia
3a. Confirmation of Endotracheal Tube Placement
The most safety-critical application. Expired CO2 confirms endotracheal placement; the absence of an alveolar waveform after intubation is strongly suggestive of oesophageal intubation. Any CO2 in the stomach from swallowed air is washed out within a few breaths, so persistent waveforms confirm tracheal placement. Importantly, capnography does not reliably detect mainstem bronchial (endobronchial) intubation, as both lungs are usually served.
- Scott-Brown's Otorhinolaryngology, p.389; Morgan & Mikhail, p.227
3b. Monitoring Adequacy of Ventilation
EtCO2 reflects alveolar ventilation in real time:
- Rising EtCO2 - hypoventilation, increased CO2 production, rebreathing
- Falling EtCO2 - hyperventilation, reduced CO2 production, or impaired pulmonary perfusion
This allows the anaesthetist to titrate ventilator settings (tidal volume, rate) to maintain normocarbia or target hypocapnia (e.g. in raised ICP).
3c. Detection of Circuit Faults
- Sudden loss of EtCO2 waveform - circuit disconnection, tube dislodgement, or cardiac arrest
- Elevated inspired CO2 (baseline elevated above zero) - rebreathing due to exhausted CO2 absorber or incompetent expiratory valve (waveform D in the figure above)
- Incompetent inspiratory valve - exhaled gas persists into the inspiratory phase (waveform E)
- Morgan & Mikhail, p.227-228
3d. Detecting and Monitoring Clinical Conditions
| Condition | Capnographic finding |
|---|---|
| Pulmonary embolism / air embolism | Sudden fall in EtCO2 (increased dead space + reduced cardiac output) |
| Malignant hyperthermia | Marked and rapid rise in EtCO2 (massively increased CO2 production) |
| Reduced cardiac output / haemorrhage | Gradual fall in EtCO2 |
| Obstructive airways disease (COPD/asthma) | Slow, sloping plateau - no flat alveolar phase reached (waveform B) |
| V/Q mismatch | Increased PaCO2-EtCO2 gradient |
| Spontaneous respiratory effort | Notch/dip in the plateau (waveform C) - useful for detecting awakening |
The "shark-fin" appearance (oblique, never flat plateau) is characteristic of bronchospasm or COPD.
3e. Monitoring During CPR and Resuscitation
EtCO2 is a sensitive marker of cardiac output during CPR - rising EtCO2 signals improved perfusion and heralds return of spontaneous circulation (ROSC). A persistently low EtCO2 despite effective compressions can inform decisions about ongoing resuscitation.
3f. Monitored Anaesthesia Care (MAC) and Sedation
Capnography is especially valuable in non-intubated sedated patients, where hypoventilation and apnoea can be missed clinically (particularly when supplemental oxygen maintains SpO2 temporarily). Meta-analysis data shows that respiratory depression is 17.6 times more likely to be detected with capnography than with standard monitoring alone. Pulse oximetry detects only ~50% of apnoea episodes that capnography catches, and hypoxaemia (SpO2 <90%) lags behind the onset of apnoea by an average of 45.6 seconds.
- Barash Clinical Anesthesia, 9e, p.2491-2492
Sidestream capnographs have been adapted for face masks, nasal airways, and modified nasal cannulae, making monitoring feasible in spontaneously breathing sedated patients.
4. Limitations
- EtCO2 underestimates PaCO2 in states of increased dead space (COPD, PE, low cardiac output) - the gradient widens significantly.
- High aspiration rates in sidestream devices can dilute readings in small tidal volumes (e.g. neonates/infants).
- Water vapour condensation can obstruct sidestream sampling lines.
- Cannot reliably confirm correct depth of ETT insertion (endobronchial intubation still gives a waveform).
- Readings may be affected by agents like nitrous oxide (infrared absorption overlap).
5. Regulatory and Standard-of-Care Status
EtCO2 monitoring during general anaesthesia is mandated by virtually all international anaesthesia standards (AAGBI, ASA, WHO) and is a standard ASA monitor wherever intubation or mechanical ventilation is used. Its role during sedation is increasingly recognised as essential given the evidence base above.
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e, pp. 226-228
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, pp. 2491-2492
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1, pp. 389-390
- Tintinalli's Emergency Medicine: A Comprehensive Study, pp. 122-123
This is a shared conversation. Sign in to Orris to start your own chat.