anti arrythmics
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
Vaughan Williams antiarrhythmic drug classification action potential
I now have comprehensive data. Let me compile a thorough reference on antiarrhythmic drugs.
Antiarrhythmic Drugs
Mechanisms of Arrhythmia (Context)
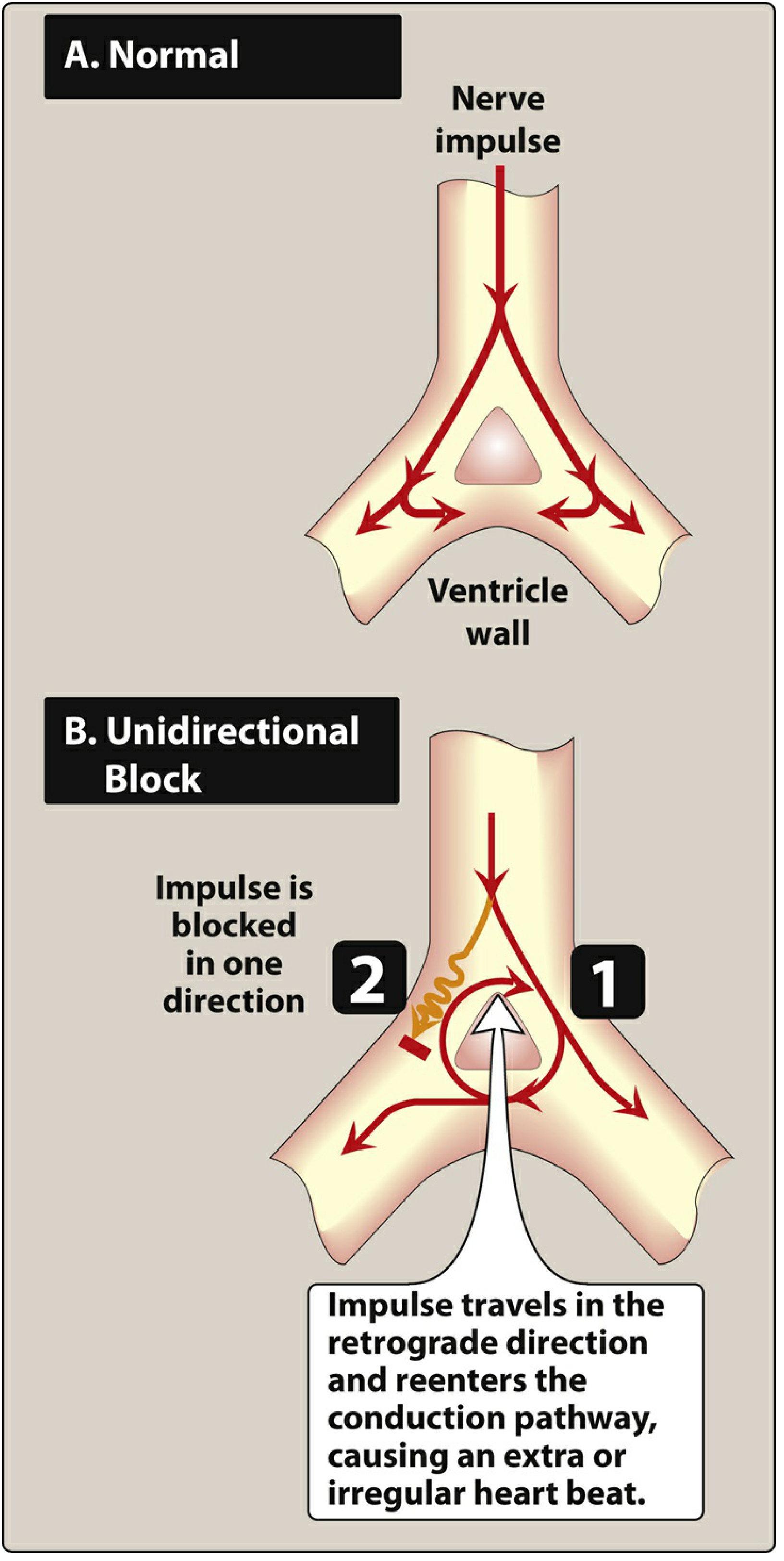
Arrhythmias arise from two main mechanisms:
- Abnormal automaticity — ectopic pacemaker activity
- Reentry — a unidirectional block allows an impulse to travel retrogradely and re-excite proximal tissue, generating a circus loop
Antiarrhythmic drugs modify impulse generation and conduction to suppress these mechanisms. A critical caveat: many are proarrhythmic themselves, particularly by prolonging the QT interval → risk of torsades de pointes (TdP).
Vaughan-Williams Classification
The dominant framework, grouping drugs by their predominant effect on the cardiac action potential. Note its limitations — many drugs span multiple classes (amiodarone acts on all four), and some drugs (adenosine, digoxin) don't fit at all.
Class I — Sodium Channel Blockers
Block fast inward Na⁺ channels → slow Phase 0 depolarization. Subclassified by kinetics of Na⁺ channel binding:
| Subclass | Kinetics | Potency | Effect on AP | Drugs |
|---|---|---|---|---|
| IA | Intermediate | Moderate | Slows Phase 0; prolongs repolarization (↑QT) | Quinidine, Procainamide, Disopyramide |
| IB | Fast | Low | Slows Phase 0; shortens Phase 3 repolarization (↓QT) | Lidocaine, Mexiletine |
| IC | Slow | High | Markedly slows Phase 0; minimal effect on repolarization | Flecainide, Propafenone |
Class IA
Quinidine
- Blocks Na⁺, IKr, IKs, Ito, and KATP channels; also α-adrenergic and anticholinergic effects
- Prolongs QT via IKr block (reverse use-dependent — more effect at slow rates → TdP risk)
- Unique use: Brugada syndrome and idiopathic VF (blocks Ito)
- Side effects: Cinchonism (tinnitus, visual disturbances, headache), hemolytic anemia, esophagitis, QT prolongation, TdP
- Hemodynamics: vasodilation via α-blockade → hypotension
Procainamide
- Similar to quinidine but less anticholinergic
- Active metabolite NAPA has Class III (K⁺ channel blocking) properties
- Key adverse effect: Lupus-like syndrome (ANA positive in 80%; symptomatic in ~30% with long-term use), also hypotension
Disopyramide
- Strongest anticholinergic effects of the class → dry mouth, urinary retention, blurred vision, constipation
- Negative inotrope — avoid in heart failure
Class IB
Lidocaine
- IV only (extensive first-pass if oral)
- Preferentially affects ischemic/depolarized tissue (use-dependent)
- Primary use: ventricular arrhythmias, especially post-MI and reperfusion
- Side effects: CNS — tremor, ataxia, paresthesias, confusion, seizures (dose-dependent)
Mexiletine
- Oral analogue of lidocaine
- Used for ventricular arrhythmias and long QT syndrome type 3
- Side effects: N/V, dyspepsia, CNS effects
Class IC
Flecainide & Propafenone
- Most potent Na⁺ channel blockers; markedly slow conduction
- Highly effective for AF/flutter rhythm control and SVT
- ⚠️ CAST trial: Flecainide/encainide increased mortality post-MI → contraindicated in structural heart disease (ischemic or LV dysfunction)
- Propafenone also has mild β-blocking and weak Ca²⁺ channel effects
- Propafenone-specific: bronchospasm, liver toxicity, agranulocytosis
Class II — Beta-Adrenergic Blockers
Block β₁ receptors → inhibit Phase 4 (pacemaker) depolarization in SA and AV nodes → ↓ heart rate, ↓ AV conduction
Key agents: Metoprolol, Atenolol, Esmolol (IV, ultra-short acting), Carvedilol, Propranolol
Uses:
- SVT, atrial flutter/AF (rate control)
- Post-MI (reduce sudden cardiac death)
- Hypertrophic cardiomyopathy, long QT syndrome
Side effects: Bradycardia, heart block, hypotension, bronchospasm (non-selective), fatigue, exercise intolerance, sexual dysfunction, hyperlipidemia
Class III — Potassium Channel Blockers
Block K⁺ channels (primarily Kv11.1 / IKr, encoded by KCNH2) → prolong Phase 2–3 repolarization → ↑ action potential duration → ↑ QT interval
⚠️ QT prolongation is both the therapeutic mechanism and the primary risk (TdP)
| Drug | Key Features |
|---|---|
| Amiodarone | Acts on all 4 classes; most effective AAD overall; extensive toxicity with long-term use |
| Sotalol | Also a potent β-blocker (Class II + III); prominent QT prolongation |
| Dofetilide | Pure IKr blocker; QT prolongation greatest at slow rates (reverse use-dependence); used for AF/flutter |
| Ibutilide | IV only; used solely for acute cardioversion of AF/flutter |
| Dronedarone | Amiodarone analogue without iodine; milder multi-channel effects; less toxicity but contraindicated in permanent AF or decompensated HF |
Amiodarone (Special Focus)
Properties of all four Vaughan-Williams classes:
- Na⁺ channel block (Class I)
- β-blockade (Class II)
- K⁺ channel block — prolongs action potential (Class III, dominant)
- Ca²⁺ channel block (Class IV)
Uses: AF (cardioversion and maintenance), VT/VF, hemodynamically unstable VT
Toxicity (long-term): The most extensive toxicity profile of any AAD:
- Pulmonary toxicity (pneumonitis/fibrosis) — most serious
- Thyroid dysfunction (hypo- or hyperthyroidism — contains 37% iodine by weight)
- Hepatotoxicity
- Corneal microdeposits (nearly universal; rarely affects vision)
- Photosensitivity, blue-grey skin discoloration
- Peripheral neuropathy
- Half-life of 40–55 days → interactions persist long after stopping
Class IV — Calcium Channel Blockers (Non-dihydropyridines)
Block L-type Ca²⁺ channels in SA and AV nodes → ↓ automaticity and AV conduction
Agents: Verapamil, Diltiazem
Uses: SVT (rate control), AF/flutter (rate control), AVNRT
Side effects: Bradycardia, AV block, hypotension, constipation (verapamil)
⚠️ Avoid in WPW — blocking the AV node can accelerate conduction down the accessory pathway
Drugs Outside the Vaughan-Williams Schema
Adenosine
- IV, ultra-short acting (half-life ~10 seconds)
- Activates K⁺ channels in AV node → transient complete AV block
- Drug of choice for terminating AVNRT and diagnosing SVT
- Causes transient flushing, dyspnea, chest tightness — reassure patient
Digoxin
- Inhibits Na⁺/K⁺-ATPase → increases intracellular Ca²⁺ → positive inotropy
- Increases vagal tone → slows AV node conduction (rate control in AF)
- Narrow therapeutic index; toxicity: arrhythmias, N/V, visual changes (xanthopsia)
- Levels increased by hypokalemia, hypomagnesemia
Ranolazine
- Blocks late Na⁺ current (INa-late) → shortens action potential (similar to IB)
- Also K⁺ channel effects
- Used for refractory atrial and ventricular arrhythmias, often in combination
- Well tolerated (dizziness, constipation); avoid strong CYP3A inhibitors/inducers
Clinical Selection Pearls
| Situation | Preferred Agent(s) | Avoid |
|---|---|---|
| Post-MI VT/VF prevention | β-blockers (metoprolol) | Flecainide, Class IA |
| AF rhythm control, structurally normal heart | Flecainide, Propafenone, Sotalol | — |
| AF rhythm control + HF | Amiodarone, Dofetilide | Flecainide, Propafenone, Dronedarone |
| Acute SVT (AVNRT) termination | Adenosine | — |
| SVT/AF rate control | β-blockers, Verapamil, Diltiazem | — |
| VT in ischemic cardiomyopathy | Amiodarone, Sotalol | Class IC agents |
| Brugada syndrome | Quinidine | Na⁺ channel blockers (Class I generally) |
| Long QT type 3 | Mexiletine, Ranolazine | Class IA, III (further QT prolongation) |
| Hemodynamically unstable VT (acute) | Amiodarone IV, Lidocaine IV | — |
| Acute AF cardioversion | Ibutilide IV | — |
Proarrhythmic Risk Summary
All antiarrhythmic drugs carry proarrhythmic potential. The major mechanisms:
- QT prolongation → TdP: Class IA (quinidine, disopyramide), Class III (sotalol, dofetilide, ibutilide), amiodarone (less than others despite QT prolongation)
- Increased mortality in structural heart disease: Class IC (CAST trial)
- Reverse use-dependence: K⁺ channel blockers are most dangerous at slow heart rates (sotalol, dofetilide)
Sources: Lippincott Illustrated Reviews: Pharmacology; Harrison's Principles of Internal Medicine, 22e (2025); Braunwald's Heart Disease, 10e; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.