Inj. Amikacin uses
Reading File
Finding Sources
Searching the Web
Amikacin injection uses indications clinical
Finding Sources
Reading Web Page
https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?set…
Finding Sources
Reading File
Excellent - I now have comprehensive information from Goodman & Gilman's. Here is the full, detailed answer:
Injection Amikacin - Uses & Clinical Overview
Drug Class
Amikacin is an aminoglycoside antibiotic that inhibits bacterial protein synthesis by binding to the 30S ribosomal subunit, causing misreading of mRNA and accumulation of abnormal initiation complexes. It has concentration-dependent bactericidal activity.
Antibacterial Spectrum
Primary activity: Aerobic Gram-negative bacilli
- Pseudomonas aeruginosa
- Escherichia coli
- Klebsiella pneumoniae
- Enterobacter species
- Serratia species
- Proteus species (indole-positive and indole-negative)
- Providencia species
- Acinetobacter species
- Citrobacter freundii
Special advantage: Amikacin and plazomicin are the most active aminoglycosides against multidrug-resistant (MDR) organisms because amikacin resists most plasmid-mediated inactivating enzymes that destroy gentamicin and tobramycin. This makes it valuable when other aminoglycosides have failed or for MDR/XDR gram-negative infections.
Gram-positive activity: Effective against Staphylococcus aureus infections - can be used in patients allergic to other antibiotics or in mixed gram-negative/staphylococcal infections.
Clinical Indications
1. Bacterial Septicemia (including Neonatal Sepsis)
- First-line option in neonatal sepsis (often combined with ampicillin or a penicillin)
- Serious gram-negative bacteremia
2. Respiratory Tract Infections
- Hospital-acquired pneumonia (HAP) / ventilator-associated pneumonia (VAP)
- Gram-negative pneumonia
- MDR Pseudomonas lung infections (especially cystic fibrosis patients)
- Refractory Mycobacterium avium complex (MAC) lung disease (inhaled liposomal form)
3. Urinary Tract Infections (UTIs)
- Complicated and recurrent UTIs due to resistant gram-negative organisms
- NOT indicated for uncomplicated initial UTI unless causative organisms are resistant to less toxic alternatives
- Dose for uncomplicated UTI: 250 mg twice daily
4. Bone and Joint Infections
- Osteomyelitis due to gram-negative organisms
- Septic arthritis
5. Central Nervous System Infections
- Bacterial meningitis (gram-negative meningitis)
- CNS infections in neonates
6. Intra-abdominal Infections
- Peritonitis
- Post-operative abdominal sepsis
7. Skin and Soft Tissue Infections
- Serious gram-negative skin infections
- Burns (post-burn infections)
8. Post-operative Infections
- Post-vascular surgery infections
- Wound infections with resistant gram-negative pathogens
9. MDR / XDR Gram-negative Infections
- Carbapenem-resistant Enterobacteriaceae (CRE)
- Organisms resistant to gentamicin/tobramycin due to plasmid-mediated enzymes - amikacin retains activity because its unique structural characteristics protect it from most aminoglycoside-inactivating enzymes
- Combination therapy for extended-spectrum beta-lactamase (ESBL)-producing organisms
10. Tuberculosis (MDR-TB)
- Part of second-line regimens for multidrug-resistant tuberculosis
Dosage (Normal Renal Function)
| Route | Dose | Frequency |
|---|---|---|
| IV / IM | 15 mg/kg/day | Divided q8-12h (7.5 mg/kg q12h or 5 mg/kg q8h) |
| Once-daily dosing | 15-20 mg/kg | q24h (preferred for efficacy and reduced toxicity) |
| Neonates | 7.5 mg/kg | q12h |
| Uncomplicated UTI | 250 mg | q12h |
Maximum dose: 1.5 g/day (15 g total course)
Key Adverse Effects (Monitor Closely)
- Nephrotoxicity - dose and duration dependent; monitor renal function (creatinine, BUN)
- Ototoxicity - both cochlear (hearing loss) and vestibular; amikacin is the most cochleotoxic of the aminoglycosides
- Neuromuscular blockade - rare; risk with concurrent neuromuscular blocking agents
Important Pharmacokinetic Considerations
- Not orally bioavailable - must be given IV or IM
- Concentration-dependent killing - higher peak/MIC ratios = better bactericidal effect
- Eliminated renally (dose adjustment required in renal impairment)
- Therapeutic drug monitoring (TDM): monitor peak and trough levels
- Target peak (conventional dosing): 20-35 mcg/mL
- Target trough: <5 mcg/mL
When to Choose Amikacin Over Other Aminoglycosides
Choose amikacin specifically when:
- Gram-negative organisms are resistant to gentamicin or tobramycin
- MDR/carbapenem-resistant organisms are suspected
- Healthcare-associated infections in units with high aminoglycoside resistance rates
- Combination therapy for Pseudomonas or Acinetobacter infections
(Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics; FDA/DailyMed Amikacin Sulfate Injection Prescribing Information)
Rifagut
Finding Sources
Searching the Web
Rifagut rifaximin uses indications dosage
Reading File
Finding Sources
I have comprehensive data. Here is the full answer:
Rifagut (Rifaximin) - Complete Overview
What is Rifagut?
Rifagut is the brand name for Rifaximin, a rifamycin-derived antibiotic. It is available as 200 mg and 550 mg tablets. The key distinguishing feature is that it is minimally absorbed from the gut (<0.5% systemic absorption), resulting in very high fecal concentrations - making it a "gut-selective" antibiotic.
Mechanism of Action
- Derivative of rifampin (rifamycin class)
- Inhibits bacterial RNA synthesis by binding to the beta subunit of DNA-dependent RNA polymerase
- Active against both gram-positive and gram-negative aerobes and anaerobes
- After a 3-day course, fecal concentrations reach ~8000 mcg/g - far exceeding the MIC for most gut pathogens
FDA-Approved Indications
1. Traveler's Diarrhea (TD)
- Caused by non-invasive strains of E. coli (ETEC)
- Dose: 200 mg three times daily for 3 days
- Important: NOT for use when diarrhea is complicated by fever, blood in stool, or suspected invasive pathogens (Campylobacter, Salmonella, Shigella) - rifaximin should not be used for bloody diarrhea
2. Hepatic Encephalopathy (HE) - Prevention of Recurrence
- Reduces the risk of recurrent overt hepatic encephalopathy in adults with liver cirrhosis
- Used as adjunct to or in combination with lactulose
- Dose: 550 mg twice daily (long-term, ongoing use)
- Mechanism: reduces ammonia-producing gut bacteria, modulates intestinal microbial function (rather than changing microbial composition)
3. Irritable Bowel Syndrome with Diarrhea (IBS-D)
- Dose: 550 mg three times daily for 14 days
- Can be retreated with up to 2 more courses if symptoms recur
- Meta-analysis (5 studies): more efficacious than placebo for global IBS symptom improvement (OR 1.57; NNT ~10)
- Acts by modulating gut flora (decreases Enterobacteriaceae and Verrucomicrobiaceae)
Off-Label / Additional Uses
| Indication | Notes |
|---|---|
| Recurrent C. difficile infection | Adjunct in refractory/recurrent cases |
| Small intestinal bacterial overgrowth (SIBO) | Commonly used; 400-550 mg TID x 7-14 days |
| Prevention of spontaneous bacterial peritonitis (SBP) | In cirrhotic patients with HE |
| Diverticulitis prevention | Cyclic rifaximin (1 week/month) + fiber reduces recurrence |
| Crohn's disease | Investigational; some evidence for luminal activity |
| Pouchitis | Inflammation after ileal pouch surgery |
Dosage Summary
| Indication | Dose | Duration |
|---|---|---|
| Traveler's diarrhea | 200 mg TID | 3 days |
| Hepatic encephalopathy | 550 mg BD | Long-term / indefinite |
| IBS-D | 550 mg TID | 14 days (up to 3 courses) |
| SIBO (off-label) | 400-550 mg TID | 7-14 days |
Key Pharmacological Advantages
- Minimal systemic absorption (<0.5%) = very low systemic side effects
- No CYP450-mediated drug interactions (unlike other rifamycins such as rifampin which are potent CYP inducers)
- Low risk of systemic resistance - resistance development in extra-intestinal bacteria is minimal
- Safe in hepatic impairment for gut indications (no hepatic metabolism concerns for efficacy)
Side Effects (Generally Well Tolerated)
- Nausea
- Abdominal pain / bloating
- Flatulence
- Headache
- Peripheral edema (seen with HE dosing)
- Rarely: hypersensitivity reactions
Contraindications
- Hypersensitivity to rifaximin or other rifamycins
- Diarrhea complicated by fever or blood in stool (traveler's diarrhea indication)
- Suspected invasive enteropathogens (Salmonella, Shigella, Campylobacter)
Important Clinical Note
Unlike rifampin, rifaximin does not induce cytochrome P450 enzymes and does not cause the red-orange discoloration of body fluids. It is essentially a "local" gut antibiotic - this is what makes Rifagut suitable for long-term use in conditions like hepatic encephalopathy.
(Sources: Katzung's Basic & Clinical Pharmacology 16th Ed.; Yamada's Textbook of Gastroenterology; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E)
Create a treatment guide for IBS-D management
Asking for Preferences
Finding Sources
Finding Sources
Searching the Web
IBS-D irritable bowel syndrome diarrhea treatment guidelines 2024 2025
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have comprehensive data from multiple authoritative textbooks plus a treatment algorithm image. Here is the complete clinical treatment guide:
IBS-D (Irritable Bowel Syndrome with Diarrhea) - Treatment Guide for Clinicians
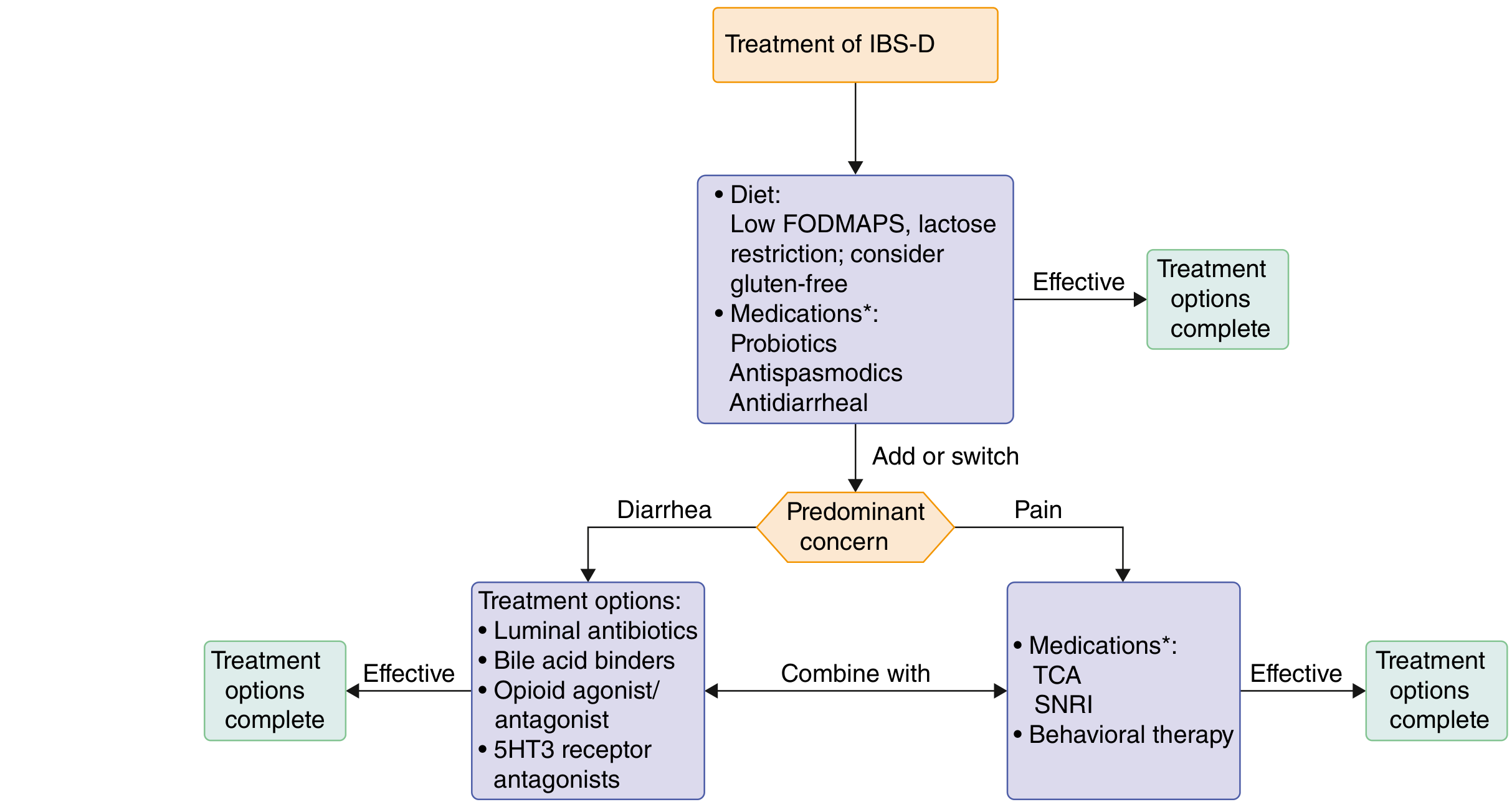
Treatment Algorithm
The flowchart below (from Goldman-Cecil Medicine) provides the overall treatment framework:
Step 1 - Establish Diagnosis (Rome IV Criteria)
Recurrent abdominal pain on average at least 1 day per week in the last 3 months, associated with ≥2 of the following:
- Related to defecation
- Associated with a change in stool frequency
- Associated with a change in stool form/appearance
- Onset of symptoms at least 6 months before diagnosis
- IBS-D subtype: >25% of stools are loose/watery and <25% are hard/lumpy
Exclude alarm features before labeling as IBS-D: rectal bleeding, weight loss, nocturnal symptoms, family history of colorectal cancer/IBD, age >50 with new onset, iron-deficiency anemia. If present, investigate further.
Step 2 - Non-Pharmacological Measures (Start Here)
Dietary Interventions
| Intervention | Evidence | Recommendation |
|---|---|---|
| Low FODMAP diet | Strong | ACG, AGA recommended - reduces fermentable carbohydrates (oligosaccharides, disaccharides, monosaccharides, polyols) |
| Lactose restriction | Moderate | Trial in patients with suspected lactose intolerance |
| Gluten-free diet | Moderate | Consider in refractory cases even without celiac disease |
| Soluble fiber (psyllium/ispaghula) | Moderate (NNT=7) | Can help regulate bowel habit; increase dose gradually to minimize bloating |
| Avoid bran | - | Bran can worsen IBS symptoms; not recommended |
| Caffeine restriction | Low | Limit to <3 cups/day; caffeine accelerates gut transit |
Lifestyle Measures
- Regular physical activity (improves bowel regularity and psychological well-being)
- Stress identification and reduction
- Regular meal times (avoid skipping meals)
- Keep a food and symptom diary to identify personal triggers
- Adequate hydration
Step 3 - Pharmacological Management
A. For Predominant Diarrhea
1. Loperamide (First-Line for Mild IBS-D)
- Peripheral μ-opioid receptor agonist
- Reduces stool frequency and urgency
- Dose: Up to 4 mg four times daily (titrate to effect)
- Limitation: Does NOT improve global IBS symptoms or abdominal pain - best for patients whose primary complaint is stool frequency with mild pain
- Safe for long-term use; no systemic opioid effects
2. Rifaximin (First-Line for IBS-D with Bloating)
- Minimally absorbed gut antibiotic; modulates intestinal microbiota
- Dose: 550 mg three times daily for 14 days
- Up to 3 retreatment courses for relapse
- Improves global symptoms, bloating, stool consistency
- Meta-analysis: OR 1.57 vs placebo for global symptom improvement (NNT ~10)
- Well tolerated; side effects: nausea, abdominal pain
- Preferred when bloating is a prominent feature
3. Eluxadoline (IBS-D with Pain + Diarrhea)
- Mixed opioid: μ/κ-receptor agonist + δ-receptor antagonist
- Addresses both diarrhea and abdominal pain
- Dose: 100 mg twice daily (reduce to 75 mg BD if not tolerated)
- Contraindications: Absence of gallbladder, biliary duct obstruction, sphincter of Oddi dysfunction, pancreatic disease, hepatic impairment (mild-moderate), alcohol use disorder
- Side effects: nausea, constipation, rare pancreatitis
4. Bile Acid Sequestrants (If Bile Acid Diarrhea suspected)
- ~25-30% of IBS-D patients have underlying bile acid malabsorption
- Test: fecal bile acid levels (if available); or trial empirically
- Agents: Cholestyramine (4 g TID), Colesevelam (1.875 g BD), Colestipol
- Consider in IBS-D patients who have had cholecystectomy or small bowel disease
5. Alosetron (Severe, Refractory IBS-D in Women - REMS Required)
- 5-HT3 receptor antagonist; slows colonic transit and reduces visceral hypersensitivity
- Dose: 0.5 mg twice daily (start low); increase to 1 mg twice daily after 4 weeks if tolerated
- Consistent efficacy in high-quality RCTs; also evidence in men (lower grade)
- Restricted use (REMS program): only for women with severe IBS-D refractory to conventional therapy
- Risks: Ischemic colitis (1.1/1000 patient-years), serious complications of constipation (0.66/1000 patient-years) - monitor closely; discontinue if constipation develops
- ACG/AGA conditional recommendation (Grade 2B-2C)
B. For Predominant Abdominal Pain / Cramping
1. Antispasmodics (For Postprandial Pain and Cramping)
- Reduce GI spasm and motility
- Hyoscyamine: 0.125-0.25 mg sublingual/oral before meals or as needed
- Dicyclomine: 20 mg QID (antimuscarinic)
- Mebeverine: 135-200 mg TID (direct smooth muscle relaxant, fewer anticholinergic effects)
- Side effects: dry mouth, drowsiness, urinary retention (anticholinergic)
- Use before meals for meal-triggered symptoms
2. Gut-Brain Neuromodulators (Central Sensitization / Chronic Pain)
| Drug | Class | Dose | Notes |
|---|---|---|---|
| Amitriptyline | TCA | 10-75 mg at night | Slows gut transit; good for diarrhea-predominant pain; start low (10 mg), titrate |
| Nortriptyline | TCA | 10-75 mg at night | Similar to amitriptyline; slightly fewer side effects |
| Duloxetine | SNRI | 30-60 mg daily | Good for comorbid anxiety/depression + IBS-D |
| Venlafaxine | SNRI | 37.5-75 mg daily | May accelerate transit at higher doses - use cautiously in diarrhea |
- TCAs preferred in IBS-D (anticholinergic effect slows transit, reduces diarrhea)
- SNRIs preferred when comorbid depression/anxiety is present
- Treat as neuromodulators, not antidepressants - explain this to patients; effects independent of psychiatric action
3. Peppermint Oil
- Natural smooth muscle relaxant (calcium channel blocker effect in gut)
- Enteric-coated capsules: 0.2-0.4 mL (1-2 capsules) TID before meals
- Evidence for global IBS symptom improvement; well tolerated
- Side effects: heartburn (use enteric-coated formulation to minimize)
C. Adjunctive Therapies
Probiotics
- Evidence is mixed; no single strain consistently recommended
- Some benefit for bloating and flatulence
- Bifidobacterium-containing products have the best evidence
- Trial for 4-8 weeks; discontinue if no benefit
Psychological / Behavioral Therapies
Recommended for moderate-severe IBS-D, especially when:
- Symptoms clearly triggered or worsened by stress
- Comorbid anxiety or depression
- Inadequate response to pharmacological therapy
| Therapy | Evidence |
|---|---|
| Cognitive-Behavioral Therapy (CBT) | Strong; reduces maladaptive thought patterns, emotional awareness training |
| Gut-Directed Hypnotherapy | Strong; particularly effective for visceral hypersensitivity |
| Mindfulness-based therapy | Moderate |
| Relaxation training | Moderate |
| Psychotherapy / Psychodynamic therapy | Moderate |
Step 4 - Combining Treatments Based on Predominant Concern
As illustrated in the treatment algorithm above:
- If diarrhea is the predominant concern - prioritize: luminal antibiotics (rifaximin), bile acid binders, opioid agonist/antagonist (eluxadoline/loperamide), or 5-HT3 antagonists (alosetron)
- If pain is the predominant concern - prioritize: TCAs, SNRIs, behavioral therapy
- For both - combine treatments targeting each concern simultaneously
Pharmacological Summary Table
| Drug | Mechanism | Dose | Target Symptom | Grade |
|---|---|---|---|---|
| Loperamide | μ-opioid agonist | Up to 4 mg QID | Diarrhea only | ACG 2C |
| Rifaximin | Gut antibiotic / microbiome modulator | 550 mg TID x 14 days | Diarrhea + bloating | ACG 1B |
| Eluxadoline | μ/κ agonist + δ antagonist | 100 mg BD | Diarrhea + pain | ACG 1B |
| Alosetron | 5-HT3 antagonist | 0.5-1 mg BD | Severe IBS-D (women) | ACG 2B |
| Bile acid sequestrants | Binds bile acids | Variable | Bile acid diarrhea | ACG 2C |
| Antispasmodics | Antimuscarinic / smooth muscle | Variable | Cramping/pain | ACG 2C |
| TCAs (amitriptyline) | Neuromodulator + anti-transit | 10-75 mg nocte | Pain + diarrhea | ACG 1A |
| SNRIs (duloxetine) | Central/peripheral neuromodulator | 30-60 mg daily | Pain + mood | ACG 2C |
| Peppermint oil | Smooth muscle relaxant | 0.2-0.4 mL TID | Global symptoms | ACG 1B |
| CBT / Hypnotherapy | Gut-brain axis modulation | Structured sessions | Global + psych comorbidity | ACG 1A |
Monitoring and Follow-Up
- Reassess at 4-6 weeks after initiating new treatment
- Use validated symptom scoring tools: IBS-SSS (Symptom Severity Score) or IBS-QOL
- If no response after adequate trial, switch or add another class
- Rifaximin: retreatment with up to 3 courses is safe and effective for relapse
- For alosetron: stop immediately if constipation develops or rectal bleeding occurs
- Eluxadoline: monitor for pancreatitis (abdominal pain radiating to back)
- TCAs: monitor for anticholinergic effects; check for urinary retention in elderly males
When to Refer
- Gastroenterology: diagnostic uncertainty, alarm features, refractory IBS-D, consideration of alosetron
- Dietitian: low FODMAP diet implementation (requires structured guidance for proper reintroduction phase)
- Psychologist/Psychiatrist: CBT, gut-directed hypnotherapy, significant psychological comorbidity
(Sources: Goldman-Cecil Medicine; Yamada's Textbook of Gastroenterology 7th Ed.; Lippincott Illustrated Reviews Pharmacology; Katzung's Basic & Clinical Pharmacology 16th Ed.; Harrison's Principles of Internal Medicine 22E)
This is a shared conversation. Sign in to Orris to start your own chat.