A clinical scenario in which a 30 yr old patient has hemoglobin 19.5 and when walks about 250 m takes rest and feels dyspnea
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
secondary polycythemia erythrocytosis hypoxia management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have comprehensive information to deliver a thorough clinical analysis. Let me put it all together.
Clinical Analysis: 30-Year-Old with Hb 19.5 g/dL and Exertional Dyspnea at ~250 m
Immediate Clinical Impression
A 30-year-old with hemoglobin of 19.5 g/dL (markedly elevated - normal male upper limit ~17.5 g/dL) plus dyspnea on minimal exertion (250 m walk) is a classic presentation pointing to secondary polycythemia (erythrocytosis) from chronic hypoxia, most likely from a cyanotic/right-to-left shunting lesion or significant pulmonary disease. At this young age, cyanotic congenital heart disease (Eisenmenger syndrome, Tetralogy of Fallot) is a strong leading diagnosis. Polycythemia vera is less likely at age 30 but must be excluded.
Why Is the Hemoglobin So High?
Hb 19.5 g/dL represents absolute erythrocytosis - a true increase in red cell mass. The body raises EPO in response to tissue hypoxia, driving compensatory RBC production. This increases oxygen-carrying capacity but also raises blood viscosity, which paradoxically worsens cardiopulmonary function and can cause thrombosis. - Harrison's Principles of Internal Medicine 22E, p. 495
Differential Diagnosis (Structured by Likelihood)
1. Secondary Polycythemia - Hypoxia-Driven (Most Likely at Age 30)
The most important category in a young patient. From Tintinalli's Emergency Medicine:
| Cause | Key Features |
|---|---|
| Cyanotic congenital heart disease (Eisenmenger, ToF, TAPVR) | Cyanosis, clubbing, right-to-left shunt |
| Chronic pulmonary disease (severe asthma, ILD, COPD) | Wheezing, crackles, reduced FEV1/FVC |
| Obstructive sleep apnea | Obesity, snoring, daytime somnolence |
| High-altitude habitat | Recent move to altitude, resolves at sea level |
| Chronic CO poisoning | History of indoor heater exposure |
At age 30, Eisenmenger syndrome or uncorrected VSD/ASD/PDA with reversal is particularly important: these patients develop pulmonary hypertension from long-standing left-to-right shunts, eventually reversing flow and causing systemic cyanosis + polycythemia. They present with progressive dyspnea on exertion, cyanosis, and clubbing. - Harrison's 22E; Braunwald's Heart Disease
2. Primary Polycythemia (Polycythemia Vera) - Less Likely But Must Exclude
PV is characterized by a JAK2 V617F mutation (found in 95-98% of cases). It typically presents in older adults but can occur at 30. Key distinguishing features:
- Elevated WBC and platelets (not just RBC)
- Splenomegaly
- Pruritus after hot bathing (aquagenic pruritus)
- Low or undetectable serum EPO
- JAK2 mutation positive
- Normal oxygen saturation
3. Congenital/Hereditary Causes
- High-oxygen-affinity hemoglobinopathy (hemoglobin shifts left, releases less O2, drives EPO)
- 2,3-BPG deficiency
- Chuvash polycythemia (VHL gene mutation)
- EPO receptor mutations
- Family history important; erythrocytosis mutation panels now available
4. Spurious (Relative) Polycythemia
- Decreased plasma volume (dehydration, burns, diuretics)
- Hematocrit elevated, but RBC mass is actually normal
- Less likely with Hb 19.5 g/dL plus symptoms
Diagnostic Algorithm
This is exactly the scenario described in Harrison's diagnostic flowchart:
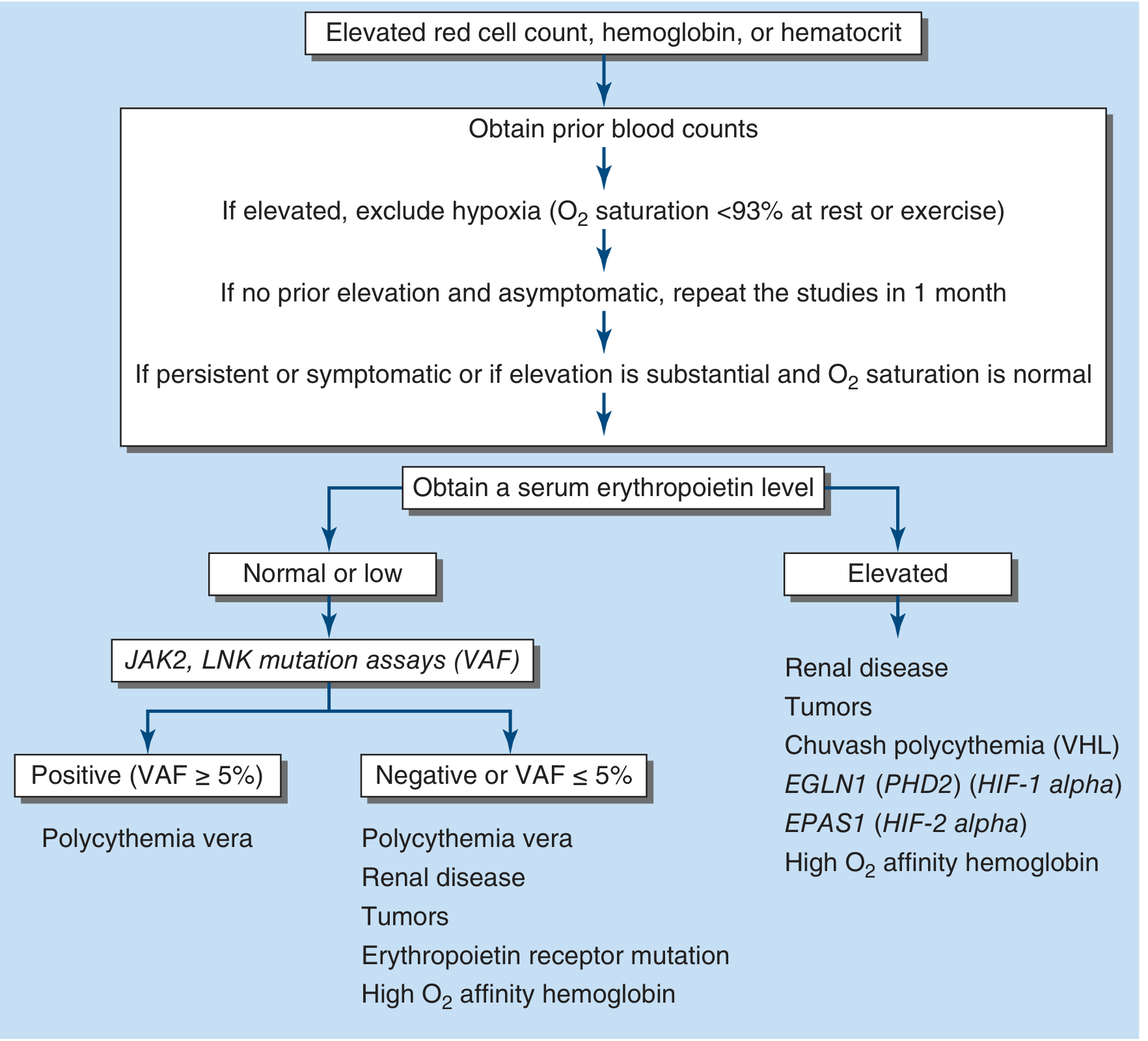
Harrison's Principles of Internal Medicine 22E, Fig. 56-18 - Approach to differential diagnosis of elevated hemoglobin
Step-by-step workup:
- Pulse oximetry (SpO2) - first and most critical test
- SpO2 <93% at rest or exercise → hypoxia-driven secondary cause
- SpO2 normal → consider PV, high-affinity hemoglobin, EPO tumor
- Serum EPO level
- Low/undetectable → strongly suggests Polycythemia Vera → test for JAK2 mutation
- Elevated → secondary erythrocytosis from hypoxia or autonomous EPO production
- ABG + co-oximetry - assess PaO2, true O2 saturation, rule out CO poisoning or methemoglobin
- Chest X-ray + Echocardiography - detect cardiac shunts, pulmonary hypertension
- ECG - right ventricular hypertrophy, right axis deviation (suggests pulmonary hypertension)
- CBC with differential - isolated RBC rise suggests secondary; pancytosis (RBC+WBC+platelets) suggests PV
- Abdominal ultrasound - splenomegaly supports PV; also check kidneys for tumors/cysts
- JAK2 V617F mutation (if EPO low or normal)
- Bone marrow biopsy - if PV is suspected but molecular testing is inconclusive
- Erythrocytosis mutation panel (VHL, HIF2A, PHD2, EPO receptor) - if congenital cause suspected
Clinical Features to Look For on Examination
| Finding | Suggests |
|---|---|
| Cyanosis + clubbing | Right-to-left shunt (Eisenmenger, ToF) |
| Ruddy complexion, plethoric face | Polycythemia vera or any erythrocytosis |
| Splenomegaly | Polycythemia vera |
| Loud P2, RV heave, TR murmur | Pulmonary hypertension / Eisenmenger |
| Wheeze / reduced air entry | Chronic pulmonary disease |
| Obesity, large neck | OSA |
| Heart murmur (from childhood) | Congenital heart disease |
Importantly, from Harrison's 22E: "The presence of cyanosis or evidence of a right-to-left shunt suggests congenital heart disease presenting in the adult, particularly tetralogy of Fallot or Eisenmenger's syndrome."
Pathophysiology of Dyspnea in This Patient
The dyspnea is multifactorial:
- Primary hypoxia - if shunt or lung disease is the driver, low SpO2 directly limits exercise
- Hyperviscosity - Hb 19.5 raises blood viscosity sharply, increasing pulmonary artery pressure and cardiac afterload
- Reduced O2 offloading at tissues (in high-affinity hemoglobinopathy) - tissues are starved despite elevated Hb
- Cor pulmonale - chronic hypoxemia causes pulmonary vasoconstriction → right heart strain → reduced cardiac output on exertion - Harrison's 22E, p. 2513
Management Approach
Treat the underlying cause first. The hemoglobin elevation is compensatory in secondary polycythemia - aggressively reducing it without treating the cause is dangerous.
| Scenario | Management |
|---|---|
| Secondary polycythemia (hypoxia-driven) | Treat the underlying cause (supplemental O2, CPAP for OSA, cardiac surgery/catheter intervention for shunts). Cautious phlebotomy only if symptoms of hyperviscosity are severe (headache, visual changes, stroke risk) - do NOT target low hematocrit as it removes the compensatory benefit |
| Eisenmenger syndrome | Specialist management: endothelin receptor antagonists (bosentan), PDE5 inhibitors (sildenafil), careful phlebotomy with iso-volume replacement |
| Polycythemia vera | Low-dose aspirin + phlebotomy to hematocrit ≤45%. Hydroxyurea, interferon-α, or ruxolitinib (JAK1/JAK2 inhibitor) for high-risk patients after risk stratification. Hematology referral. - Tintinalli's Emergency Medicine |
| Relative polycythemia | IV/oral hydration, address underlying fluid loss |
Key warning: Never aggressively phlebotomize a patient with secondary polycythemia from a right-to-left shunt without replacing volume - it drops cardiac output and can cause hemodynamic collapse.
Summary
| Feature | Clinical Significance |
|---|---|
| Age 30 + Hb 19.5 | Chronic compensatory erythrocytosis more likely than PV |
| Dyspnea at 250 m | Significant cardiopulmonary limitation (NYHA class II-III) |
| Most likely diagnosis | Secondary polycythemia from cyanotic CHD (Eisenmenger/ToF) or severe pulmonary disease |
| Key initial test | Pulse oximetry + Echo + Serum EPO + JAK2 mutation |
| Red flags | SpO2 <93%, cyanosis, clubbing, RV hypertrophy on ECG |
Recent evidence note: A 2025 review on JAK2-unmutated erythrocytosis management (PMID 41123216, Am J Hematol 2025) updates the diagnostic and management approach for non-PV erythrocytosis, reinforcing the need for systematic molecular evaluation before treatment decisions.
Sources consulted:
- Harrison's Principles of Internal Medicine 22E (2025), Chapters 56 & 280
- Tintinalli's Emergency Medicine - A Comprehensive Study, Chapter 231
- Textbook of Family Medicine 9e, Chapter 14
- Goldman-Cecil Medicine International Edition, Chapter 152
- Braunwald's Heart Disease - A Textbook of Cardiovascular Medicine
He has this condition since childhood
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent - I now have very rich, authoritative content. Here is the refined, focused clinical analysis.
Revised Clinical Analysis: Condition Since Childhood
The key detail - symptoms/condition since childhood - locks in the diagnosis to cyanotic congenital heart disease (CHD) as the cause of secondary polycythemia. This is now a near-certain diagnosis until proven otherwise. Polycythemia vera, OSA, and acquired lung disease do not present from childhood.
The Diagnosis: Cyanotic Congenital Heart Disease with Secondary Erythrocytosis
The two dominant diagnoses to consider are:
1. Eisenmenger Syndrome (Most Likely in a 30-Year-Old Surviving to Adulthood)
What happens: A patient is born with a large left-to-right shunt (VSD, ASD, PDA, AVSD). Over years, the chronic high-volume/high-pressure pulmonary blood flow causes irreversible pulmonary vascular injury and pulmonary arterial hypertension (PAH). When pulmonary vascular resistance (PVR) finally exceeds systemic vascular resistance (SVR), blood flow reverses - now flowing right-to-left, mixing deoxygenated blood into the systemic circulation. This is Eisenmenger syndrome. - Harrison's 22E
Chronic cyanosis then drives EPO production → secondary erythrocytosis with Hb rising well above 19 g/dL (hematocrit >60% is common in these patients). - Braunwald's Heart Disease
Typical history at age 30:
- Known heart defect since birth (murmur noted in infancy)
- Possibly told "too risky" for surgery as a child, or surgery not available (common in low/middle-income countries)
- Progressive effort intolerance over years - now limited to 250 m
- Cyanosis and clubbing noted since childhood
Clinical features to find in this patient:
| Sign | Finding |
|---|---|
| Central cyanosis | Bluish lips, tongue, mucous membranes |
| Digital clubbing | Bulbous fingertips + toes (from chronic hypoxia since childhood) |
| Right parasternal heave | Right ventricular hypertrophy |
| Loud P2 | Elevated pulmonary artery pressure |
| Diastolic murmur | Pulmonary regurgitation from dilated PA |
| Systolic murmur faint or absent | Shunt equalization - pressure equal on both sides means no flow gradient |
| Elevated JVP with prominent a-wave | Right heart pressure overload |
Below is a real clinical photograph from Braunwald's Heart Disease showing the hallmark of Eisenmenger syndrome - note the digital clubbing and cyanosis on the affected hand (right) vs. a healthy family member (left):

Lab findings typical for Eisenmenger syndrome (from Braunwald's Heart Disease, Table 82.15):
| Investigation | Expected Finding |
|---|---|
| SpO2 | Low (<93%, often 75-85%) |
| Hb / Hematocrit | Very high (Hb 18-22 g/dL, Hct often >60%) |
| Serum EPO | Elevated (appropriate secondary response) |
| Iron stores | Often iron-deficient despite polycythemia - iron is chronically consumed driving RBC production |
| BNP | Elevated (RV strain) |
| Uric acid | Elevated (hyperuricemia from cell turnover) |
| Platelet count | Often low (thrombocytopenia) |
| WBC | Leukopenia possible |
| ECG | Right axis deviation, RVH, right atrial enlargement |
| CXR | Dilated central pulmonary arteries, peripheral "pruning," enlarged RV/RA |
| Echo | RV enlargement, RV hypertrophy, elevated RVSP, large shunt defect, low-velocity bidirectional flow |
2. Tetralogy of Fallot (ToF) - Unrepaired or with Residual Defect
ToF is the most common cause of cyanotic CHD beyond infancy. Its four components: RVOTO + large unrestrictive VSD + overriding aorta + RVH. Deoxygenated blood is shunted right-to-left across the VSD, bypassing the lungs.
From Rosen's Emergency Medicine: "Chronic hypoxemia results in a compensatory polycythemia and varying degrees of clubbing of the fingers and toes."
Key differences from Eisenmenger:
- In ToF, pulmonary blood flow is reduced from the start (not over-circulated)
- Cyanosis is present from infancy/early childhood
- "Tet spells" in infancy (paroxysmal hypercyanotic episodes during exertion/crying)
- Squatting behavior in childhood (increases SVR, reduces right-to-left shunt)
- CXR shows classic "boot-shaped heart" (coeur en sabot) with decreased pulmonary vascular markings
- If unrepaired and the patient has survived to age 30, significant collateral circulation has usually developed
Why the Polycythemia Is So High (Hb 19.5) - The Compensatory Loop
Chronic right-to-left shunt
↓
Systemic arterial hypoxemia (SpO2 chronically 75-90%)
↓
Renal peritubular cells detect low O2 tension
↓
Increased EPO secretion
↓
Bone marrow: increased erythropoiesis
↓
Hb rises to 19.5 g/dL → augments O2 delivery to tissues
↓
BUT: Blood viscosity rises sharply
↓
Increased PVR + reduced cardiac output on exertion
↓
Dyspnea at 250 m (NYHA Class III functional limitation)
The polycythemia is the body's attempt to compensate - it is adaptive and necessary. Without it, tissues would be profoundly hypoxic.
Serious Complications in This Patient
Because of the hyperviscosity + right-to-left shunt, this patient faces:
| Complication | Mechanism |
|---|---|
| Paradoxical embolism / stroke | Clot or air bypasses pulmonary filter via shunt → goes directly to brain |
| Brain abscess | Bacteria bypass pulmonary filter |
| Hemoptysis | Rupture of dilated pulmonary vessels |
| Gout | Hyperuricemia from high RBC turnover |
| Iron deficiency | Despite high Hb - iron consumed by erythropoiesis |
| Infective endocarditis | Turbulent flow at shunt site |
| Sudden cardiac death | Arrhythmia from RV pressure overload |
Management Principles (Critical Points)
From Braunwald's Heart Disease (Table 82.16 - Conditions to Avoid in Eisenmenger Syndrome):
DO NOT:
- DO NOT perform routine phlebotomy - this is the single most important principle. Phlebotomy in Eisenmenger/cyanotic CHD increases stroke risk and worsens iron deficiency. The erythrocytosis is compensatory - removing blood removes the only mechanism the patient has to deliver oxygen.
- DO NOT give estrogen (thrombotic risk) - critical for female patients
- DO NOT allow pregnancy (>30% maternal mortality - absolutely contraindicated)
- DO NOT allow volume depletion (worsens hyperviscosity)
- DO NOT give routine anesthesia without cardiac anesthesiologist (very high operative risk)
- DO NOT use calcium channel blockers for PAH (negative inotropy destabilizes the RV)
ACTIVE MANAGEMENT:
| Intervention | Details |
|---|---|
| Correct iron deficiency | Iron supplements (judiciously, with monitoring) - iron deficiency worsens hyperviscosity and symptoms even without anemia |
| Pulmonary vasodilators | Bosentan (endothelin receptor antagonist) - improved exercise capacity and hemodynamics in BREATH-5 trial (VSD/ASD/PDA). Sildenafil (PDE5 inhibitor) - evidence from smaller trials. |
| Hydration | Volume repletion is usually the first-line management for hyperviscosity symptoms |
| Phlebotomy - restricted use | Only for symptomatic hyperviscosity (headache, visual changes, paresthesias) + patient is iron-replete + volume-replete. Must be accompanied by isovolume saline replacement |
| Antibiotic prophylaxis | All cyanotic CHD patients - required before dental/surgical procedures |
| Anticoagulation | Controversial - weighed against bleeding risk |
| Transplantation | Combined heart-lung transplant or lung transplant + cardiac repair for advanced refractory disease |
| ACHD specialist centre | Must be managed at a comprehensive Adult Congenital Heart Disease (ACHD) centre, seen at least annually |
Investigations to Order Now
- SpO2 at rest and on exertion (will likely be 75-88%)
- 12-lead ECG - right axis deviation, RVH, right atrial enlargement
- CXR - cardiomegaly pattern (ToF: boot-shaped, Eisenmenger: dilated PAs with pruning)
- Transthoracic echocardiogram - identifies the shunt anatomy, estimates RVSP, RV function
- CBC with differential - confirm polycythemia, check for thrombocytopenia, leukopenia
- Serum iron, ferritin, TIBC - iron deficiency common and worsens outcome
- Serum EPO - will be elevated (confirming secondary etiology)
- Uric acid, renal function, LFTs, BNP
- Cardiac MRI or CT angiography - detailed anatomy of shunt, PA size, RV volumes
- 6-minute walk test - baseline functional capacity, prognostic value
Prognosis
From Braunwald's Heart Disease: "Death during childhood is rare but becomes much more common during the 4th decade of life or later." This 30-year-old is entering the highest-risk period. Predictors of worse survival: lower resting SpO2, non-sinus rhythm, pericardial effusion, poor 6-minute walk distance.
Adults with Eisenmenger syndrome actually survive longer than other forms of severe PAH due to the adaptive effects of the RV being "trained" since birth, but they carry significant morbidity. Referral to an ACHD specialist centre is mandatory.
Sources:
- Braunwald's Heart Disease, 2-Vol Set, Chapter 82 (Eisenmenger Syndrome section, Tables 82.14, 82.15, 82.16)
- Harrison's Principles of Internal Medicine 22E, Chapter 280 (Specific CHD Lesions - Eisenmenger Syndrome)
- Rosen's Emergency Medicine, Chapter 165 (Tetralogy of Fallot)
This is a shared conversation. Sign in to Orris to start your own chat.