I now have comprehensive content from Guyton. Let me compile the full masterclass lecture:
🔬 CELL PHYSIOLOGY - COMPLETE MASTERCLASS
Guyton & Hall | The Orris Elite Physiology Series
From Absolute Basics to Advanced Clinical Mastery
Before we begin: Think of a cell the way you think of a city. It has a boundary wall (cell membrane), a power plant (mitochondria), a post office (Golgi), a factory (ribosomes), a library (nucleus), and a waste management system (lysosomes). Everything in physiology - every disease, every drug, every clinical sign - starts here.
━━━━━━━━━━━━━━━━━━━━
STAGE 1: BIG PICTURE
━━━━━━━━━━━━━━━━━━━━
Why Does Cell Physiology Exist?
The human body contains 35 to 40 trillion cells (Guyton, Chapter 2). Every organ, every tissue, every physiological function you will ever study is ultimately a scaled-up version of what individual cells do. You cannot understand why the heart beats, why kidneys make urine, why nerves transmit signals, or why insulin lowers blood sugar unless you first understand what happens at the cell level.
Guyton's famous principle: "The entire human body is an aggregate of trillions of cells, each adapted to perform specific functions." The health of the organism = the health of each cell.
Role in Homeostasis
The cell is the fundamental unit of homeostasis. Every cell:
- Senses changes in its environment
- Responds to those changes
- Communicates with neighboring cells
- Maintains its internal chemical composition despite external fluctuations
The internal environment of the cell (intracellular fluid, ICF) must be kept within narrow limits. The moment a cell loses control of its internal environment - through ion imbalance, energy failure, or membrane damage - it dies, and disease follows.
How It Connects to Everything
| System | Cell Physiology Connection |
|---|
| Nervous system | Action potentials = Na+/K+ ion movements across nerve cell membranes |
| Cardiac physiology | Cardiac contraction = Ca²+ signaling + ion channel gating |
| Renal physiology | Tubular transport = active transport pumps in renal cells |
| Endocrine | Hormone action = receptor binding on cell membrane or inside cell |
| GI absorption | Nutrient absorption = co-transport mechanisms in intestinal cells |
| Pharmacology | Every drug ultimately works by binding to a receptor/channel/pump on a cell |
Real-Life Importance
- Digitalis (digoxin) for heart failure works by blocking the Na+/K+ ATPase pump
- Loop diuretics (furosemide) block the Na+/K+/2Cl- co-transporter in renal tubular cells
- Local anesthetics (lidocaine) block Na+ channels in nerve cells
- Cholera kills by activating adenylyl cyclase in intestinal cells, flooding the gut with Cl- and water
Everything clinical traces back here.
━━━━━━━━━━━━━━━━━━━━
STAGE 2: BASIC FOUNDATION
━━━━━━━━━━━━━━━━━━━━
Key Definitions
| Term | Definition |
|---|
| Cell | The basic structural and functional unit of life |
| Protoplasm | The total living material of a cell (nucleus + cytoplasm) |
| Cell membrane (plasma membrane) | The outer boundary of the cell - 7.5 to 10 nm thick |
| Cytoplasm | Everything inside the cell except the nucleus |
| Organelle | Specialized subunit within the cell with specific functions |
| Homeostasis | Maintenance of a stable internal environment |
| Intracellular fluid (ICF) | Fluid inside the cell (~67% of body fluid) |
| Extracellular fluid (ECF) | Fluid outside the cell (~33% of body fluid) |
Composition of Protoplasm (from Guyton)
| Component | Percentage | Role |
|---|
| Water | 70-85% | Solvent; medium for reactions |
| Proteins | 10-20% | Structural + functional (enzymes) |
| Lipids | ~2% | Membrane structure |
| Carbohydrates | ~1% | Energy, cell recognition |
| Electrolytes | Small amounts | Electrical signaling, enzyme function |
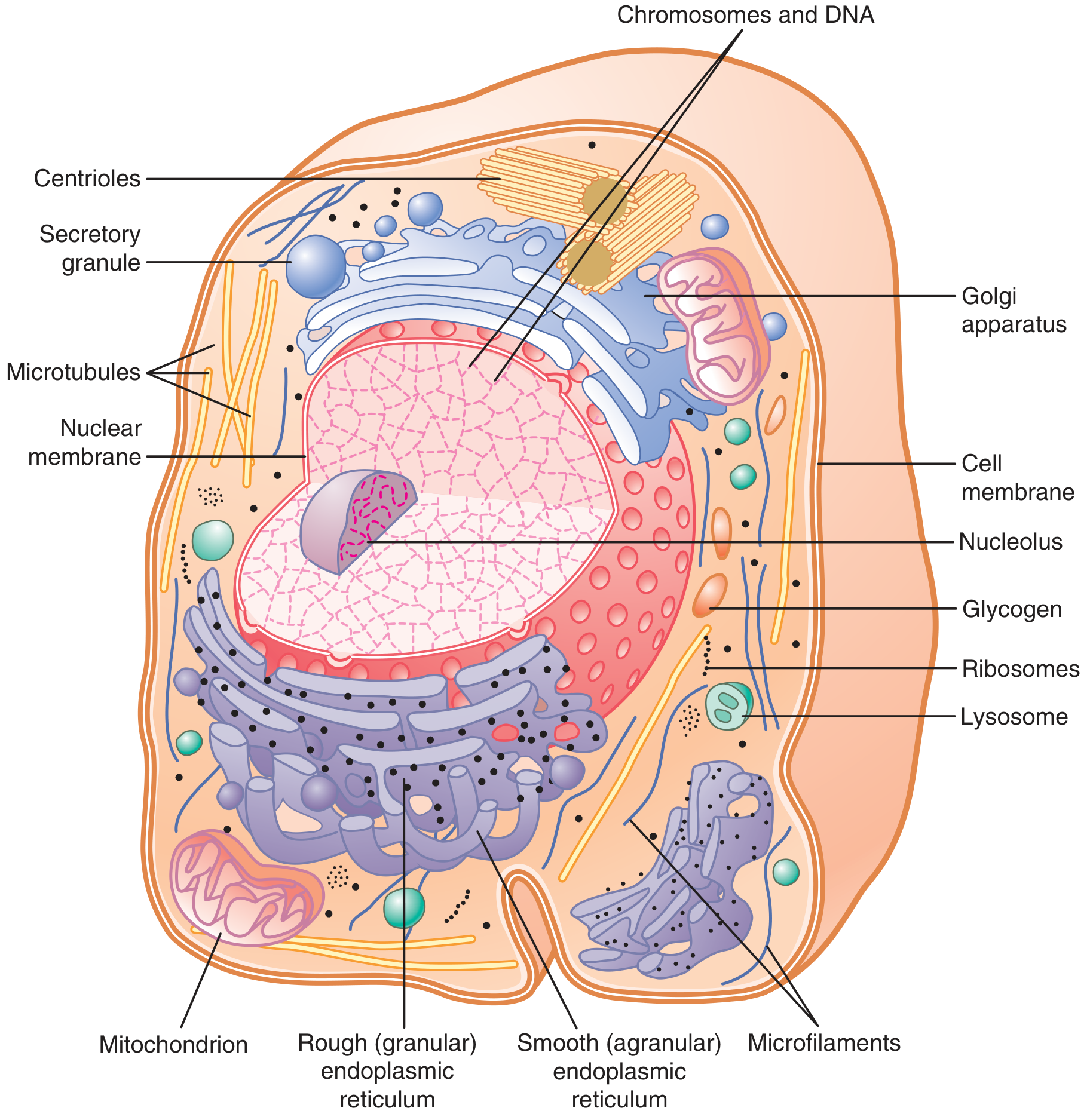
Cell Structure Overview (Guyton Fig. 2.2)
Here is the actual cell diagram from Guyton & Hall:
Figure 2.2 from Guyton & Hall - Reconstruction of a typical cell showing all internal organelles
Organelle-by-Organelle Breakdown
1. The Cell Membrane (Plasma Membrane)
- Thickness: 7.5-10 nanometers
- Composition: 55% proteins, 25% phospholipids, 13% cholesterol, 4% other lipids, 3% carbohydrates
- Structure: Fluid mosaic model - phospholipid bilayer with embedded proteins
- Key property: Selectively permeable
Why phospholipids form a bilayer: Each phospholipid has a hydrophilic (water-loving) head and two hydrophobic (water-fearing) fatty acid tails. In water, they automatically arrange themselves so:
Water (outside)
[ Head Head Head Head Head ] ← hydrophilic heads face water
[ Tail Tail Tail Tail Tail ] ← hydrophobic tails hide from water
[ Tail Tail Tail Tail Tail ]
[ Head Head Head Head Head ]
Water (inside)
This bilayer arrangement is thermodynamically spontaneous - nature favors it.
Role of cholesterol: Inserted between phospholipids, it:
- Prevents the membrane from becoming too rigid in cold
- Prevents it from becoming too fluid in heat
- Maintains just the right fluidity (think of cholesterol as the "shock absorber" of the membrane)
Membrane Proteins (2 types):
- Integral proteins (intrinsic): Penetrate deep into or entirely through the membrane. Functions: transport channels, carrier proteins, receptor proteins, enzyme proteins, structural anchor proteins
- Peripheral proteins (extrinsic): Attached to surface, do not penetrate. Functions: enzymes, cell signaling, structural support
2. The Nucleus
- Master controller of the cell
- Contains DNA organized into chromosomes (46 in human somatic cells)
- Contains nucleolus: the site of ribosomal RNA (rRNA) synthesis
- Surrounded by nuclear membrane (double membrane with pores)
- Nuclear pores allow passage of mRNA, proteins, ions
Function: DNA → mRNA (transcription in nucleus) → protein (translation in cytoplasm on ribosomes)
3. Mitochondria - The Powerhouse
- Double membrane: outer smooth + inner folded (cristae)
- Cristae = site of ATP synthesis (electron transport chain + oxidative phosphorylation)
- Matrix = contains enzymes for Krebs cycle, fatty acid oxidation
- Contains its own DNA (mitochondrial DNA - maternal inheritance)
- Number varies by cell energy demand: muscle cells = thousands; red blood cells = zero
- ATP yield: 1 glucose → ~30-32 ATP molecules
Clinical pearl: Mitochondrial diseases (e.g., MELAS syndrome) cause muscle weakness, neurological defects, and lactic acidosis because cells cannot produce enough ATP.
4. Endoplasmic Reticulum (ER)
| Feature | Rough ER | Smooth ER |
|---|
| Ribosomes | Present (dotted appearance) | Absent |
| Function | Protein synthesis + initial processing | Lipid synthesis, drug detoxification, Ca²+ storage |
| Location | Near nucleus | Throughout cytoplasm |
| Clinical relevance | Antibody production (plasma cells have huge RER) | Steroid hormone synthesis (adrenal cortex, gonads) |
5. Golgi Apparatus
- The post office of the cell
- Receives proteins from RER, modifies them (adds sugars = glycosylation), packages them
- Creates secretory granules, lysosomes, membrane vesicles
- Proteins destined for export → secretory vesicles → exocytosis
- Proteins destined for digestion → lysosomes
6. Lysosomes
- Membrane-bound sacs containing ~40 hydrolytic enzymes
- pH inside: ~5 (acidic - enzymes work best here)
- Digest: worn-out organelles (autophagy), phagocytosed bacteria, pinocytosed materials
- "Suicide bags" of the cell - if membrane ruptures, enzymes digest the cell itself
Clinical pearl - Lysosomal storage diseases:
When a lysosomal enzyme is missing, undigested material accumulates → cell swells → organ dysfunction:
- Gaucher's disease: Glucocerebrosidase deficiency → glucocerebroside accumulates in macrophages (liver, spleen, bone marrow)
- Tay-Sachs disease: Hexosaminidase A deficiency → GM2 ganglioside accumulates in neurons → neurodegeneration
- Hurler's syndrome: α-L-iduronidase deficiency → mucopolysaccharide accumulation
7. Ribosomes
- Made of rRNA + protein (two subunits: large 60S + small 40S = 80S total in eukaryotes)
- Free ribosomes: Synthesize proteins for use inside the cell (cytoplasmic proteins, enzymes)
- Bound ribosomes (on RER): Synthesize proteins for secretion or membrane insertion
- Prokaryote ribosomes = 70S (target of many antibiotics: aminoglycosides, macrolides, tetracyclines, chloramphenicol block bacterial ribosomes but not human 80S - this is why these antibiotics are selective)
8. Cell Cytoskeleton
Three types:
| Type | Diameter | Composition | Function |
|---|
| Microfilaments | 5-9 nm | Actin | Cell movement, muscle contraction |
| Intermediate filaments | 10 nm | Keratin, vimentin, desmin | Mechanical support |
| Microtubules | 25 nm | Tubulin | Cell shape, intracellular transport, cilia/flagella, mitotic spindle |
Clinical pearl - Colchicine (for gout) binds tubulin and prevents microtubule polymerization, stopping neutrophil migration (anti-inflammatory) and blocking mitosis.
Vincristine/Vinblastine (cancer chemotherapy) also block microtubule function to stop cancer cell division.
9. Centrioles
- Paired structures near the nucleus
- Made of microtubules
- Organize the mitotic spindle during cell division
- Form the base of cilia and flagella (basal bodies)
Kartagener's Syndrome: Defect in dynein (ciliary motor protein) → immotile cilia → bronchiectasis, recurrent respiratory infections, situs inversus (organs reversed), male infertility (immotile sperm)
━━━━━━━━━━━━━━━━━━━━
STAGE 3: CORE PHYSIOLOGY - MEMBRANE TRANSPORT
━━━━━━━━━━━━━━━━━━━━
This is the most clinically important section of cell physiology. Every drug, every electrolyte imbalance, every organ function depends on how substances cross cell membranes.
The Transport Problem
The cell membrane is a lipid bilayer. Lipids are hydrophobic. So:
- Fat-soluble substances (O₂, CO₂, steroid hormones, alcohol) cross freely - no help needed
- Water-soluble substances (glucose, amino acids, ions, drugs) CANNOT cross freely - need help
The cell has solved this problem with protein transporters.
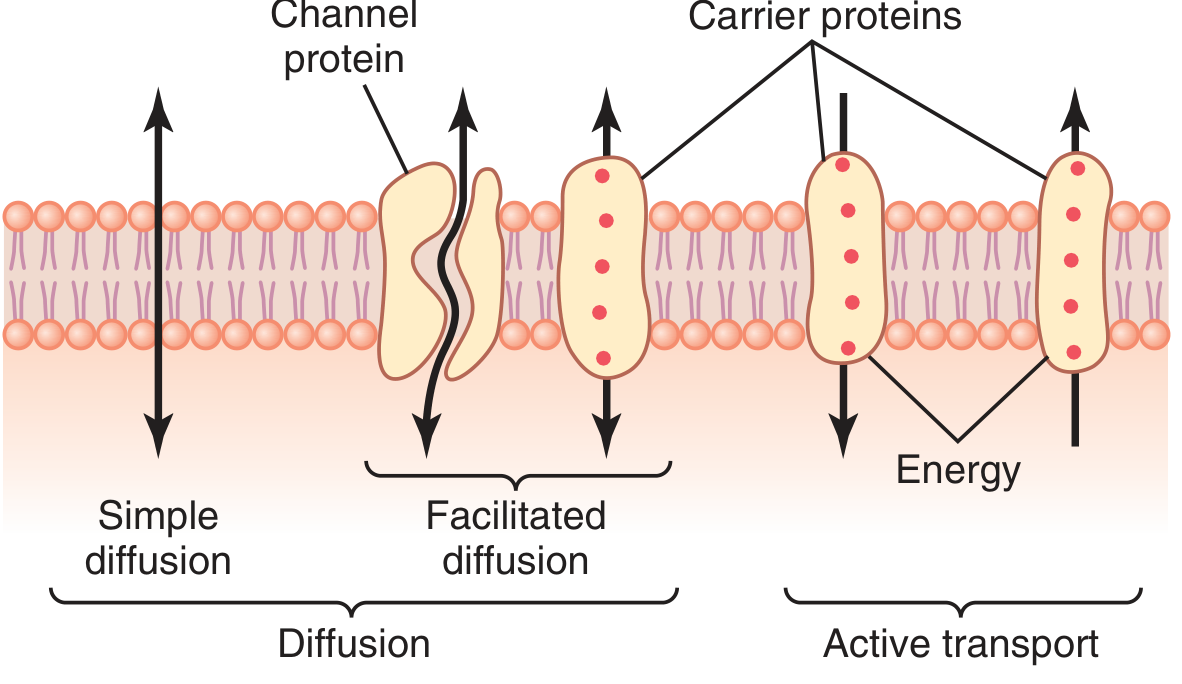
Transport Transport Transport: The Master Map
MEMBRANE TRANSPORT
├── DIFFUSION (No energy needed - moves WITH gradient)
│ ├── Simple Diffusion
│ │ ├── Through lipid bilayer (fat-soluble substances)
│ │ └── Through protein channels (water, ions)
│ └── Facilitated Diffusion (carrier proteins, still WITH gradient)
│
└── ACTIVE TRANSPORT (Energy needed - moves AGAINST gradient)
├── Primary Active Transport (directly uses ATP)
│ ├── Na+/K+ ATPase pump
│ ├── Ca²+ ATPase pump
│ └── H+/K+ ATPase pump
└── Secondary Active Transport (uses Na+ gradient created by Na+/K+ ATPase)
├── Co-transport (symport) - Na+ and solute move same direction
└── Counter-transport (antiport) - Na+ and solute move opposite directions
Here is the Guyton diagram showing all these pathways:
Figure 4.2 from Guyton & Hall - The complete spectrum of membrane transport mechanisms
A. SIMPLE DIFFUSION
What is it?
Random movement of molecules from high concentration to low concentration, powered entirely by the kinetic energy of molecules (thermal motion). No energy input from the cell required.
Fick's Law of Diffusion (The Governing Equation)
Net Rate of Diffusion ∝ (Concentration Difference × Membrane Area × Lipid Solubility)
────────────────────────────────────────────────────────────
(Membrane Thickness × Molecular Size)
In simple terms:
- Increases if: Higher concentration difference, larger membrane area, more lipid-soluble substance, thinner membrane, smaller molecule
- Decreases if: Smaller concentration difference, smaller area, water-soluble substance, thicker membrane, larger molecule
Two Sub-types of Simple Diffusion:
1. Diffusion through the lipid bilayer (for lipid-soluble substances):
- O₂ (critical for respiration)
- CO₂ (critical for gas exchange)
- N₂ (important in decompression sickness)
- Steroid hormones (cortisol, testosterone, estrogen, progesterone, aldosterone)
- Thyroid hormones
- Alcohol, anesthetic gases (halothane, isoflurane)
- Fat-soluble vitamins: A, D, E, K
- Urea (partially)
2. Diffusion through protein channels (for water + selected ions):
Channel proteins form water-filled pores through which water molecules and small, charged ions move at high speed.
Key properties of ion channels:
- Selective: K+ channels allow K+ but not Na+ (and vice versa) - determined by the size of the channel pore and the charge lining
- Gated: Can be open or closed, controlled by:
- Voltage-gated channels: Opened/closed by membrane potential change (Na+ channels in nerve action potential)
- Ligand-gated channels: Opened by a chemical binding (acetylcholine receptor at neuromuscular junction)
- Mechanically gated: Opened by physical deformation (hearing - hair cells in cochlea)
Aquaporins (discovered by Peter Agre, Nobel Prize 2003) are specialized water channels:
- Allow ~3 billion water molecules/second to pass through each channel
- AQP2 in collecting duct is regulated by ADH (vasopressin) - critical for urine concentration
B. FACILITATED DIFFUSION
What is it?
Diffusion with help of carrier proteins. Still moves WITH the concentration gradient (no ATP needed), but uses a specific carrier protein that undergoes conformational change.
Mechanism (Step by Step):
Molecule approaches membrane from high-concentration side
↓
Binds to specific site on carrier protein
↓
Carrier protein changes shape (conformational change)
↓
Molecule is released on the other side (low concentration)
↓
Carrier returns to original shape - ready for next molecule
Key Examples:
| Transporter | Substance Transported | Location | Clinical Relevance |
|---|
| GLUT-1 | Glucose | RBCs, brain, fetal tissue | Always expressed (basal glucose uptake) |
| GLUT-2 | Glucose + fructose | Liver, pancreatic β-cells, kidney, intestine | Low affinity - sensor of blood glucose in β-cells |
| GLUT-3 | Glucose | Neurons | High affinity - neurons always get glucose |
| GLUT-4 | Glucose | Muscle, adipose tissue | INSULIN-REGULATED - the most clinically important |
| GLUT-5 | Fructose | Small intestine, sperm | Does not transport glucose |
GLUT-4 and Insulin (most exam-tested concept):
Normal state: GLUT-4 stored in intracellular vesicles (not on membrane)
↓
Insulin binds insulin receptor
↓
Tyrosine kinase activation → signal cascade
↓
GLUT-4 vesicles fuse with plasma membrane
↓
GLUT-4 appears on cell surface
↓
Glucose enters cell rapidly (facilitated diffusion DOWN concentration gradient)
In Type 2 Diabetes: Insulin resistance means GLUT-4 does not translocate properly → glucose stays in blood → hyperglycemia.
Characteristics of Facilitated Diffusion:
- Saturability: Has a maximum rate (Vmax) - unlike simple diffusion, which has no ceiling. When all carriers are occupied, adding more solute does not increase transport rate.
- Specificity: Each carrier is specific for one or a few closely related molecules
- Competitive inhibition: A similar molecule can compete for the carrier
- Bidirectional: Can move in either direction, always down concentration gradient
C. OSMOSIS
What is it?
The net diffusion of water across a selectively permeable membrane from the side of lower solute concentration (higher water concentration) to the side of higher solute concentration (lower water concentration).
Simply: Water moves to wherever the particles are more concentrated - it moves toward the more concentrated solution.
The Osmosis Story (Simple Explanation First):
Imagine you have a U-tube with a membrane in the middle that allows water through but not salt:
- Left side: pure water
- Right side: saltwater
Water moves from left (pure water) to right (saltwater) by osmosis, trying to dilute the salt. The water level on the right rises. The pressure created by the rising water column = osmotic pressure.
Osmotic Pressure Calculation (Van't Hoff Equation):
π = nCRT
Where:
- π = osmotic pressure
- n = number of particles the solute dissociates into (e.g., NaCl → Na+ + Cl- → n=2)
- C = molar concentration
- R = gas constant
- T = absolute temperature (Kelvin)
Clinical values:
- Normal plasma osmolality = 285-295 mOsm/kg H₂O
- Intracellular osmolality = approximately equal (cells are in osmotic equilibrium with ECF)
- Formula: Plasma Osm ≈ 2[Na+] + Glucose/18 + BUN/2.8
Tonicity vs. Osmolality:
| Term | Definition | What it affects |
|---|
| Osmolality | Total solute particles per kg water | Measured in lab |
| Tonicity | Effective osmolality - only particles that can't cross membrane | Determines cell volume |
- Isotonic solution (0.9% NaCl / Normal Saline): No net water movement → cell size unchanged
- Hypotonic solution (pure water / 0.45% NaCl): Water enters cell → cell swells → may lyse (hemolysis of RBCs)
- Hypertonic solution (3% NaCl / 50% glucose): Water leaves cell → cell shrinks (crenation)
Clinical application - IV fluids:
- 0.9% NaCl (Normal Saline) = isotonic - safe for most situations
- 0.45% NaCl (Half Normal Saline) = hypotonic - causes cells to swell
- 3% NaCl (Hypertonic saline) = hypertonic - used in severe hyponatremia to pull water from brain cells (to reduce cerebral edema)
- 5% Dextrose in water: Initially isotonic, but glucose is metabolized quickly → effectively hypotonic in body → causes cells to swell (not good for brain edema patients!)
D. ACTIVE TRANSPORT
Why is it needed?
Some substances must be moved against their concentration gradient. The cell "wants" to keep Na+ low inside and K+ high inside, even though Na+ naturally wants to flow in (high outside) and K+ naturally wants to flow out (high inside). Moving them against their gradient requires energy (ATP).
PRIMARY ACTIVE TRANSPORT: The Na+/K+ ATPase Pump
This is the most important pump in human physiology. It consumes 20-40% of all ATP produced in many cells.
The pump transports:
- 3 Na+ OUT of the cell (against Na+ concentration gradient)
- 2 K+ IN to the cell (against K+ concentration gradient)
- Uses 1 ATP per cycle
Step-by-step mechanism:
Step 1: 3 Na+ bind to the inner face of the pump
↓
Step 2: ATP binds to the pump → ATP is hydrolyzed → Pi is transferred to pump (phosphorylation)
↓
Step 3: Phosphorylation causes conformational change → pump opens to OUTSIDE
↓
Step 4: 3 Na+ are released outside the cell
↓
Step 5: 2 K+ bind from outside
↓
Step 6: Dephosphorylation (Pi released) → pump returns to original shape → opens to INSIDE
↓
Step 7: 2 K+ are released inside the cell
↓
Cycle repeats
Net result of Na+/K+ ATPase activity:
- Low Na+ inside the cell (14 mEq/L ICF vs 142 mEq/L ECF)
- High K+ inside the cell (140 mEq/L ICF vs 4 mEq/L ECF)
- Net negative charge inside the cell (because 3+ out, 2+ in = net 1+ out per cycle) → Resting membrane potential approximately -70 mV inside
- Osmotic stability - prevents cell swelling
What regulates Na+/K+ ATPase:
- Increased by: High intracellular Na+, thyroid hormones (upregulate pump), aldosterone (increases pump in kidney)
- Decreased by: Digoxin/digitalis (specifically inhibits the pump), ouabain, low ATP (hypoxia), hypothyroidism
THE DIGOXIN STORY (Classic Clinical Application):
Digoxin blocks Na+/K+ ATPase pump
↓
Na+ accumulates inside cardiac cell
↓
Na+/Ca²+ exchanger (NCX) can no longer expel Ca²+
(NCX normally exports Ca²+ in exchange for Na+ entering)
↓
Ca²+ accumulates inside cardiac cell
↓
More Ca²+ available for myosin-actin interaction
↓
Stronger cardiac contraction (positive inotropic effect)
↓
Used in heart failure and atrial fibrillation
Side effects of digoxin toxicity:
- Nausea, vomiting (GI - gut cells also have Na+/K+ ATPase)
- Visual disturbances (yellow-green halos - photoreceptors affected)
- Arrhythmias (cardiac cells - enhanced automaticity)
- Hypokalemia WORSENS digoxin toxicity (low K+ outside competes less with digoxin for pump)
OTHER PRIMARY ACTIVE TRANSPORT PUMPS:
| Pump | Location | Function | Drug that acts on it |
|---|
| Ca²+ ATPase (SERCA) | SR/ER membrane | Pumps Ca²+ into SR for muscle relaxation | -- |
| Ca²+ ATPase (PMCA) | Plasma membrane | Pumps Ca²+ out of cell | -- |
| H+/K+ ATPase | Gastric parietal cells | Secretes H+ into stomach (acid production) | Proton pump inhibitors (omeprazole, pantoprazole) |
| H+ ATPase | Renal collecting duct | Acid secretion | Defect → Distal Renal Tubular Acidosis (Type 1) |
SECONDARY ACTIVE TRANSPORT
The concept: The Na+/K+ ATPase pump creates a steep Na+ gradient (low Na+ inside the cell). This gradient represents stored energy. Secondary active transport "spends" this stored Na+ gradient to move other substances against their gradients - without directly using ATP (it indirectly uses ATP, because ATP was used to build the Na+ gradient).
Two types:
1. Co-transport (Symport) - substances move SAME direction as Na+:
| Transporter | What it transports | Location | Clinical relevance |
|---|
| SGLT-1 | Na+ + Glucose | Small intestine | Glucose absorption |
| SGLT-2 | Na+ + Glucose | Proximal renal tubule | Reabsorbs 90% of filtered glucose |
| NKCC2 | Na+/K+/2Cl- | Loop of Henle (thick ascending) | Target of furosemide (loop diuretics) |
| NCC | Na+/Cl- | Distal convoluted tubule | Target of thiazide diuretics |
SGLT-2 Inhibitors (Gliflozins) - The New Diabetic Revolution:
SGLT-2 normally reabsorbs glucose from glomerular filtrate
↓
Empagliflozin/Dapagliflozin/Canagliflozin block SGLT-2
↓
Glucose stays in urine (glucosuria) → blood glucose falls
↓
Osmotic diuresis → weight loss, blood pressure reduction
↓
Also reduces preload/afterload on heart → cardiovascular protection
2. Counter-transport (Antiport) - substances move OPPOSITE direction to Na+:
| Transporter | What it transports | Location | Clinical relevance |
|---|
| Na+/Ca²+ exchanger (NCX) | Na+ IN, Ca²+ OUT | Heart, neurons | 3 Na+ in, 1 Ca²+ out |
| Na+/H+ exchanger (NHE) | Na+ IN, H+ OUT | Kidney, gut | Acid-base regulation |
| Na+/K+/2Cl- (NKCC1) | Na+/K+/2Cl- IN | Multiple tissues | Cell volume regulation |
━━━━━━━━━━━━━━━━━━━━
STAGE 4: MOLECULAR & CELLULAR PHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
The Resting Membrane Potential
Every living cell has an electrical potential difference across its membrane. In a typical nerve cell: -70 mV inside relative to outside.
Why -70 mV? (The Complete Explanation)
Step 1 - Unequal ion distribution (created by Na+/K+ ATPase):
| Ion | Inside (ICF) | Outside (ECF) | Equilibrium Potential |
|---|
| K+ | 140 mEq/L | 4 mEq/L | -94 mV |
| Na+ | 14 mEq/L | 142 mEq/L | +61 mV |
| Cl- | 4 mEq/L | 103 mEq/L | -86 mV |
| Ca²+ | 0.0001 mEq/L | 2.4 mEq/L | +132 mV |
| Large anions (A-) | High | Low | Cannot cross membrane |
Step 2 - Selective permeability at rest:
At rest, the membrane is much more permeable to K+ than to Na+ (K+ leaks channels are always open). K+ tends to diffuse OUT (down concentration gradient), carrying positive charge out.
Step 3 - Equilibrium:
As K+ leaves, the inside becomes more negative. Eventually the electrical attraction (inside is negative, pulls K+ back) balances the concentration gradient (pushing K+ out). The voltage at which these forces balance = Nernst Equilibrium Potential for K+ = -94 mV.
But the actual resting membrane potential is only -70 mV (not -94 mV) because a small amount of Na+ leaks in, partly depolarizing the membrane.
The Goldman-Hodgkin-Katz (GHK) equation accounts for multiple ions:
Vm = (RT/F) × ln [PK(Ko) + PNa(Nao) + PCl(Cli)]
[PK(Ki) + PNa(Nai) + PCl(Clo)]
Where P = permeability of each ion. At rest, PK >> PNa, so K+ dominates and pushes potential toward -94 mV.
Signal Transduction Pathways (Receptor-to-Response)
Understanding how cells respond to signals is fundamental.
Type 1: G-Protein Coupled Receptors (GPCRs)
Ligand (hormone/neurotransmitter) binds to GPCR
↓
GPCR activates G-protein (Gs, Gi, Gq)
↓
Gs → activates adenylyl cyclase → ↑ cAMP → activates PKA
Gi → inhibits adenylyl cyclase → ↓ cAMP
Gq → activates phospholipase C → IP3 + DAG
IP3 → releases Ca²+ from ER
DAG → activates PKC
cAMP pathway examples:
- β-adrenergic receptor (Gs) → ↑cAMP → PKA → phosphorylates proteins → ↑heart rate, ↑contractility, bronchodilation
- Glucagon receptor (Gs) → ↑cAMP → gluconeogenesis, glycogenolysis
- TSH receptor (Gs) → ↑cAMP → thyroid hormone synthesis
- Muscarinic M2 receptor (Gi) → ↓cAMP → ↓heart rate
IP3/DAG pathway examples:
- α1-adrenergic (Gq) → IP3 → Ca²+ release → vasoconstriction
- Angiotensin II (AT1 receptor, Gq) → vasoconstriction
- Oxytocin → uterine contraction
Type 2: Receptor Tyrosine Kinases (RTKs)
Insulin / IGF-1 / EGF / PDGF binds receptor
↓
Receptor dimerizes → autophosphorylation (tyrosine residues)
↓
Activates IRS-1 (insulin receptor substrate)
↓
PI3K → PIP3 → Akt (PKB) activation
↓
GLUT-4 translocation → glucose uptake
↓
Glycogen synthesis, protein synthesis, cell growth
Type 3: Nuclear Receptors (for lipid-soluble hormones)
Steroid hormone / Thyroid hormone / Vitamin D / Retinoic acid enters cell (lipid soluble)
↓
Binds to cytoplasmic or nuclear receptor
↓
Hormone-receptor complex enters nucleus
↓
Binds to hormone response element (HRE) on DNA
↓
Increases or decreases gene transcription
↓
Changes protein synthesis → slower, longer-lasting response (hours to days)
Contrast with membrane receptors: Effect in minutes vs. nuclear receptors (hours to days)
━━━━━━━━━━━━━━━━━━━━
STAGE 5: INTEGRATED PHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
Cell Physiology Connects Every System
| System | Connection to Cell Physiology |
|---|
| Nervous system | Action potential = Na+ influx then K+ efflux through voltage-gated channels; synaptic transmission via ligand-gated channels |
| Cardiac | Pacemaker potential = funny (HCN) channels; action potential = Na+, Ca²+, K+ channels; contraction = Ca²+ signaling |
| Renal | All tubular transport = transporters studied here (SGLT-2, NHE, NKCC2, NCC, AQP2) |
| Endocrine | All hormone action = receptor signaling (GPCRs, RTKs, nuclear receptors) |
| GI | Glucose/amino acid absorption = SGLT-1 (co-transport); iron absorption = active transport; B12 = receptor-mediated endocytosis |
| Respiratory | O₂/CO₂ exchange = simple diffusion across alveolar-capillary membrane; CO₂ enters RBC → converted to HCO₃- by carbonic anhydrase (cellular reaction) |
| Immune | Phagocytosis, endocytosis; cytokine receptor signaling; lymphocyte activation |
━━━━━━━━━━━━━━━━━━━━
STAGE 6: APPLIED PHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
Exercise Physiology
- Muscle cells increase Na+/K+ ATPase activity
- ATP demand increases 10-100 fold → mitochondria work harder → oxygen demand increases
- GLUT-4 translocation occurs even WITHOUT insulin during exercise (muscle contraction activates AMPK → GLUT-4 to membrane) - why exercise helps diabetes
- K+ exits working muscle cells → slight hyperkalemia during vigorous exercise → vasodilation of muscle vessels
High Altitude
- Lower O₂ partial pressure → less O₂ diffuses into blood (Fick's Law - reduced concentration gradient)
- Cells experience hypoxia → switch to anaerobic glycolysis → lactic acid accumulates
- Adaptive: ↑erythropoietin (EPO) from renal interstitial cells → more RBCs → more O₂ carriers
- HIF-1α (Hypoxia Inducible Factor) activated in cells → upregulates genes for EPO, VEGF, glycolysis enzymes
Aging
- Mitochondrial function declines (mtDNA mutations accumulate)
- Na+/K+ ATPase activity decreases
- Cell membrane becomes less fluid (cholesterol: phospholipid ratio changes)
- Accumulation of oxidative damage to proteins, membranes, and DNA
Pregnancy
- Placental cells have high Na+/K+ ATPase and amino acid transporters
- Maternal cells downregulate GLUT-4 sensitivity (insulin resistance) → nutrients available for fetus
- Syncytiotrophoblast has multiple transport systems for glucose, amino acids, fatty acids
Stress Response
- Cortisol enters cells → nuclear receptor → upregulates gluconeogenic enzymes → provides glucose
- Catecholamines → β-receptors → ↑cAMP → glycogenolysis in muscle/liver cells
- Na+/K+ ATPase activity increases during stress → cell volume maintained
━━━━━━━━━━━━━━━━━━━━
STAGE 7: CLINICAL PHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
What Happens When Cell Membrane Transport Fails?
| Condition | Mechanism | Manifestation |
|---|
| Hyponatremia | ECF becomes hypotonic → water enters cells → cells swell | Brain cells swell → headache, confusion, seizures, coma |
| Hypernatremia | ECF becomes hypertonic → water exits cells → cells shrink | Brain cells shrink → neurological symptoms |
| Hypokalemia | Low ECF K+ → more K+ leaks out → hyperpolarization of membrane | Muscle weakness, cramps, arrhythmias |
| Hyperkalemia | High ECF K+ → less K+ leaks out → depolarization → persistent Na+ channel inactivation | Muscle weakness, dangerous cardiac arrhythmias (peaked T waves, wide QRS, sine wave pattern, VF) |
| Digoxin toxicity | Na+/K+ ATPase blocked | Nausea, arrhythmias, visual changes |
| Cholera | Cholera toxin ADP-ribosylates Gs → permanently activates adenylyl cyclase → ↑↑cAMP in enterocytes → Cl- secretion into gut | Massive "rice-water" diarrhea (10-20 L/day), severe dehydration, death |
| Cystic Fibrosis | CFTR Cl- channel mutation → Cl- cannot exit cells → water follows → thick, dry mucus | Chronic lung infections, pancreatic insufficiency, male infertility |
| Nephrogenic DI | AQP2 or V2 receptor defect → ADH cannot insert aquaporins into collecting duct → cannot concentrate urine | Polyuria, polydipsia, dilute urine despite high serum osmolality |
Important Bedside Findings
- Hyponatremia: Check for signs of cerebral edema - papilledema, seizures
- Hyperkalemia on ECG: Peaked T waves → prolonged PR → wide QRS → sine wave → VF (memorize this sequence!)
- Cholera patient: Sunken eyes, skin tenting, absent pulse, "washerwoman's hands" - all signs of profound dehydration
━━━━━━━━━━━━━━━━━━━━
STAGE 8: PATHOPHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
Classic Pathophysiology Chain - Cholera
Vibrio cholerae ingested
↓
Colonizes small intestine
↓
Secretes cholera toxin
↓
Toxin A subunit ADP-ribosylates Gs alpha subunit
↓
Gs alpha PERMANENTLY ACTIVATED (cannot hydrolyze GTP to GDP)
↓
Adenylyl cyclase permanently active → ↑↑↑ cAMP in enterocytes
↓
PKA activates CFTR Cl- channel → massive Cl- efflux into intestinal lumen
↓
Na+ follows Cl- (electrochemical gradient) → water follows by osmosis
↓
Profuse watery diarrhea (10-20 L/day)
↓
Hypovolemia, hypokalemia, metabolic acidosis
↓
Cardiac arrest from electrolyte abnormalities if untreated
Classic Pathophysiology Chain - Cystic Fibrosis
CFTR gene mutation (most common: ΔF508 - deletion of phenylalanine 508)
↓
CFTR protein misfolded → degraded by ubiquitin-proteasome system
↓
No functional Cl- channel on apical membrane of epithelial cells
↓
Cl- trapped inside cells
↓
Na+ channel (ENaC) hyperactive → excess Na+ absorbed
↓
Water follows Na+ → airway surface liquid depleted → mucus becomes thick
↓
Ciliary beating impaired → mucus clearance fails
↓
Bacterial colonization (Pseudomonas aeruginosa, Staphylococcus aureus)
↓
Chronic infection → neutrophilic inflammation → bronchiectasis → respiratory failure
Plus: Pancreatic duct obstruction → pancreatic insufficiency → malabsorption
Vas deferens obstruction → obstructive azoospermia → male infertility (98% of CF males)
Classic Pathophysiology Chain - Hyponatremia/Cerebral Edema
Serum Na+ falls rapidly (e.g., SIADH, excessive water intake)
↓
ECF becomes hypotonic relative to ICF
↓
Water moves INTO brain cells by osmosis (water moves to area of higher solute concentration)
↓
Brain cells swell
↓
Brain is enclosed in rigid skull → increased intracranial pressure
↓
Headache → confusion → seizures → herniation → death
Management principle: Correct slowly (not more than 8-10 mEq/L per 24 hours) or rapid correction causes central pontine myelinolysis (osmotic demyelination syndrome) - myelin sheaths collapse when brain cells shrink too fast.
━━━━━━━━━━━━━━━━━━━━
STAGE 9: PHARMACOLOGICAL CORRELATIONS
━━━━━━━━━━━━━━━━━━━━
Drugs Acting on Cell Membrane Transport
| Drug | Target | Mechanism | Clinical Use |
|---|
| Digoxin | Na+/K+ ATPase | Blocks pump → ↑intracellular Na+ → ↑Ca²+ via NCX | Heart failure, Atrial fibrillation |
| Furosemide | NKCC2 (Na+/K+/2Cl- co-transporter) | Blocks co-transport in thick ascending loop | Loop diuretic - HTN, HF, edema |
| Thiazides | NCC (Na+/Cl- co-transporter) | Blocks Na+/Cl- co-transport in DCT | HTN, thiazide-sensitive hyponatremia |
| Amiloride | ENaC (Na+ channel) | Blocks epithelial Na+ channel in collecting duct | K+-sparing diuretic, CF (experimental) |
| SGLT-2 inhibitors | SGLT-2 co-transporter | Blocks Na+/glucose co-transport in PCT → glucosuria | Type 2 DM, Heart failure, CKD |
| Omeprazole/Pantoprazole | H+/K+ ATPase (proton pump) | Irreversibly blocks pump → no acid secretion | GERD, PUD, H. pylori |
| Local anesthetics (Lidocaine) | Voltage-gated Na+ channels | Block Na+ influx → no action potential | Local anesthesia, Ventricular arrhythmias |
| Ivermectin | Cl- channels | Opens Cl- channels in parasites → hyperpolarization → paralysis | Onchocerciasis, strongyloidiasis |
| Lumacaftor/Ivacaftor | CFTR channel | Corrects CFTR protein folding and gating | Cystic fibrosis |
| Colchicine | Microtubules | Binds tubulin → prevents polymerization → stops neutrophil migration | Acute gout, FMF |
| Vincristine | Microtubules | Binds tubulin → stops mitotic spindle formation → cell death | Cancer chemotherapy |
━━━━━━━━━━━━━━━━━━━━
STAGE 10: IMPORTANT GRAPHS
━━━━━━━━━━━━━━━━━━━━
Graph 1: Simple vs. Facilitated Diffusion
Rate of | Facilitated diffusion
Transport | _____________________________ (Vmax plateau)
| /
| /
| / Simple diffusion
| / /
| / /
| / /
|__/__________/__________________
Concentration
Key points:
- Simple diffusion: Linear - no maximum rate, increases proportionally with concentration
- Facilitated diffusion: Hyperbolic - saturates at Vmax when all carriers are occupied
- Km = concentration at which transport is at 50% Vmax (measure of carrier affinity)
- High Km = low affinity (needs high concentration to half-saturate); Low Km = high affinity
- GLUT-2 has HIGH Km (low affinity for glucose) → acts as glucose sensor in pancreatic β-cells (only activates at high glucose)
- GLUT-3 has LOW Km (high affinity) → neurons always get glucose even when blood glucose is low
Graph 2: Osmosis Curve (Volume vs. Osmolality)
Cell Volume |
|
| Normal -----------
Swollen | \ ^isotonic
| \
| \_______________
Shrunken |
|___________________
Hypo Normal Hyper
tonic tonic
(Osmolality)
Graph 3: Resting Membrane Potential - Effect of ECF [K+]
Membrane |
Potential |
(mV) |
0 ---------|------------------------------------------
| Normal ECF K+
-70 --------|--------X (resting potential)
| /
| / (hypokalemia → hyperpolarization)
-94 --------|-----X (K+ equilibrium potential)
|
| ↑ Hyperkalemia → depolarization (toward 0)
|
|__________________________________________
ECF [K+] concentration
Clinical:
- Hypokalemia → K+ exits cell more freely → membrane hyperpolarizes (more negative) → cell harder to excite → muscle weakness
- Hyperkalemia → less K+ exits → membrane depolarizes (less negative) → cell initially more excitable, then Na+ channels inactivate → muscle paralysis + arrhythmias
━━━━━━━━━━━━━━━━━━━━
STAGE 11: IMPORTANT TABLES
━━━━━━━━━━━━━━━━━━━━
Table 1: Intracellular vs. Extracellular Fluid Composition
| Ion/Substance | ICF (mEq/L) | ECF (mEq/L) | Gradient Maintained by |
|---|
| Na+ | 14 | 142 | Na+/K+ ATPase (pumps Na+ OUT) |
| K+ | 140 | 4 | Na+/K+ ATPase (pumps K+ IN) |
| Ca²+ | 0.0001 | 2.4 | Ca²+ ATPase + Na+/Ca²+ exchanger |
| Cl- | 4 | 103 | Follows Na+ gradients, passive |
| HCO₃- | 10 | 24 | Na+/HCO₃- co-transporters |
| Mg²+ | 58 | 1.2 | Active transport |
| Phosphate | 140 | 4 | Active transport |
Table 2: Types of Membrane Transport - Complete Comparison
| Feature | Simple Diffusion | Facilitated Diffusion | Primary Active Transport | Secondary Active Transport |
|---|
| Energy required | No | No | Yes (ATP directly) | No (ATP indirectly) |
| Direction | Down gradient | Down gradient | Against gradient | Against gradient for secondary solute |
| Carrier protein | No | Yes | Yes | Yes |
| Saturation (Vmax) | No | Yes | Yes | Yes |
| Specificity | Low | High | High | High |
| Examples | O₂, CO₂, steroids | Glucose (GLUT), urea | Na+/K+ pump, H+/K+ pump | SGLT-1, NKCC2, NHE |
Table 3: GLUT Transporters - High Yield
| GLUT | Km for glucose | Location | Regulation | Significance |
|---|
| GLUT-1 | Low (1 mM) | RBCs, brain endothelium, placenta | Constitutive | Always on - basal glucose |
| GLUT-2 | High (15-20 mM) | Liver, β-cells, kidney, gut | Constitutive | Glucose sensor |
| GLUT-3 | Very low (0.1 mM) | Neurons, placenta | Constitutive | Neurons get glucose first |
| GLUT-4 | Moderate (5 mM) | Muscle, adipose | Insulin-dependent | Insulin-stimulated |
| GLUT-5 | High (fructose) | Small intestine, sperm | Constitutive | Fructose absorption |
Table 4: Key Clinical Disorders of Cell Transport
| Disease | Defective Protein | What accumulates/fails | Key Features |
|---|
| Cystic Fibrosis | CFTR (Cl- channel) | Thick mucus, Cl- transport failure | Lung disease, pancreatic insufficiency, infertility |
| Diabetes Type 2 | GLUT-4 signaling | Glucose in blood | Hyperglycemia, complications |
| Gaucher's Disease | Glucocerebrosidase (lysosomal) | Glucocerebroside | Hepatosplenomegaly, bone pain |
| Nephrogenic DI | AQP2 or V2 receptor | Cannot concentrate urine | Polyuria, polydipsia |
| Barter Syndrome | NKCC2 (ROMK, ClC-Kb) | Na+, K+, Cl- wasting | Like furosemide being permanently on |
| Gitelman Syndrome | NCC (DCT Na+/Cl-) | Na+, Mg2+ wasting | Like thiazide being permanently on |
━━━━━━━━━━━━━━━━━━━━
STAGE 12: NUMERICAL VALUES - HIGH YIELD
━━━━━━━━━━━━━━━━━━━━
| Parameter | Normal Value | Unit | Clinical Significance |
|---|
| Cell membrane thickness | 7.5-10 | nm | -- |
| Total body cells | ~35-40 trillion | cells | -- |
| Water content of cell | 70-85 | % | Fat cells have less water |
| ICF volume | 28 | L (in 70 kg man) | 40% body weight |
| ECF volume | 14 | L | 20% body weight |
| Plasma volume | 3 | L | Part of ECF |
| ICF Na+ | 14 | mEq/L | Low (pump keeps Na+ out) |
| ECF Na+ | 142 | mEq/L | High |
| ICF K+ | 140 | mEq/L | High (pump keeps K+ in) |
| ECF K+ | 4 | mEq/L | Low (normal: 3.5-5.0) |
| ICF Ca²+ | 0.0001 | mEq/L | Extremely low (~100 nM) |
| ECF Ca²+ | 2.4 | mEq/L | High |
| Resting membrane potential (nerve) | -70 | mV | Inside negative |
| K+ equilibrium potential | -94 | mV | Nernst equation |
| Na+ equilibrium potential | +61 | mV | Nernst equation |
| Plasma osmolality | 285-295 | mOsm/kg | Maintained by ADH |
| Na+/K+ ATPase stoichiometry | 3 Na+ out, 2 K+ in | ions/ATP | Net -1 charge out per cycle |
| ATP used by Na+/K+ ATPase | 20-40 | % of total cell ATP | Enormous energy cost |
| Ribosome size (eukaryote) | 80 S (60S + 40S) | Svedberg units | Differs from 70S prokaryote |
| Lysosomal pH | ~5 | pH units | Acid hydrolases work here |
━━━━━━━━━━━━━━━━━━━━
STAGE 13: VIVA PREPARATION
━━━━━━━━━━━━━━━━━━━━
Short Viva Questions
-
Q: What is the composition of the cell membrane?
A: 55% proteins, 25% phospholipids, 13% cholesterol, 4% other lipids, 3% carbohydrates.
-
Q: How many Na+ and K+ does the Na+/K+ ATPase pump transport per ATP?
A: 3 Na+ OUT, 2 K+ IN per 1 ATP.
-
Q: What is the resting membrane potential of a nerve cell?
A: Approximately -70 mV (inside negative relative to outside).
-
Q: What is the difference between simple and facilitated diffusion?
A: Both move substances DOWN their concentration gradient without ATP. Simple diffusion needs no protein; facilitated diffusion requires a carrier protein and shows saturation kinetics.
-
Q: What is secondary active transport?
A: Transport of a substance against its gradient, using the energy of the Na+ electrochemical gradient (which was built by the Na+/K+ ATPase using ATP). Indirectly uses ATP.
-
Q: Name the enzyme inside lysosomes and its optimal pH.
A: Acid hydrolases (various). Optimal pH ~5.
-
Q: Which organelle synthesizes steroids?
A: Smooth endoplasmic reticulum.
-
Q: What is GLUT-4's unique feature?
A: It is insulin-dependent - translocates to the cell surface only when insulin stimulates it. Present in muscle and adipose tissue.
-
Q: Why does digoxin increase cardiac contractility?
A: Digoxin inhibits Na+/K+ ATPase → intracellular Na+ rises → Na+/Ca²+ exchanger cannot expel Ca²+ → intracellular Ca²+ rises → stronger contraction.
-
Q: What is Fick's law of diffusion?
A: Rate of diffusion is proportional to (concentration gradient × area × lipid solubility) divided by (membrane thickness × molecular size).
Long Viva Questions
-
Describe the structure of the cell membrane and explain the fluid mosaic model. How does the composition of the membrane relate to its function as a selective barrier?
-
Explain the mechanism of the Na+/K+ ATPase pump, its regulation, and its clinical significance. How does digoxin exploit this mechanism?
-
Compare and contrast primary and secondary active transport. Give clinical examples of drugs that act on secondary active transporters.
-
Explain the concept of resting membrane potential. What ions are involved? How is it maintained? What are the clinical consequences of altering it?
-
Describe the GLUT transporter family. Why does GLUT-2 have high Km while GLUT-3 has low Km, and what is the physiological rationale?
Examiner's Favorite Trap Questions
Q: "Osmosis is not diffusion" - TRUE or FALSE?
A: FALSE. Osmosis IS a form of diffusion - specifically the diffusion of WATER across a selectively permeable membrane. A very common trap.
Q: Which cell has no mitochondria?
A: Mature red blood cells. They have no nucleus OR mitochondria. They rely entirely on anaerobic glycolysis (Embden-Meyerhof pathway) for ATP.
Q: Is the Na+/K+ ATPase electrogenic?
A: YES. It pumps 3 Na+ out for every 2 K+ in = net 1 positive charge exits per cycle = contributes to the negative resting membrane potential (electrogenic pump).
━━━━━━━━━━━━━━━━━━━━
STAGE 14: EXAM PREPARATION - HIGH YIELD
━━━━━━━━━━━━━━━━━━━━
MBBS Important Points
- Cell membrane = fluid mosaic model (Singer-Nicholson, 1972)
- Phospholipid bilayer = hydrophilic heads face water, hydrophobic tails face each other
- Cholesterol = fluidity regulator
- Integral proteins = penetrate membrane; peripheral proteins = on surface
- Simple diffusion = no protein, no energy, linear, no saturation
- Facilitated diffusion = carrier protein, no energy, saturates at Vmax
- Active transport = energy (ATP), against gradient
- Na+/K+ ATPase = 3 Na+ out, 2 K+ in, 1 ATP consumed
- Secondary active transport = co-transport (symport) or counter-transport (antiport)
- Osmolality = 285-295 mOsm/kg; formula = 2[Na+] + Glucose/18 + BUN/2.8
PG Entrance High-Yield Concepts
| Concept | Answer |
|---|
| Drug inhibiting Na+/K+ ATPase | Digoxin, Ouabain |
| Drug blocking H+/K+ ATPase | Omeprazole (PPI) |
| Drug blocking NKCC2 | Furosemide |
| Drug blocking NCC | Thiazides |
| Drug blocking ENaC | Amiloride, Triamterene |
| SGLT-2 inhibitor example | Empagliflozin, Dapagliflozin |
| Transporter defect in CF | CFTR (Cl- channel) |
| Lysosomal storage disease with glucocerebrosidase deficiency | Gaucher's disease |
| Water channel protein | Aquaporin (AQP) |
| Nobel Prize for aquaporin discovery | Peter Agre, 2003 |
| Most abundant organelle | Ribosome |
| Organelle with its own DNA | Mitochondria (also chloroplasts in plants) |
| Maternal inheritance | Mitochondrial DNA |
| Ribosome size in eukaryotes | 80S (60S + 40S) |
| Ribosome size in prokaryotes | 70S (50S + 30S) |
━━━━━━━━━━━━━━━━━━━━
STAGE 15: MEMORY TOOLS
━━━━━━━━━━━━━━━━━━━━
Mnemonics
Na+/K+ ATPase: "THREE's OUT, TWO's IN"
- 3 Na+ go OUT (like 3-letter word "out")
- 2 K+ come IN (like 2-letter word "in")
Organelles without membranes: "CRS"
- Centrosome/Centrioles
- Ribosomes
- Cytoskeleton
Lysosomal storage diseases: "Gauche Tay Has Niemann-Pick's Fabry"
- Gaucher's (glucocerebrosidase)
- Tay-Sachs (hex A)
- Hurler's (α-L-iduronidase)
- Niemann-Pick (sphingomyelinase)
- Fabry (α-galactosidase A)
GLUT transporters: "1-Brain, 2-Liver, 3-Neuron, 4-Muscle, 5-Fructose"
(Think: 1=everywhere basal, 2=β-cell sensor, 3=neuron preferential, 4=insulin-dependent, 5=fructose only)
Membrane composition: "55-25-13-4-3" = "Five-Five-Twenty-Five-Thirteen-Four-Three"
- 55% protein, 25% phospholipid, 13% cholesterol, 4% lipids, 3% carbs
Analogies
Na+/K+ ATPase = Security Guard at a Nightclub:
- The guard (pump) throws out 3 troublemakers (Na+) for every 2 VIPs (K+) let in
- Uses energy (salary/ATP) to do this job
- If you bribe the guard (digoxin), chaos ensues (Na+ builds up, then Ca²+)
Osmosis = Tea Bag in Hot Water:
- The tea (solute) can't cross, but water can
- Water moves INTO the tea bag to dilute the tea
- The tea bag swells - exactly what happens to cells in hypotonic solution
Facilitated Diffusion = Revolving Door:
- The door (carrier protein) helps you through but you must walk yourself (no motor pushing you)
- Only works if there's more people outside wanting in, than inside wanting out (concentration gradient)
- If too many people try to use one door, it gets saturated (Vmax)
Cell = City Analogy:
| City Component | Cell Equivalent |
|---|
| City wall | Cell membrane |
| Power plant | Mitochondria |
| Library/Archives | Nucleus (DNA) |
| Post office | Golgi apparatus |
| Assembly line | Ribosomes + RER |
| Waste management | Lysosomes |
| Roads/Transport network | Cytoskeleton |
| Chemical factory | Smooth ER |
━━━━━━━━━━━━━━━━━━━━
STAGE 16: FLOWCHARTS & MIND MAPS
━━━━━━━━━━━━━━━━━━━━
Master Flowchart: Membrane Transport Decision Tree
SUBSTANCE NEEDS TO CROSS CELL MEMBRANE
↓
Is it LIPID-SOLUBLE?
/ \
YES NO
↓ ↓
Simple Diffusion Is there a CONCENTRATION GRADIENT?
(O₂, CO₂, (high outside → low inside OR
steroids, high inside → low outside)
fat-soluble / \
vitamins) YES NO (going against gradient)
↓ ↓
Does it use a PROTEIN? ACTIVE TRANSPORT
/ \ / \
NO YES Uses ATP Uses Na+ gradient
↓ ↓ directly (built by ATP)
Simple Facilitated ↓ ↓
Diffusion Diffusion PRIMARY SECONDARY
(through (GLUT ACTIVE ACTIVE TRANSPORT
channels) transporters) TRANSPORT (co-transport/
(Na+/K+ pump, counter-transport)
Ca²+ pump,
H+/K+ pump)
Mind Map: Na+/K+ ATPase
NA+/K+ ATPASE PUMP
|
┌───────────────┼───────────────┐
↓ ↓ ↓
FUNCTION REGULATION CLINICAL
3 Na+ OUT ↑ by: SIGNIFICANCE
2 K+ IN - High ICF Na+ ↓
1 ATP used - Aldosterone Resting membrane
- T3/T4 potential
↓ ↓ by: ↓
CREATES: - Digoxin Osmotic stability
Low ICF Na+ - Ouabain ↓
High ICF K+ - Hypoxia Secondary active
Negative RMP - Hypothyroid transport driving
force
━━━━━━━━━━━━━━━━━━━━
STAGE 17: COMMON MISTAKES & EXAM TRAPS
━━━━━━━━━━━━━━━━━━━━
| Common Mistake | Correct Understanding |
|---|
| "Osmosis is not diffusion" | WRONG. Osmosis IS diffusion of water |
| "Active transport always needs ATP directly" | WRONG. Secondary active transport is indirect - uses Na+ gradient |
| "Facilitated diffusion requires energy" | WRONG. No energy needed - just carrier protein |
| "All cells have mitochondria" | WRONG. Mature RBCs and platelets have NO mitochondria |
| "Cell membrane is mostly protein" | CORRECT but tricky - 55% protein, 25% phospholipid (protein > lipid) |
| "GLUT-4 is always on the cell surface" | WRONG. GLUT-4 is intracellular at rest; only moves to surface with insulin (or exercise) |
| "Digoxin has positive inotropic effect because it increases Ca²+ channel opening" | WRONG. It works via Na+/K+ ATPase inhibition → Na+ accumulation → NCX reversal → Ca²+ accumulation |
| "Hypertonic saline is bad in hyponatremia" | PARTIALLY WRONG. Hypertonic saline (3%) IS used in severe/symptomatic hyponatremia, but must be given SLOWLY |
| "Isotonic means the same osmolality as plasma" | Partially incomplete - tonicity (effective osmolality) is what matters for cell volume, not total osmolality |
| "Ribosomes are organelles" | Technically debatable - ribosomes have no membrane and occur free in cytoplasm too. Many textbooks call them organelles; strictly speaking they are ribonucleoprotein particles |
━━━━━━━━━━━━━━━━━━━━
STAGE 18: RAPID REVISION
━━━━━━━━━━━━━━━━━━━━
20 Key Takeaways
- Cell membrane = lipid bilayer (55% protein, 25% phospholipid, 13% cholesterol)
- Phospholipids are amphipathic - hydrophilic heads face water, hydrophobic tails face each other
- Cholesterol = fluidity buffer
- Integral proteins penetrate membrane; peripheral proteins sit on surface
- Simple diffusion: no protein, no energy, linear kinetics
- Facilitated diffusion: carrier protein, no energy, saturation kinetics (Vmax, Km)
- Active transport: moves AGAINST gradient, requires energy (directly or indirectly)
- Na+/K+ ATPase: 3 Na+ OUT, 2 K+ IN, 1 ATP consumed, electrogenic pump
- Resting membrane potential = -70 mV (mainly K+ equilibrium potential = -94 mV, modified by Na+ leak)
- Normal ICF K+ = 140 mEq/L; ECF K+ = 4 mEq/L
- Normal ICF Na+ = 14 mEq/L; ECF Na+ = 142 mEq/L
- Osmolality formula = 2[Na+] + Glucose/18 + BUN/2.8 = 285-295 mOsm/kg
- GLUT-4 is insulin-dependent; GLUT-2 is the β-cell glucose sensor (high Km)
- Secondary active transport uses Na+ gradient (indirectly uses ATP)
- Digoxin: blocks Na+/K+ ATPase → ↑ICF Na+ → ↑ICF Ca²+ via NCX reversal → ↑contractility
- Furosemide blocks NKCC2 (Na+/K+/2Cl-) in thick ascending limb
- SGLT-2 inhibitors block glucose reabsorption in PCT → glucosuria + cardiovascular protection
- Lysosomes: acid hydrolases, pH 5, lysosomal storage disease = missing enzyme
- Mitochondria: double membrane, cristae, own DNA, maternal inheritance
- CF: CFTR mutation → Cl- transport failure → thick mucus → recurrent infections
Clinical Pearls
- Hypokalemia worsens digoxin toxicity: Low ECF K+ → less competition with digoxin for the K+ binding site on Na+/K+ ATPase → more pump blockade → more toxicity
- Exercise triggers GLUT-4 translocation without insulin - via AMPK activation. This is why exercise improves glucose control in Type 2 DM even when insulin resistance is present
- Cholera treatment is ORS (Oral Rehydration Solution): Even though cholera blocks active Cl- secretion via cAMP, the SGLT-1 co-transporter is unaffected. ORS contains glucose + Na+ → SGLT-1 brings Na+ in → water follows by osmosis → rehydration. Ingenious physiology!
- Potassium shift: Insulin and β₂-agonists drive K+ INTO cells (activate Na+/K+ ATPase) → used therapeutically in hyperkalemia. Acidosis drives K+ OUT of cells in exchange for H+ → extracellular hyperkalemia
━━━━━━━━━━━━━━━━━━━━
STAGE 19: CLINICAL CASES
━━━━━━━━━━━━━━━━━━━━
Case 1 - Basic Level
A 2-year-old child is brought to the emergency with profuse watery diarrhea for 2 days. Stool is pale, rice-water in appearance. Child is lethargic with sunken eyes, dry mucous membranes, and capillary refill > 3 seconds. Stool culture reveals Vibrio cholerae.
Questions:
- What is the cellular mechanism causing the diarrhea?
- Why is ORS effective despite active secretion occurring?
- What electrolyte abnormalities do you expect?
- If the ECF becomes severely hypotonic (from water replacement without Na+), what would happen to the brain cells?
Case 2 - Intermediate Level
A 65-year-old man with hypertension and heart failure is on digoxin. He also takes furosemide. He presents with nausea, visual disturbances (yellow-green halos), and palpitations. ECG shows frequent premature ventricular contractions. Serum K+ = 2.9 mEq/L.
Questions:
- Why is this patient experiencing digoxin toxicity?
- What is the cellular mechanism of digoxin's therapeutic effect?
- How does furosemide contribute to this presentation?
- What is the specific ion that worsens digoxin toxicity and why?
- What are your immediate treatment steps?
Case 3 - Advanced Level
A 15-year-old boy is diagnosed with Cystic Fibrosis (ΔF508 mutation). He has recurrent Pseudomonas lung infections, pancreatic insufficiency, and is azoospermic. A new drug combination (Trikafta - Elexacaftor/Tezacaftor/Ivacaftor) is started.
Questions:
- Explain the cellular mechanism of disease from gene mutation to thick mucus.
- Why does CF cause pancreatic insufficiency?
- Why is 98% of male CF patients infertile?
- How does Ivacaftor work at the cellular level?
- Why is glucose absorption in the gut UNAFFECTED in CF (SGLT-1 still works)?
Try to answer these cases using the physiology you just learned. Solutions and reasoning are available upon request.
━━━━━━━━━━━━━━━━━━━━
STAGE 20: ACTIVE RECALL - MCQs
━━━━━━━━━━━━━━━━━━━━
Question 1:
The Na+/K+ ATPase pump is described as "electrogenic." This means:
- A. It requires electricity to function
- B. It generates an electrical potential by moving unequal charges across the membrane
- C. It neutralizes the membrane potential
- D. It only transports charged ions
(Answer: B - 3 Na+ out, 2 K+ in = net 1 positive charge out per cycle = creates negativity inside)
Question 2:
A patient is given intravenous 5% dextrose (D5W). Initially this is isotonic, but after glucose is metabolized, the solution effectively becomes:
- A. Hypertonic
- B. Isotonic
- C. Hypotonic
- D. Isotonic then hypertonic
(Answer: C - Pure water remains after glucose metabolism → hypotonic → water enters cells → cells swell)
Question 3:
Which of the following statements about facilitated diffusion is CORRECT?
- A. It can move substances against concentration gradients
- B. It directly requires ATP
- C. It shows saturation at high substrate concentrations
- D. It occurs only in the nervous system
(Answer: C - Facilitated diffusion uses carrier proteins that saturate at Vmax - classic distinguishing feature)
Question 4:
ASSERTION: Digoxin is used in heart failure.
REASON: Digoxin inhibits Na+/K+ ATPase, leading to intracellular Ca²+ accumulation and stronger cardiac contraction.
- A. Both A and R are true and R is the correct explanation of A
- B. Both A and R are true but R is not the correct explanation of A
- C. A is true but R is false
- D. A is false but R is true
(Answer: A - Both correct; R explains exactly how digoxin achieves positive inotropy)
Question 5:
A patient with Type 2 Diabetes is started on empagliflozin. The mechanism of glucose lowering involves:
- A. Inhibition of GLUT-4 translocation
- B. Inhibition of Na+/glucose co-transporter in proximal convoluted tubule
- C. Stimulation of insulin secretion from β-cells
- D. Inhibition of hepatic glucose production
(Answer: B - SGLT-2 inhibitors block Na+/glucose co-transport (secondary active transport) in PCT → glucose lost in urine)
Question 6:
The MOST abundant intracellular cation is:
- A. Sodium (Na+)
- B. Calcium (Ca²+)
- C. Potassium (K+)
- D. Magnesium (Mg²+)
(Answer: C - K+ = 140 mEq/L inside cells; Na+ is mostly outside (142 mEq/L ECF))
Question 7:
Which organelle is CORRECTLY matched with its function?
- A. Smooth ER - Protein synthesis
- B. Rough ER - Steroid hormone synthesis
- C. Golgi apparatus - Final modification and packaging of proteins
- D. Lysosome - ATP production
(Answer: C - Golgi modifies, packages and dispatches proteins. Smooth ER = steroids. Rough ER = protein synthesis. Mitochondria = ATP.)
Question 8:
A 4-year-old presents with progressive neurodegeneration, a cherry-red spot on the macula, and exaggerated startle response. The deficient enzyme is:
- A. Glucocerebrosidase
- B. Hexosaminidase A
- C. Sphingomyelinase
- D. α-L-iduronidase
(Answer: B - Tay-Sachs disease = hexosaminidase A deficiency → GM2 ganglioside accumulates in neurons → neurodegeneration. Cherry-red spot is classic.)
Source: Guyton and Hall Textbook of Medical Physiology (14th Edition), Chapters 2 and 4.
- Guyton & Hall, pp. 22-75
What's Next?
You have now completed Cell Physiology from absolute basics to advanced clinical mastery. The next logical topic in the Guyton & Hall sequence is:
- Membrane Potentials and Action Potentials (Chapter 5) - How nerve cells fire
- Contraction of Skeletal Muscle (Chapter 6) - Cell physiology applied to movement
- Nerve Fiber Physiology - Conduction, velocity, classification
Just say "Continue with Action Potentials" or "Teach me [any topic]" and I will deliver the same complete framework.