Fever
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete overview of Fever - its definition, pathophysiology, types, and causes, drawn from authoritative medical textbooks.
Fever - Definition, Pathophysiology, Types & Causes
1. Definition
Fever (pyrexia) is an abnormal elevation of body temperature above the usual range of normal (approximately 36-37.5°C / 97-99.5°F). It is produced when the hypothalamic set-point temperature is raised above normal. - Guyton and Hall Textbook of Medical Physiology
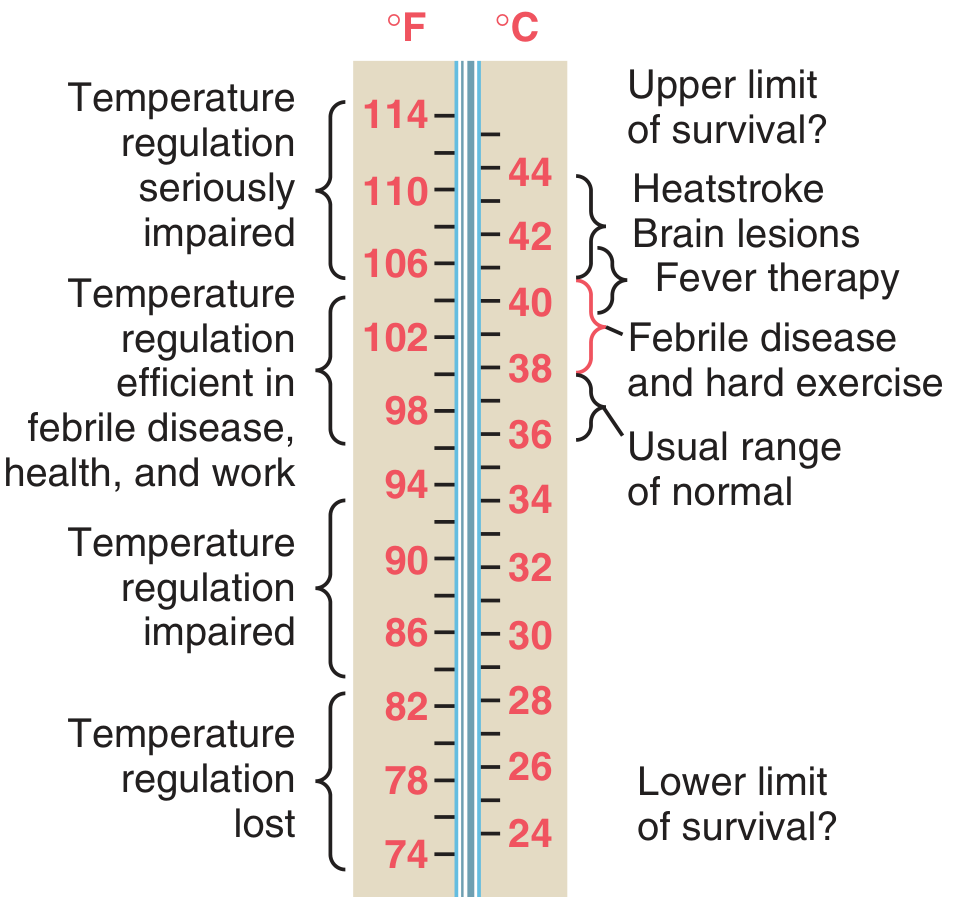
Figure: Body temperatures under different clinical conditions (Guyton & Hall)
2. Pathophysiology
Step 1 - Pyrogen Release
Bacteria, viruses, tissue breakdown products, and toxins (especially lipopolysaccharide / endotoxin from gram-negative bacteria) act as exogenous pyrogens.
Step 2 - Cytokine Production
These pyrogens are phagocytized by leukocytes, macrophages, and killer lymphocytes. These cells then release cytokines - key among them Interleukin-1 (IL-1), also called endogenous pyrogen or leukocyte pyrogen. Other important cytokines include IL-6 and TNF-alpha.
Step 3 - Hypothalamic Set-Point Reset
IL-1 reaches the anterior hypothalamus and stimulates local production of prostaglandins (PGE2). Prostaglandins raise the thermostat set-point. The hypothalamus now "reads" the normal body temperature as too low and activates heat-generating mechanisms:
- Shivering (rigors)
- Cutaneous vasoconstriction (chills, pale skin - the "cold" phase)
- Reduced sweating
Once the body reaches the new (higher) set-point, the patient feels hot, skin becomes warm, and sweating begins.
Step 4 - Resolution
When the cause resolves, the set-point drops back to normal. The body now sweats and vasodilates to shed excess heat (the "defervescence" phase).
Antipyretic Mechanism
Aspirin and NSAIDs inhibit cyclooxygenase (COX), blocking prostaglandin synthesis, thereby lowering the set-point back to normal. This causes vasodilation and sweating to dissipate heat. - Costanzo Physiology 7th Edition
3. Types of Fever (by Pattern)
Different fever patterns have classic diagnostic associations:
| Fever Type | Description | Classic Association |
|---|---|---|
| Continuous (Sustained) | Temperature remains elevated (>38°C) with <1°C daily variation; never touches normal | Typhoid, lobar pneumonia, UTI |
| Remittent | Temperature elevated all day, but daily variation >1°C; never touches normal | Most bacterial infections, TB |
| Intermittent | Temperature spikes above normal then returns to normal each day | Malaria, pyemia, septicemia |
| Quotidian | Daily fever spikes (every 24 hrs) | P. vivax malaria, some bacterial infections |
| Tertian | Fever spikes every 48 hours | P. vivax / P. ovale malaria |
| Quartan | Fever spikes every 72 hours | P. malariae |
| Hectic (Septic) | Wide daily swings (>5°C); temperature spikes then drops to subnormal with profuse sweating | Septicemia, pyemia, abscesses |
| Pel-Ebstein | Alternating weeks of fever and weeks of normal temperature | Hodgkin's lymphoma (classic) |
| Double Quotidian | Two fever spikes per day | Adult Still's disease, gonococcal endocarditis |
| Relapsing | Episodes of fever separated by days of normal temperature | Brucellosis, Borrelia infections, malaria |
4. Causes of Fever
Fever causes are broadly grouped into three major categories (the "3 I's" plus a 4th group):
A. Infections (most common)
- Bacterial: tuberculosis, pneumonia, endocarditis, intraabdominal abscess, osteomyelitis, UTI, septicemia
- Viral: CMV, EBV (infectious mononucleosis), influenza, HIV
- Parasitic: malaria (classic), amoebiasis
- Fungal: disseminated fungal disease (in immunocompromised)
- Others: brucellosis, psittacosis
B. Neoplasms
- Hematological: leukemia, lymphoma (especially Hodgkin's - Pel-Ebstein pattern), multiple myeloma
- Solid tumors: renal cell carcinoma (classic FUO presentation), hepatic metastases from any tumor, atrial myxoma
C. Connective Tissue / Autoimmune Diseases
- Adult Still's disease (double quotidian pattern, salmon-pink rash, high ferritin)
- Temporal arteritis / Giant cell arteritis (especially in elderly)
- SLE, rheumatoid arthritis
- Vasculitis syndromes
D. Other (Non-infectious) Causes
- Drug fever - many drugs, including antibiotics, anticonvulsants
- DVT / pulmonary embolism
- Transfusion reactions
- Post-surgical fever - atelectasis, wound infection, anastomotic leak, haematoma
- Tissue injury/necrosis - MI, trauma, burns
- Malignant hyperthermia - triggered by inhalation anesthetics in susceptible individuals
- Endocrine: thyroid storm, adrenal crisis
5. Fever of Unknown Origin (FUO)
Classic FUO is defined as:
- Fever >38.3°C on multiple occasions
- Duration >3 weeks
- No diagnosis despite 1 week of inpatient investigation
Key causes to consider from Textbook of Family Medicine:
| Category | Examples & Clues |
|---|---|
| Infections | Miliary TB, endocarditis, intraabdominal abscess, CMV, malaria, osteomyelitis, sinusitis |
| Tumors | Hodgkin's lymphoma (Pel-Ebstein), renal cell carcinoma, leukemia, liver metastases |
| Connective Tissue | Adult Still's (double quotidian, high ferritin), temporal arteritis (elderly), SLE |
| Hepatobiliary | Charcot's intermittent fever (ascending cholangitis from gram-negative sepsis) |
| Misc | Drug fever, factitious fever |
6. Summary of Key Points
- Fever is mediated through IL-1 → prostaglandins → hypothalamic set-point reset
- The pattern of fever is a useful diagnostic clue
- The most common cause is infection, but malignancy and autoimmune diseases are important differentials, especially in FUO
- Antipyretics (aspirin, NSAIDs) work by blocking COX → prostaglandin synthesis
- Temperatures >42°C (107.6°F) carry serious risk of brain lesions and heatstroke
Sources: Guyton & Hall Textbook of Medical Physiology | Costanzo Physiology 7th Edition | Textbook of Family Medicine 9e | Goldman-Cecil Medicine | Bailey & Love's Surgery 28th Edition
This is a shared conversation. Sign in to Orris to start your own chat.