Heart Sound medicine ug
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive information from multiple authoritative textbooks. Let me compile the complete answer.
Heart Sounds - Complete UG Medicine Guide
Sources: Guyton & Hall Medical Physiology, Fuster & Hurst's The Heart 15th Ed., Harrison's Principles of Internal Medicine 22E, Harriet Lane Handbook 23rd Ed., Goldman-Cecil Medicine
Overview
Normal cardiac auscultation produces the classic "lub-dub" sound pattern. These sounds arise from valve closure and associated blood/wall vibrations.
Auscultation Areas
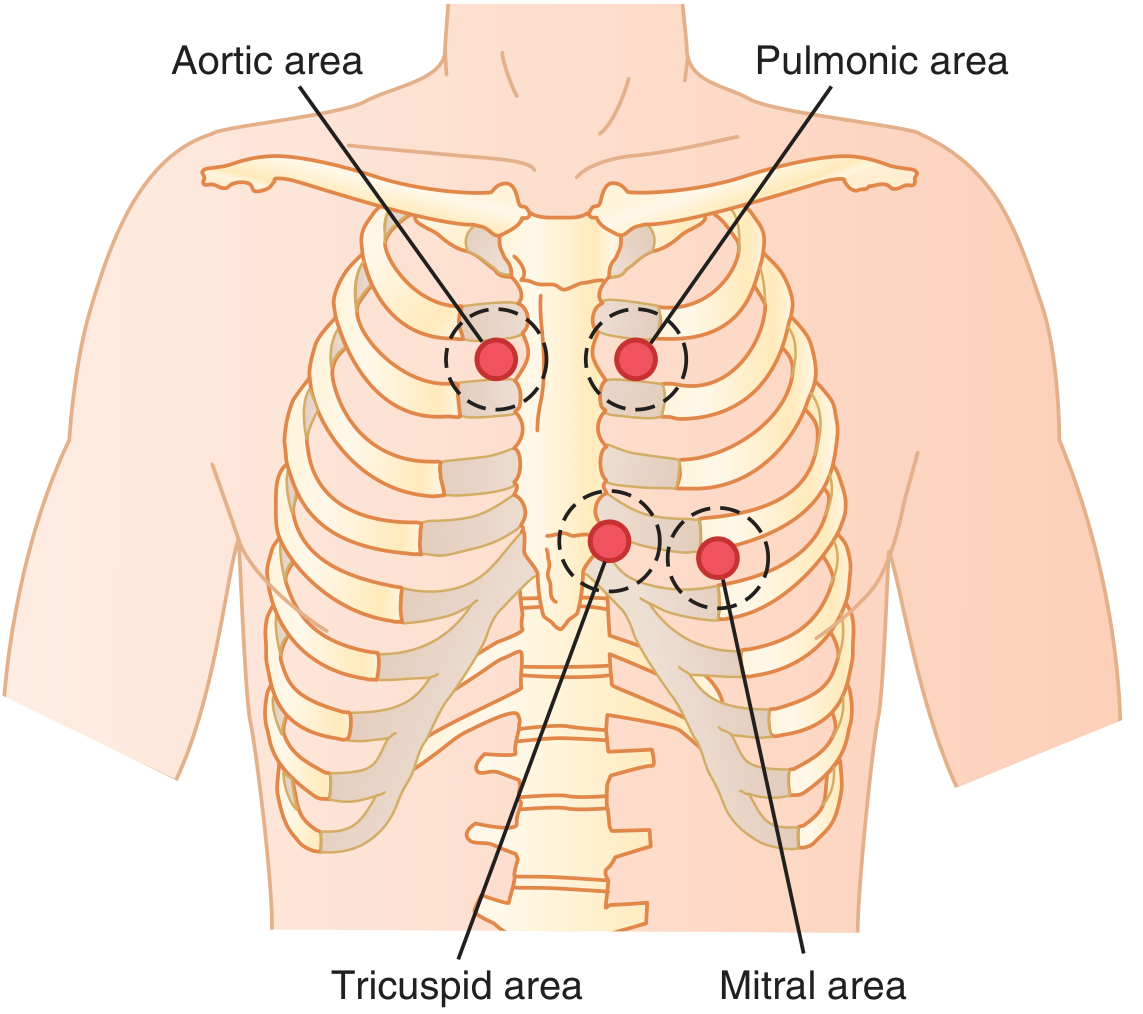
| Area | Location | Best For |
|---|---|---|
| Mitral (Apex) | 5th ICS, midclavicular line | S1, S3, S4, MR, MS |
| Tricuspid | 5th ICS, left parasternal | S1, TR |
| Pulmonary | 2nd ICS, left parasternal | P2, splitting of S2, PS |
| Aortic | 2nd ICS, right parasternal | A2, AS |
| Accessory Aortic (Erb's point) | 3rd ICS, left parasternal | AR |
Technique note: Use the diaphragm for high-pitched sounds (S1, S2, most murmurs); use the bell (light pressure) for low-pitched sounds (S3, S4, mitral diastolic rumble). Always auscultate in three positions: supine, sitting, and left lateral decubitus.
The Four Heart Sounds
S1 - First Heart Sound ("Lub")
- Timing: Beginning of systole (ventricular contraction)
- Cause: Closure of mitral (M1) and tricuspid (T1) valves; M1 precedes T1
- Best heard: Apex / left lower sternal border (LLSB)
- Quality: Low-pitched, longer (~0.14 sec), dull
- Normal splitting: M1-T1 split can be heard at LLSB - this is physiologic
Intensity changes of S1:
| Loud S1 | Soft S1 |
|---|---|
| Short PR interval (preexcitation, tachycardia) | Prolonged PR interval (1st degree AV block) |
| Pliable mitral stenosis | Calcified/immobile MS leaflets |
| Hyperdynamic states (fever, thyrotoxicosis) | Poor LV contractility / severe LV dysfunction |
| Thin chest wall | Obesity, emphysema, pericardial effusion |
| - | Atrial fibrillation (variable intensity) |
S2 - Second Heart Sound ("Dub")
- Timing: End of systole
- Cause: Closure of aortic (A2) and pulmonary (P2) valves
- Best heard: Left upper sternal border (LUSB)
- Quality: Higher-pitched, shorter (~0.11 sec) than S1 due to tauter semilunar valves
Physiologic (Normal) Splitting of S2
During inspiration: increased venous return → prolonged RV ejection → P2 delayed → A2-P2 gap widens (audible split)
During expiration: gap narrows → single S2
Types of Abnormal S2 Splitting
| Type | Character | Causes |
|---|---|---|
| Wide (persistent) splitting | Split heard in both inspiration and expiration; widens more on inspiration | RBBB, pulmonary stenosis, pulmonary hypertension (delayed P2); MR, VSD, early A2 closure |
| Fixed splitting | Wide split that does NOT change with respiration | ASD, PAPVR (equalised RV/LV preload changes) |
| Paradoxical (reversed) splitting | Split heard in expiration, disappears on inspiration | LBBB (delayed A2), severe AS, HOCM, WPW type B, RV pacing |
| Single S2 | No audible split | Pulmonary HTN (loud P2 merges), severe PS/AS (absent P2 or A2), TGA, TOF, pulmonary atresia, aortic atresia, truncus arteriosus |
P2 loudness clues:
- Loud P2 = pulmonary arterial hypertension (if heard at apex = severe PAH)
- Diminished/absent P2 = severe valvular PS, COPD/emphysema, TOF
- Loud A2 = systemic hypertension, syphilitic aortitis
- Diminished A2 = calcific aortic stenosis (important severity marker)
S3 - Third Heart Sound (Ventricular Gallop / "Ken-tuc-KY")
- Timing: Early diastole (beginning of middle third); follows S2 by ~0.12-0.16 sec
- Cause: Rapid ventricular filling phase - blood rebounding off ventricular walls
- Quality: Low-pitched, soft; heard with the bell at the apex in left lateral decubitus
- Rhythm: "S1 - S2 - S3" = "lub-dub-ta" = Protodiastolic gallop
| S3 - Physiologic (Normal) | S3 - Pathological |
|---|---|
| Children, adolescents, young adults (<40 yrs) | Adults >40 yrs |
| Athletes | LV systolic failure (dilated cardiomyopathy, CCF) |
| Pregnancy, high-output states | Large VSD, severe MR, severe AR |
| - | Right-sided S3 in RV failure (heard at LLSB, increases with inspiration) |
S4 - Fourth Heart Sound (Atrial Gallop / "TEN-nes-see")
- Timing: Late diastole (presystole); just before S1
- Cause: Forceful atrial contraction into a non-compliant (stiff) ventricle
- Quality: Low-pitched; heard with the bell at the apex (left lateral decubitus)
- Rhythm: "S4 - S1 - S2" = "ta-lub-dub" = Presystolic gallop
- S4 is ALWAYS pathological (never normal in adults)
- Absent in atrial fibrillation (no atrial contraction)
Causes of S4:
- LV hypertrophy (HTN, HCM, AS)
- Acute MI (stiff, ischemic ventricle)
- Diastolic dysfunction (Grade I)
- Restrictive cardiomyopathy
- Right-sided S4: RV hypertrophy, pulmonary hypertension, pulmonic stenosis
Summary Diagram - Added Heart Sounds
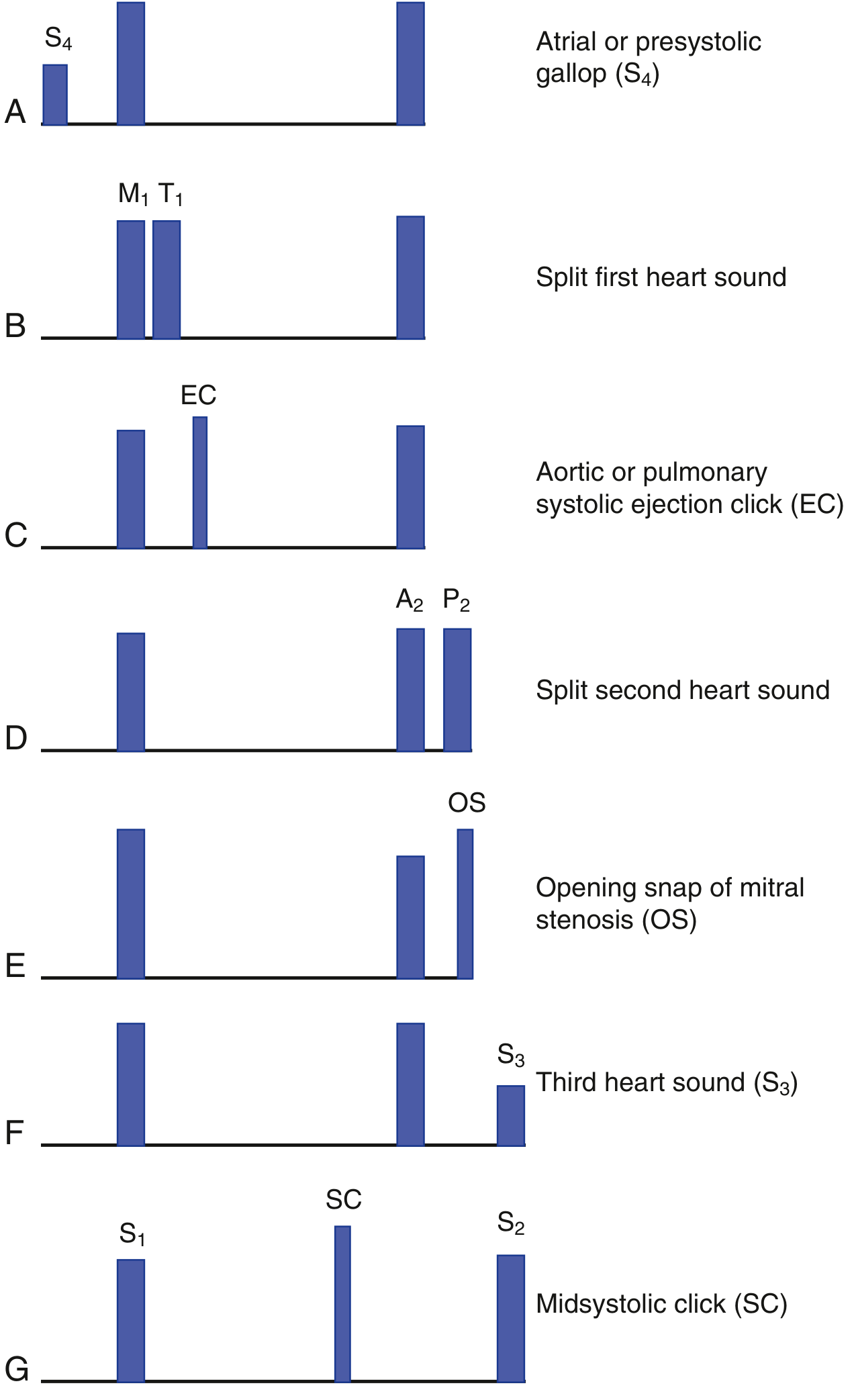
A = S4 atrial/presystolic gallop | B = Split S1 (M1-T1) | C = Ejection click (EC) | D = Split S2 (A2-P2) | E = Opening snap (OS) | F = S3 third heart sound | G = Midsystolic click (SC)
Additional Sounds
Ejection Clicks (Systolic)
- Occur just after S1 (early systole)
- High-pitched, best with diaphragm
- Causes: Stenosis or dilation of semilunar valves
- Aortic ejection click - aortic stenosis, bicuspid aortic valve, aortic root dilation (does NOT change with respiration)
- Pulmonary ejection click - pulmonary stenosis, pulmonary HTN, idiopathic PA dilation (DECREASES with inspiration - unique among right-sided sounds)
Midsystolic Click
- Mid-to-late systole
- Best heard at apex
- Cause: Mitral Valve Prolapse (MVP) - click moves earlier with standing/Valsalva (decreased preload), later with squatting (increased preload)
Opening Snap (OS) - Diastolic
- High-pitched snap just after S2 in early diastole
- Cause: Mitral stenosis (pliable, non-calcified leaflets snapping open)
- Also in tricuspid stenosis (rare)
- S2-OS interval: shorter interval = more severe MS (higher LA pressure)
- Absent when leaflets are calcified and immobile
Pericardial Knock
- Early diastolic sound (like loud S3)
- Cause: Constrictive pericarditis - abrupt cessation of ventricular filling by rigid pericardium
Tumor Plop
- Mid-diastolic sound
- Cause: Left atrial myxoma prolapsing through mitral valve; mimics OS but timing varies with position
Quick Memory Table
| Sound | Timing | Best Heard | Cause | Significance |
|---|---|---|---|---|
| S1 | Beginning systole | Apex | MV + TV closure | Normal |
| S2 | End systole | LUSB | AV + PV closure | Normal |
| S3 | Early diastole | Apex (bell) | Rapid filling / volume overload | Physiologic in young; CCF in old |
| S4 | Late diastole (pre-S1) | Apex (bell) | Forceful atrial contraction | Always pathologic; not in AF |
| EC | Early systole | LUSB/Apex | Semilunar valve disease | AS, PS, MVP |
| Midsystolic click | Mid systole | Apex | MVP | Varies with preload |
| OS | Early diastole | Apex/LLSB | MS (pliable leaflets) | Rheumatic MS |
| Pericardial knock | Early diastole | LLSB | Constrictive pericarditis | Loud early diastolic sound |
Grading of Heart Murmurs (Levine Scale)
| Grade | Description |
|---|---|
| I | Barely audible (very experienced examiner, quiet room) |
| II | Soft but readily heard |
| III | Moderately loud; NOT associated with thrill |
| IV | Loud; associated with palpable thrill |
| V | Very loud; audible with stethoscope barely touching chest |
| VI | Audible with stethoscope off the chest |
Grades I-II: soft murmurs | Grades IV-VI: always associated with thrill (from Grade IV onwards)
- Guyton & Hall Textbook of Medical Physiology, p.289 | Fuster & Hurst's The Heart 15th Ed., pp.88-92 | Harrison's Principles of Internal Medicine 22E | Harriet Lane Handbook 23rd Ed., pp.223-224 | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.