Essay answer for ENT PG exam - "Choanal Atresia - etiology, pathophysiology, management. Add note on Types & management" under 800 words - images/diagrams/
Reading File
Finding Sources
Searching Images
choanal atresia types CT scan anatomy diagram
Searching PubMed
"choanal atresia"[MeSH Terms] AND management
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the content needed to write a comprehensive, well-illustrated ENT PG exam essay. Here it is:
Choanal Atresia — Etiology, Pathophysiology, Types & Management
Definition & Incidence
Choanal atresia is the absence of communication between the posterior nasal cavity and the nasopharynx due to persistence of an atretic plate at the posterior choana. It is one of the most common congenital nasal anomalies, with an incidence of 1 in 5,000–8,000 live births. Females are affected more than males (2:1). Up to two-thirds of cases are unilateral, with right-side predominance.
Etiology
The etiology is multifactorial — both genetic and environmental factors contribute:
Embryological basis: In normal development, the buccopharyngeal membrane ruptures at 6–7 weeks gestation, establishing posterior nasal communication. Several theories have been proposed for failure of this process:
| Theory | Mechanism |
|---|---|
| Persistence of buccopharyngeal membrane | Failure of rupture of the nasobuccal membrane of Hochstetter |
| Abnormal mesodermal adhesions | Mesodermal ingrowth obliterating the posterior choana |
| Misdirected neural crest cell migration | Aberrant cell migration leads to abnormal bony/membranous plate |
| Local infection/trauma | Environmental insults during embryogenesis |
Associated syndromes: Up to 50% of all choanal atresia patients — and 75% of bilateral cases — have associated congenital anomalies, most notably:
- CHARGE syndrome (Coloboma, Heart defects, Atretic choana, Retardation of growth, Genitourinary disorders, Ear abnormalities) — the most important association
- Crouzon syndrome, craniosynostosis, microcephaly
- Cleft palate, hypertelorism, polydactyly
- Hypoplasia of orbit and midface
Pathophysiology
The anatomic features constituting choanal atresia are:
- Narrow nasal cavity
- Lateral bony obstruction — medialisation of the pterygoid plates
- Medial obstruction — thickening and broadening of the vomer
- Membranous obstruction at the posterior choana
Because neonates are obligate nasal breathers, bilateral atresia produces a dramatic cyclic pattern: the infant attempts nasal breathing → obstruction causes respiratory distress and cyanosis → infant cries → oral breathing restores oxygenation → cycle repeats. This is the pathognomonic "cyclic cyanosis relieved by crying."
Types
Choanal atresia is classified by laterality and composition of the atretic plate:
By Laterality:
| Type | Frequency | Presentation |
|---|---|---|
| Unilateral | ~65% | Later in life; rhinorrhea, unilateral nasal obstruction, thick secretions |
| Bilateral | ~35% | Neonatal emergency; cyclic cyanosis, respiratory distress |
By Composition (Morgagni's classification):
| Type | Frequency | Features |
|---|---|---|
| Bony (osseous) | ~29% | Complete bony plate; dense on CT |
| Mixed (bony-membranous) | ~71% | Bony + soft tissue component; most common |
| Membranous | Rare/nil | Pure membranous — practically absent per current studies |
Per Cummings Otolaryngology: "No patients were found to have a purely membranous atresia" — the traditional teaching of 90% bony/10% membranous is now revised to ~29% bony and 71% mixed bony-membranous.
Diagnosis
Clinical: Failure to pass a 6-F catheter 32 mm into the nasopharynx. Pooling of secretions in the occluded nasal cavity.
Nasal endoscopy: Direct visualisation with a 120° nasopharyngoscope confirms the atretic plate and differentiates atresia from stenosis (choana < 6 mm = stenosis).

Fig. 1 — Bilateral choanal atresia viewed through a 120° nasopharyngoscope (Cummings Otolaryngology)
CT scan (gold standard): Axial cuts at the level of the posterior choana confirm bony vs. membranous nature, plate thickness, and vomerine broadening. Nasal decongestion/suctioning before imaging improves resolution.
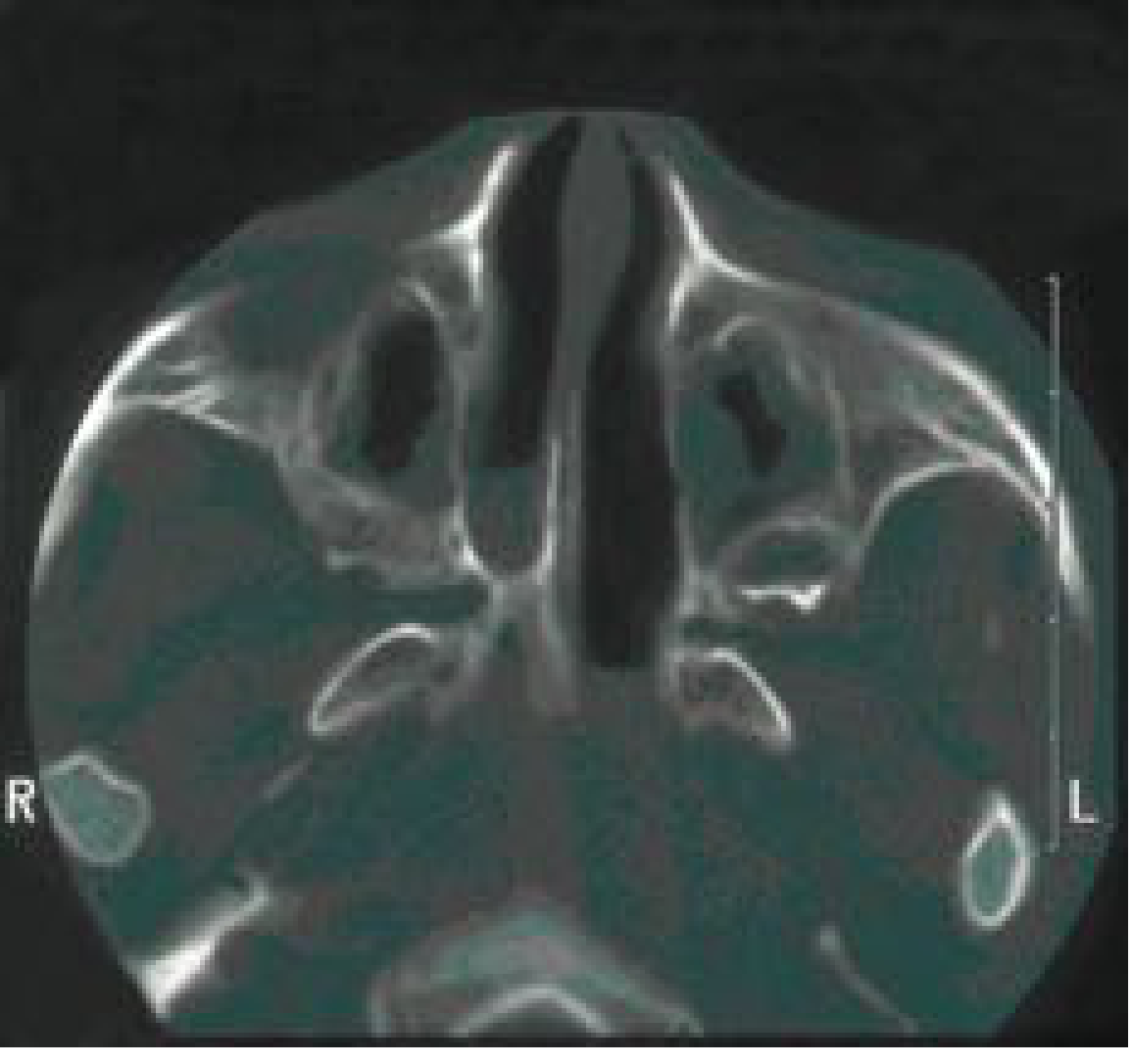
Fig. 2 — Axial CT: unilateral bony choanal atresia with associated soft tissue (Cummings Otolaryngology)
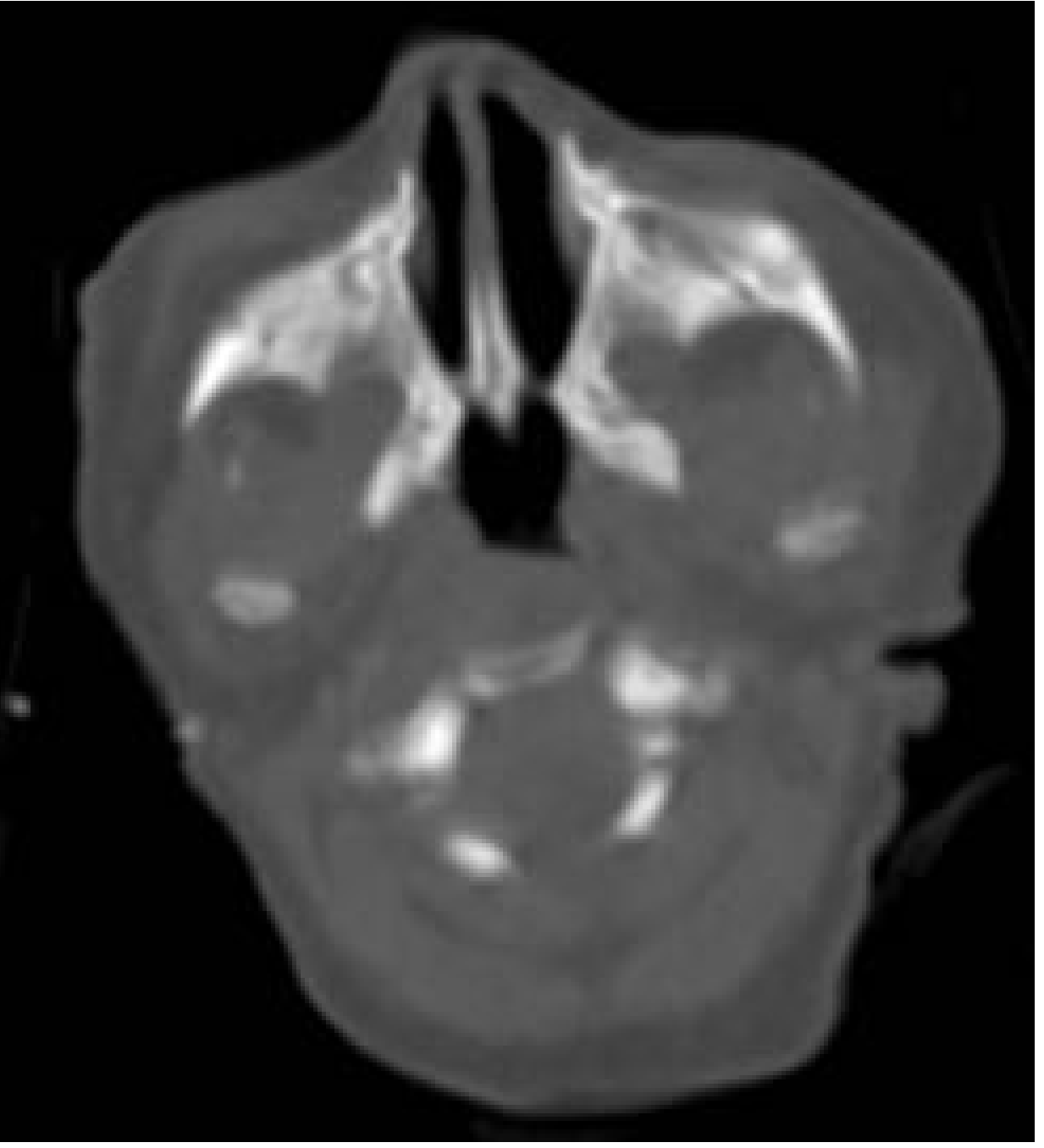
Fig. 3 — Axial CT: bilateral choanal atresia (Cummings Otolaryngology)

Fig. 4 — Axial CT: bilateral mixed-type choanal atresia in a 1-month-old — note bony plate (right) and mixed plate (left), medialization of pterygoid plates, vomerine thickening
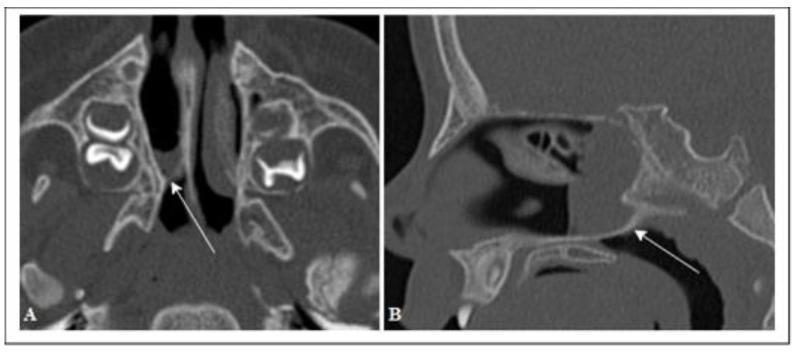
Fig. 5 — CT axial (A) and sagittal (B): unilateral right mixed choanal atresia, arrows indicate atresia wall
Management
Immediate (Bilateral Atresia — Neonatal Emergency):
- Oral airway (McGovern nipple) or orotracheal intubation to establish airway
- Supplemental oxygen
- NG tube feeding or gastrostomy if oral feeding impaired
- Tracheotomy only in cases of multiple-level airway obstruction or respiratory failure
Surgical Repair:
Timing:
- Bilateral atresia: Surgery after initial airway stabilisation; ideally wait several months for adequate facial growth (analogous to cleft lip repair timing), unless respiratory compromise demands earlier intervention
- Unilateral atresia: May be safely delayed months to years — allows nasal growth and reduces risk of restenosis
Surgical approaches:
| Approach | Details | Preferred? |
|---|---|---|
| Transnasal endoscopic | 0° endoscope; urethral sound to perforate plate at thinnest point; backbiting forceps, microdebrider, drill, or laser to remove tissue and bone | Current gold standard |
| Transpalatal | Pedicled hard palate mucoperiosteal flap (based on greater palatine artery) elevated to expose choanae | Older approach; used for revision or complex anatomy |
| Transeptal | Via septal window | Rarely used |

Fig. 6 — Transpalatal repair: mucoperiosteal flap elevated exposing the choanae (Cummings Otolaryngology)
Transnasal endoscopic technique:
- Topical decongestion and vasoconstriction
- Perforate atretic plate with urethral sound at its thinnest portion
- Enlarge with backbiting forceps, microdebrider, drill, or KTP/CO₂ laser
- Landmark: posterior tip of middle turbinate — stay inferior to avoid intracranial injury
- Create adequate choanal opening with mucosal flap preservation
Adjunctive measures (controversial):
- Stenting: Silastic stents post-repair to maintain patency; duration 4–6 weeks (now debated)
- Mitomycin C (fibroblast inhibitor): Topical application to reduce scar fibrosis and restenosis
- Mucosal flap preservation: Minimising mucosal trauma correlates with lower restenosis rates
Complications:
- Restenosis — most common; rates highest in neonates and syndromic cases
- Intracranial injury (if dissection superior to middle turbinate)
- Revision surgery often required
Note on Types of Choanal Atresia & Type-Specific Management
| Type | Key Feature | Management Consideration |
|---|---|---|
| Unilateral bony | Dense plate, unilateral | Delay surgery; transnasal endoscopic approach |
| Bilateral bony | Neonatal emergency | Urgent airway, then staged endoscopic repair |
| Mixed bony-membranous | Most common (71%); combined obstruction | Transnasal drill + microdebrider; more tissue removal needed |
| Bilateral vs. unilateral | Syndromic associations higher with bilateral | Screen for CHARGE; multidisciplinary management |
Prognosis is better in older children and non-syndromic, unilateral cases — these have the lowest recurrence rates after repair. Bilateral syndromic cases carry higher surgical morbidity and restenosis risk.
Sources: Cummings Otolaryngology: Head & Neck Surgery (7th ed.); Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.