Panopthalmitis case presentation viva questions and answers for ophthalmology residency in detail
Reading File
Finding Sources
Finding Sources
Searching the Web
panophthalmitis ophthalmology residency viva questions case presentation clinical features management
Reading File
Finding Sources
Reading Web Page
https://eyewiki.org/Panophthalmitis
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple textbook sources and EyeWiki to construct a thorough viva Q&A. Let me compile the final answer.
Panophthalmitis - Ophthalmology Residency Viva: Case Presentation Q&A
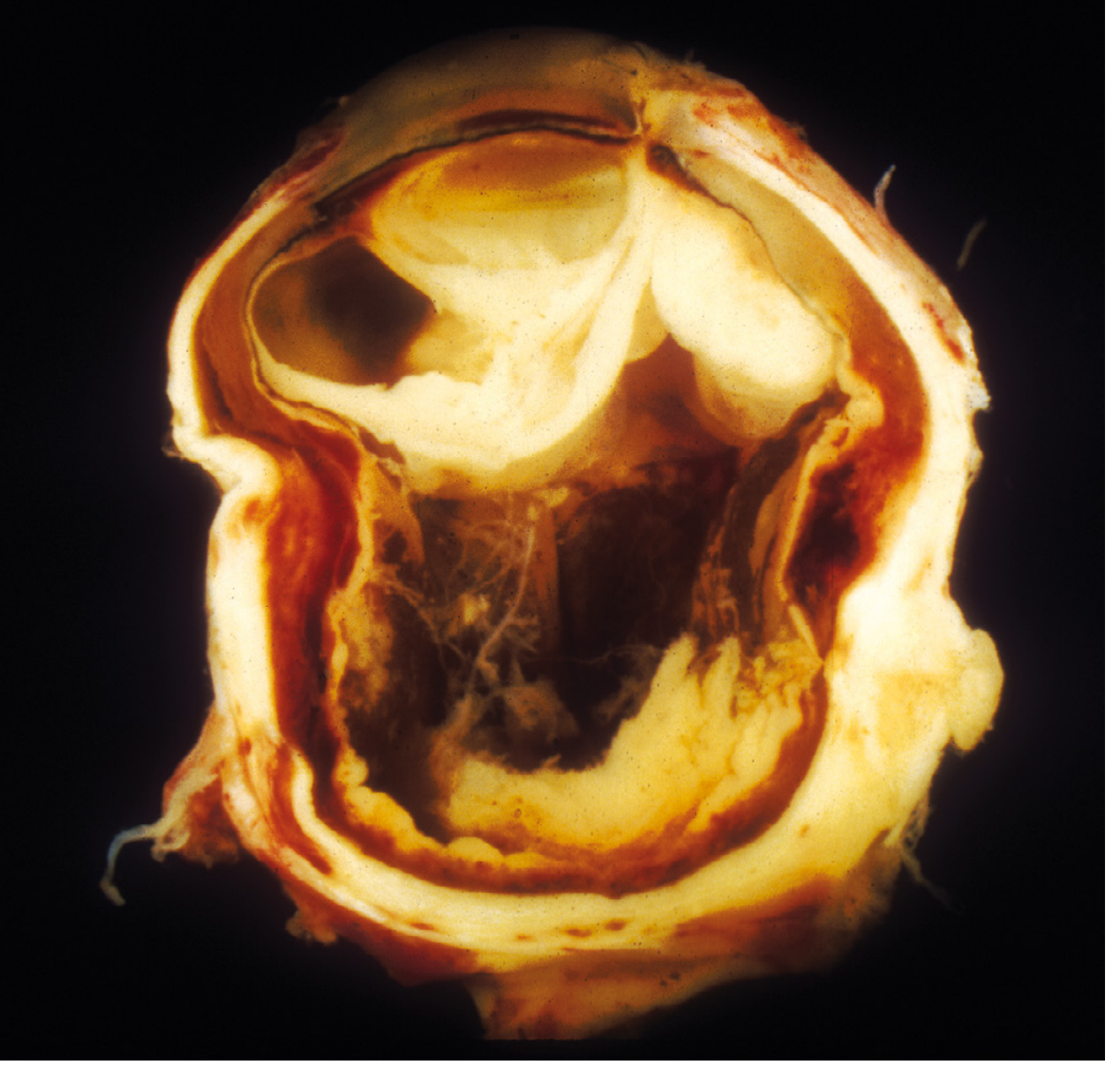
Gross pathology of exogenous panophthalmitis: cross-section of an enucleated eye after foreign body injury showing complete architectural disruption by suppurative inflammation - Robbins Pathologic Basis of Disease
SECTION 1: Definition and Classification
Q1. Define panophthalmitis and how does it differ from endophthalmitis?
A: Panophthalmitis is a severe, rapidly progressive suppurative inflammation involving ALL structures of the globe - vitreous, aqueous, retina, choroid, sclera, cornea, and lens - with extension into the surrounding orbital and periorbital tissues. The term derives from pan- (all), ophthalmo- (eye), -itis (inflammation).
Endophthalmitis involves the intraocular contents (vitreous and adjacent structures) but is CONTAINED within the fibrous tunic (sclera + cornea). Once inflammation breaches the sclera and involves the orbit, it becomes panophthalmitis. A simple clinical mnemonic: panophthalmitis = endophthalmitis + orbital cellulitis.
| Feature | Endophthalmitis | Panophthalmitis |
|---|---|---|
| Anatomy | Intraocular only | All globe layers + orbit |
| Scleral involvement | No | Yes |
| Proptosis | Absent | Present |
| Ophthalmoplegia | Absent | Partial/complete |
| Severity | Vision-threatening | Globe + life-threatening |
| Surgical outcome | Vitrectomy may save eye | Evisceration/enucleation often needed |
(Source: Robbins Pathologic Basis of Disease, p.1216; EyeWiki)
Q2. How is panophthalmitis classified by route of infection?
A:
-
Exogenous - organism enters from outside the body:
- Penetrating globe trauma (most common; especially organic matter, wood, soil-contaminated metal)
- Post-operative (cataract surgery, glaucoma filtering surgery - bleb-associated, intravitreal injections)
- Corneal ulcer with perforation
- Descemetocele rupture
-
Endogenous (metastatic) - hematogenous seeding from a distant focus:
- Infective endocarditis (vegetations on heart valves)
- IV drug use (Candida, gram-negatives)
- Liver abscess (Klebsiella pneumoniae - especially in diabetics from Southeast Asia)
- Meningococcemia, pneumococcemia
- Immunocompromised states (HIV, transplant, chemotherapy)
(Source: EyeWiki; Robbins, p.1216)
SECTION 2: Etiology and Microbiology
Q3. What are the common causative organisms?
A:
Bacteria (most common):
- Post-traumatic: Staphylococcus aureus, Streptococcus spp., Bacillus cereus (soil/organic matter injury - notoriously virulent, can destroy eye in 24-48 hours), gram-negatives, anaerobes
- Post-operative: Staphylococcus epidermidis (CoNS - most common), S. aureus, Streptococcus spp.
- Bleb-associated: Streptococcus spp., Haemophilus influenzae, gram-negatives (more virulent than post-cataract organisms)
- Endogenous: Klebsiella pneumoniae (diabetics, liver abscess), Streptococcus pneumoniae, gram-negative rods
Fungi:
- Candida albicans - IV drug users, immunocompromised
- Aspergillus spp.
- Rhizopus - mucormycosis (diabetic ketoacidosis)
Viruses (rare):
- Herpes simplex virus, Varicella zoster virus - herpetic panophthalmitis
- Dengue virus
Key viva point: Bacillus cereus panophthalmitis (often post-trauma with soil/plant material) carries the worst visual prognosis - it produces a metalloprotease that can destroy the eye in hours.
SECTION 3: Pathogenesis
Q4. Describe the pathogenesis of panophthalmitis.
A: The sequence is:
- Organisms gain access to the eye (exogenous: via wound; endogenous: blood-ocular barrier breakdown)
- Bacterial toxins + host inflammatory response destroy the blood-retinal barrier
- Suppurative inflammation begins in vitreous/aqueous (endophthalmitis stage)
- Infection extends through scleral emissaria (vessels/nerves) into episclera and orbit
- Orbital involvement causes proptosis, ophthalmoplegia, periorbital edema
- Without treatment: global architectural destruction, phthisis bulbi, or spread to cavernous sinus/meninges
Why is the retina so vulnerable? The retina poorly tolerates suppurative inflammation in the vitreous - even a few hours of purulent vitreous contact can cause irreversible retinal injury. (Robbins, p.1216)
SECTION 4: Clinical Features
Q5. Describe the typical case presentation of panophthalmitis.
A:
History:
- Recent penetrating trauma, ocular surgery, intravitreal injection, or systemic infection/sepsis
- Rapid progression over hours to days
- Diabetic, immunocompromised, or IV drug user history (for endogenous)
Symptoms (PANOPHT mnemonic):
- P - Pain (severe, throbbing, disproportionate to examination findings)
- A - Absent/reduced vision
- N - Nausea/vomiting (from severe pain)
- O - Orbital signs (proptosis, restricted movements)
- P - Photophobia
- H - Headache
- T - Temperature (fever, malaise, systemic features)
Signs - Anterior segment:
- Eyelid edema and erythema
- Chemosis (severe conjunctival edema)
- Conjunctival injection
- Purulent discharge
- Corneal edema, corneal opacity
- Hypopyon (pus in anterior chamber)
- Anterior uveitis
- Perforated cornea (in advanced cases)
Signs - Posterior segment:
- Absent red reflex
- Vitritis (hazy vitreous)
- Retinal infiltrates, flame-shaped hemorrhages with white centers
- Retinal/subretinal/choroidal abscesses
Signs - Orbital involvement (distinguishing panophthalmitis from endophthalmitis):
- Proptosis
- Ophthalmoplegia (partial or complete - indicates orbital spread)
- Afferent pupillary defect (APD)
- Raised or reduced IOP
Systemic:
- Fever, leukocytosis
- Signs of sepsis in endogenous cases
(Source: Wills Eye Manual; EyeWiki)
Q6. What features on examination distinguish panophthalmitis from preseptal/orbital cellulitis?
A:
| Feature | Preseptal Cellulitis | Orbital Cellulitis | Panophthalmitis |
|---|---|---|---|
| Proptosis | No | Yes | Yes |
| Ophthalmoplegia | No | Yes (with pain) | Yes (often complete) |
| APD | No | May be present | Present |
| Vision | Normal | May be reduced | Severely reduced/absent |
| Red reflex | Normal | Normal | Absent |
| Hypopyon | No | No | Characteristic |
| Vitreous involvement | No | No | Yes |
| IOP | Normal | Elevated | Variable |
| Chemosis | Mild | Moderate | Severe |
| Origin | Periocular skin | Paranasal sinus | Globe itself |
Remember: Panophthalmitis can cause orbital cellulitis as a complication, and orbital cellulitis from sinusitis can rarely cause panophthalmitis as a complication.
SECTION 5: Investigations
Q7. How do you investigate a case of panophthalmitis?
A:
Ocular/Local investigations:
- Vitreous tap + culture (most important) - vitreous biopsy has higher yield than aqueous tap
- Aqueous tap - additional sample
- B-scan ultrasonography - shows vitreous opacities (snowball opacities/echogenic vitreous), thickened posterior coats, choroidal effusions, retinal detachment, subretinal fluid; essential when fundus not visible
- OCT - retinal involvement, choroidal infiltrates (if media allows)
- Corneal scraping (if corneal ulcer present)
Imaging:
- CT orbit with thin cuts (1-3 mm) with and without contrast - extent of orbital involvement, subperiosteal abscess, foreign body localization, sinus disease, intracranial extension
- MRI orbit - superior soft tissue delineation, cavernous sinus assessment
Systemic (especially for endogenous):
- Blood cultures (minimum 2 sets) - before starting antibiotics
- CBC with differential (leukocytosis)
- Fasting blood glucose / HbA1c (diabetes)
- Transthoracic echocardiogram (TTE) - rule out infective endocarditis
- Liver function tests, liver ultrasound (if Klebsiella endogenous endophthalmitis suspected)
- HIV serology
- Urine culture, chest X-ray (identify primary source)
- Coagulation profile
Key viva point: Never delay intravitreal antibiotics for culture results. Tap + inject simultaneously.
SECTION 6: Management
Q8. Outline the emergency management of panophthalmitis.
A: Management is multidisciplinary (Ophthalmology + Infectious Disease + Internal Medicine). The key principles:
Step 1 - Immediate (within the hour):
- Hospital admission - panophthalmitis is a medical emergency
- IV access, blood cultures before antibiotics
- Urgent orbital imaging (CT)
- Vitreous + aqueous tap for smear and culture
Step 2 - Intravitreal antibiotics (cornerstone of treatment):
- Vancomycin 1-2 mg/0.1 mL (gram-positive coverage)
- Ceftazidime 2 mg/0.1 mL (gram-negative coverage)
- Repeat at 48-72 hours if not improving; consider pars plana vitrectomy
Step 3 - Systemic antibiotics:
- IV broad-spectrum: vancomycin + piperacillin-tazobactam OR carbapenem (meropenem) for severely ill
- Adjust based on culture sensitivities
- Duration typically 2-4 weeks for bacterial; longer for fungal
Step 4 - Adjunctive:
- Topical antibiotics (fortified: vancomycin 50 mg/mL, ceftazidime 50 mg/mL) hourly
- Cycloplegics (atropine 1%) - for pain and prevent posterior synechiae
- Topical steroids after 48 hours of antibiotics (controversial)
- Oral fluoroquinolones (excellent ocular penetration) for 10-14 days
For fungal:
- Intravitreal voriconazole (100 mcg/0.1 mL) OR amphotericin B (5-10 mcg/0.1 mL)
- IV voriconazole or amphotericin B systemically
Q9. When do you perform vitrectomy? What are the indications for evisceration/enucleation?
A:
Pars Plana Vitrectomy (PPV):
- Indicated when: no improvement after 48-72 hours of intravitreal antibiotics, severe vitreous involvement, vision better than light perception (EVS trial for post-cataract endophthalmitis), trauma-associated endophthalmitis/panophthalmitis, fungal cases
- Advantage: removes the infected vitreous scaffold, allows direct antibiotic delivery, provides sample for culture, possible visual rehabilitation
Evisceration (removal of intraocular contents, sclera retained):
- Panophthalmitis with no perception of light AND globe is intact
- Preferred over enucleation in active infection (lower risk of CNS spread through orbital tissues vs. cutting optic nerve)
- Allows fitting of orbital implant
- Contraindication: suspected intraocular malignancy (use enucleation then)
Enucleation (entire globe removed):
- When sclera is also destroyed or perforated
- Suspected intraocular tumor with panophthalmitis
- Failed evisceration
- Caution in panophthalmitis: cutting the optic nerve sheath may risk spread of infection to meninges and cavernous sinus
Exenteration (orbital contents removed):
- Rare, severe cases with fungal panophthalmitis (mucormycosis) with extensive orbital invasion, particularly in diabetic ketoacidosis
SECTION 7: Complications and Prognosis
Q10. What are the complications of panophthalmitis?
A:
Ocular:
- Permanent vision loss (most common)
- Phthisis bulbi (shrunken, atrophic, non-functional globe - end-stage)
- Corneal scarring/perforation
- Retinal detachment
- Cyclitic membrane
- Hypotony
- Secondary glaucoma
Orbital:
- Subperiosteal abscess
- Orbital abscess
Intracranial (life-threatening):
- Cavernous sinus thrombosis (high mortality)
- Meningitis
- Encephalitis
- Brain abscess
- Stroke (septic emboli)
Systemic:
- Septicemia
- Septic shock
- Death (rare with modern treatment but reported)
Q11. What is the visual prognosis of panophthalmitis?
A: Visual prognosis is typically poor even with timely treatment. Most patients either lose the eye or retain only light perception at best.
Factors affecting prognosis:
- Organism virulence (worst: Bacillus cereus, Streptococcus spp.; better: CoNS)
- Time to presentation and treatment (every hour matters)
- Route of infection (post-traumatic with soil > post-operative)
- Patient's immune status (immunocompromised fare worse)
- Extent of involvement at presentation
- Adequacy of initial treatment
Mortality from panophthalmitis itself is rare given modern antibiotics, but intracranial complications can be fatal.
SECTION 8: High-Yield Viva Points
Q12. What is the EVS trial and its relevance?
A: The Endophthalmitis Vitrectomy Study (EVS, 1995) studied POST-CATARACT SURGERY endophthalmitis (not panophthalmitis specifically):
- Immediate vitrectomy + intravitreal antibiotics was better than vitreous tap + intravitreal antibiotics ONLY in patients with light perception only (LP) - 3x better chance of achieving 20/40 vision
- In patients with hand motion (HM) or better vision, no significant difference between the two approaches
- Systemic antibiotics (IV amikacin + vancomycin) showed NO benefit over intravitreal alone
- Important: EVS excluded traumatic endophthalmitis/panophthalmitis - these are always managed aggressively with PPV
Q13. What is phthisis bulbi?
A: Phthisis bulbi is the final common pathway of end-stage ocular damage - a shrunken, atrophic, disorganized, non-functional eye resulting from severe inflammation (including panophthalmitis), trauma, or ischemia. Histologically shows disorganized intraocular structures, ossification, and scleral thickening. It is the feared end-stage outcome of untreated or treatment-resistant panophthalmitis.
Q14. A patient presents 3 days after cataract surgery with severe pain, complete loss of vision, proptosis, and ophthalmoplegia. What is your diagnosis and immediate management?
A:
- Diagnosis: Post-operative panophthalmitis (extension beyond endophthalmitis to orbital involvement)
- Distinguish from endophthalmitis: proptosis and ophthalmoplegia confirm orbital spread = panophthalmitis
Immediate management:
- Admit as emergency
- Blood cultures x2 stat
- CT orbit (thin cuts, with/without contrast) - assess orbital extension, foreign body
- Tap vitreous + aqueous simultaneously, send for Gram stain + culture
- Intravitreal vancomycin 2 mg/0.1 mL + ceftazidime 2 mg/0.1 mL IMMEDIATELY
- IV vancomycin + piperacillin-tazobactam
- Topical fortified antibiotics hourly + cycloplegics
- If no improvement in 48-72 hours: PPV
- If no light perception + failed medical management: evisceration
- Infectious disease consult
Q15. What are the differences between evisceration and enucleation and when do you choose each in panophthalmitis?
A:
| Evisceration | Enucleation | |
|---|---|---|
| What is removed | Intraocular contents (uvea, retina, vitreous, lens, cornea) | Entire globe including sclera |
| Sclera | Retained | Removed |
| Optic nerve | Preserved | Cut at orbital apex |
| Risk in infection | Preferred - no optic nerve cut, less risk of CNS spread | Risk of meningitis via optic nerve sheath |
| Cosmesis | Better (sclera holds implant, more natural movement) | Good with implant |
| Sensation | Better (ciliary nerves preserved) | Reduced |
| Contraindication | Intraocular tumor | Active severe infection (relative) |
| Panophthalmitis choice | First choice if sclera intact | When sclera perforated or tumor suspected |
Q16. A diabetic patient with liver abscess develops sudden painless loss of vision. What do you suspect and how would you manage?
A:
- Diagnosis: Endogenous panophthalmitis/endophthalmitis secondary to Klebsiella pneumoniae bacteremia (classic scenario in Asian diabetic patients with liver abscess)
- This syndrome is called Klebsiella liver abscess-associated endophthalmitis and is particularly common in Taiwan/Southeast Asia
Management:
- Admit for systemic infection control
- Blood cultures
- CT abdomen (confirm liver abscess), CT orbit
- Echo (rule out endocarditis)
- Vitreous tap + intravitreal antibiotics (ceftazidime covers Klebsiella well)
- IV third-generation cephalosporin (ceftriaxone) OR carbapenem
- Drainage of liver abscess (IR-guided)
- PPV if no improvement
- Prognosis is poor - most endogenous Klebsiella endophthalmitis results in loss of vision
Q17. What is the role of corticosteroids in panophthalmitis?
A: Controversial and carefully timed:
- Intravitreal dexamethasone (400 mcg/0.1 mL) - used by some alongside intravitreal antibiotics to reduce inflammatory damage, but not universally recommended
- Topical steroids - started AFTER 48 hours of confirmed antibiotic response, not initially (risk of worsening infection)
- Systemic steroids - generally avoided in active panophthalmitis due to immunosuppression risk
- Rationale for use: The inflammatory response itself (not just the organism) causes significant retinal damage; modulating it may preserve some visual function
- EVS trial did not include intravitreal steroids in its protocol
Q18. How does panophthalmitis due to Bacillus cereus present differently?
A: Bacillus cereus panophthalmitis is a surgical emergency with an extremely rapid course:
- Almost exclusively post-traumatic (soil, vegetation, organic material)
- Onset within 12-24 hours of injury
- Characterized by: ring corneal abscess (pathognomonic), rapid corneal perforation, severe hypopyon, total loss of vision often within 24-48 hours
- Produces potent toxins: metalloprotease, phospholipase C, cereulide - direct tissue destruction beyond inflammation
- Despite aggressive treatment, most eyes are lost
- Key management point: Aggressive PPV + intravitreal antibiotics as EMERGENCY, do not wait
Q19. What is the role of B-scan ultrasound in panophthalmitis?
A: B-scan USG is the most important bedside investigation when media opacity prevents fundal view:
- Shows: echogenic vitreous (vitritis), vitreous membranes, snowball opacities (fungal)
- Retinal detachment (flat or funnel-shaped)
- Choroidal thickening, choroidal detachment
- Subretinal/subchoroidal collections
- Posterior coats thickening (>2mm is significant for posterior scleritis/panophthalmitis)
- Can help plan vitrectomy approach
- Serial B-scans guide response to treatment
Q20. What systemic conditions predispose to endogenous panophthalmitis?
A:
- Diabetes mellitus (most common - Klebsiella, Candida, mucor)
- IV drug use (Candida, Bacillus, gram-negatives)
- Infective endocarditis (bacterial seeding)
- HIV/AIDS (Candida, CMV, Aspergillus)
- Immunosuppression (transplant, chemotherapy, biologics)
- Neonates (group B Streptococcus, gram-negatives)
- Chronic liver disease / liver abscess (Klebsiella pneumoniae)
- Post-sepsis / bacteremia from any source
- Indwelling IV catheters / TPN (Candida)
Quick-Reference Summary Card
| Topic | Key Point |
|---|---|
| Definition | All globe layers + orbit; = endophthalmitis + orbital cellulitis |
| Distinguishing sign | Proptosis + ophthalmoplegia (orbital involvement) |
| Most virulent organism | Bacillus cereus (post-trauma, soil) |
| Most common post-cataract | Staphylococcus epidermidis |
| Endogenous in diabetics | Klebsiella (liver abscess) |
| First treatment step | Tap + intravitreal vancomycin + ceftazidime |
| Intravitreal doses | Vancomycin 1-2 mg/0.1 mL + Ceftazidime 2 mg/0.1 mL |
| Fungal intravitreal | Voriconazole 100 mcg/0.1 mL |
| Surgery of choice | PPV → Evisceration (if sclera intact) → Enucleation |
| EVS trial relevance | Immediate PPV for LP only; no benefit of systemic antibiotics |
| End-stage | Phthisis bulbi |
| Worst complication | Cavernous sinus thrombosis, meningitis |
| Prognosis | Poor even with timely treatment |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p.1216 - definition and pathology of endophthalmitis vs panophthalmitis
- Kanski's Clinical Ophthalmology, 10th ed. - intravitreal antibiotic protocols
- Wills Eye Manual - clinical signs and differential diagnosis
- EyeWiki - Panophthalmitis - comprehensive clinical reference
- Tintinalli's Emergency Medicine - orbital complications
This is a shared conversation. Sign in to Orris to start your own chat.