Pseudomonas infection 2nd yr mbbs microbiology refer apurba sastri cover definition clinical manifestation pathogenesis virulance factor symptoms suppurative complications, non suppurative complications, lab diagnosis treatment answer in details
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have rich, comprehensive content. Let me compile the complete answer aligned to Apurba Sastri's 2nd year MBBS microbiology format.
Pseudomonas Infection - Comprehensive Notes (2nd Year MBBS Microbiology)
Based on Medical Microbiology 9e & Sherris & Ryan's Medical Microbiology, aligned with Apurba Sastri's approach
Definition
Pseudomonas aeruginosa is a motile, non-sporing, non-capsulated (except mucoid strains), aerobic, Gram-negative rod belonging to the family Pseudomonadaceae. It is the most clinically significant species of the genus Pseudomonas, and acts primarily as an opportunistic pathogen - causing infections mainly in immunocompromised, hospitalized, or debilitated patients.
- Name derivation: "pseudes" (false) + "monas" (a unit) - refers to how pairs of cells resemble a single cell on Gram stain
- "aeruginosa" - full of copper rust or green (refers to blue + yellow pigments that appear green)
Morphology and General Properties
| Feature | Description |
|---|---|
| Shape | Straight or slightly curved Gram-negative rod, 0.5-1.0 × 1.5-5.0 µm |
| Arrangement | Single or in pairs |
| Motility | Motile by a single polar flagellum |
| Capsule | Mucoid polysaccharide (alginate) capsule in some strains |
| Spore | Non-sporing |
| Aerobe | Obligate aerobe (can grow anaerobically with nitrate as electron acceptor) |
| Oxidase | Positive (cytochrome oxidase present) |
| Temperature range | 20-42°C (can grow at 42°C - key identifying feature) |
| Genome | One of the largest bacterial genomes: 5,567 genes including 468 regulatory genes |
Epidemiology / Habitat
- Environmental reservoir: Soil, water, decaying organic matter, vegetation - ubiquitous in nature
- Hospital reservoirs (moist): Sinks, toilets, floor mops, cut flowers, food, humidifiers, ventilator circuits, dialysis equipment, respiratory therapy equipment, contact lens solutions, even some disinfectants
- Colonization rate: 2-10% of throat/stool in healthy persons; much higher in hospitalized patients
- High-risk groups:
- Neutropenic/immunocompromised patients
- Cystic fibrosis (CF) patients
- Extensive burn patients
- Patients on broad-spectrum antibiotics
- Hematologic malignancy patients
- Diabetics (especially malignant otitis externa)
- IV drug abusers (endocarditis)
Virulence Factors
Pseudomonas has one of the most elaborate arrays of virulence factors among bacteria. Multiple factors must work together to cause disease.
1. Adhesins (Surface Structures)
| Factor | Role |
|---|---|
| Flagella | Motility + adherence to epithelial cells |
| Pili (fimbriae) | Attachment to sialic acid and N-acetylglucosamine receptors on host cells |
| Lipopolysaccharide (LPS) | Endotoxin activity via Lipid A component; also mediates adherence |
| Alginate (mucoid capsule) | Polysaccharide (D-mannuronic + L-guluronic acids); protects from phagocytosis and antibiotic killing; forms biofilm; critical in CF patients |
2. Secreted Toxins and Enzymes
| Factor | Mechanism | Effect |
|---|---|---|
| Exotoxin A (ETA) | ADP-ribosylation of elongation factor 2 (EF-2) - same mechanism as diphtheria toxin but structurally different and less potent | Arrests protein synthesis → cell death; causes dermatonecrosis in burns, corneal damage, lung tissue destruction |
| Pyocyanin (blue pigment) | Catalyzes superoxide and H₂O₂ production; stimulates IL-8 release | Toxic to host cells; toxic effect on respiratory ciliary function; attracts neutrophils |
| Pyoverdin (yellow-green siderophore) | Binds iron for bacterial metabolism | Also regulates secretion of ETA and other virulence factors |
| Elastases (LasA + LasB) | LasA = serine protease; LasB = zinc metalloprotease; act synergistically | Degrade elastin → hemorrhagic lesions (ecthyma gangrenosum), lung parenchymal damage; degrade IgA, IgG, complement components; inhibit neutrophil chemotaxis |
| Alkaline protease | Tissue destruction | Spread of infection; interferes with host immune response |
| Phospholipase C (heat-labile hemolysin) | Breaks down lipids and lecithin | Tissue destruction; hemolysis |
| Exoenzymes S (ExoS) and T (ExoT) | Injected via Type III secretion system (T3SS) into host cells; disrupt actin cytoskeleton | Epithelial cell damage, bacterial spread, tissue invasion, necrosis; ExoS associated with dissemination from burn wounds |
| ExoU | Phospholipase activity; injected by T3SS | Cytotoxin; more virulent minority of strains |
3. Type III Secretion System (T3SS)
- A molecular "syringe" that directly injects effector proteins (ExoS, ExoT, ExoU) into host cells
- Bypasses extracellular immune defenses
- Expressed by the vast majority of P. aeruginosa strains
- Associated with more severe, invasive disease
4. Antibiotic Resistance
- Intrinsic resistance: Outer membrane porins are relatively impermeable (unlike Enterobacteriaceae), limiting antibiotic entry
- Acquired resistance: Horizontal gene transfer of resistance genes
- Adaptive resistance: Upregulation of efflux pumps; biofilm formation
- Resistant to most penicillins, cephalosporins (except certain anti-pseudomonal ones), and many other classes
Pathogenesis
Infection requires:
- A break in first-line defenses (e.g., wound, burn) or a bypass (contaminated IV line, endotracheal tube)
- A compromised host (immunosuppression, neutropenia)
Steps in pathogenesis:
-
Colonization/Attachment: Pili, flagella, and alginate slime mediate adherence to epithelial cells via sialic acid and N-acetylglucosamine receptors. Attachment is favored by loss of surface fibronectin (which normally blocks binding) - explains why debilitated patients are predisposed.
-
Local tissue invasion: Exotoxin A, elastases, phospholipase C, and alkaline protease degrade host proteins, lipids, and extracellular matrix. This allows acquisition of nutrients and local spread.
-
Systemic spread: Elastase and ExoS mediate destruction of blood vessel walls (histological hallmark: hemorrhagic vascular destruction). Organisms enter the bloodstream → bacteremia.
-
Toxin-mediated damage:
- ExoA shuts down protein synthesis in host cells
- ExoS/T injected into cells cause cytoskeletal disruption and apoptosis
- Pyocyanin impairs mucociliary clearance
- Elastase destroys elastin in lungs and blood vessels
-
Biofilm formation (especially in CF): Mucoid mutants overproduce alginate, forming a thick biofilm that is essentially impossible to eradicate with antibiotics.
Clinical Manifestations / Symptoms
A. Respiratory Tract Infections
- Pneumonia: Particularly in ventilated patients (VAP - Ventilator-Associated Pneumonia); also in CF patients
- In CF: chronic colonization → mucoid biofilm formation → progressive pulmonary destruction → leading cause of morbidity and death in CF
- Presents with fever, productive cough, purulent/green sputum, dyspnea, chest pain
B. Urinary Tract Infections (UTI)
- Typically nosocomial, associated with catheterization or urological procedures
- Complicated UTI, often with antibiotic-resistant strains
C. Skin and Soft Tissue Infections
- Burn wound infections: Most feared complication of burns; can progress to bacteremia and sepsis
- Ecthyma gangrenosum: Pathognomonic skin lesion of Pseudomonas bacteremia - starts as erythematous papule/vesicle → becomes hemorrhagic → black necrotic ulcer; due to direct vascular invasion by organism
- Folliculitis: "Hot tub folliculitis" - pruritic erythematous papules/pustules after exposure to contaminated water; self-limiting
- Wound infections: Post-surgical, post-traumatic
D. Ear Infections
- Otitis externa ("swimmer's ear"): Common, localized, managed with topical antibiotics
- Malignant (necrotizing) otitis externa: Seen in diabetics and elderly; invades underlying tissues and bone (osteomyelitis of temporal bone); damages cranial nerves (especially VII); life-threatening; requires aggressive IV antibiotics ± surgery
E. Eye Infections
- Keratitis: Usually following corneal trauma (contact lens abrasion) + contaminated solutions; can destroy cornea within 24-48 hours
- Conjunctivitis, endophthalmitis (post-trauma or surgery)
F. Bacteremia and Septicemia
- Most common sources: lower respiratory tract, UTI, skin/soft tissue (especially burn wounds)
- Clinically indistinguishable from other Gram-negative bacteremia initially
- Higher mortality than most Gram-negative bacteremias due to: immunocompromised host, antibiotic resistance, inherent virulence
- May present with ecthyma gangrenosum (pathognomonic)
G. Endocarditis
- Rare; primarily in IV drug abusers (contaminated needles/paraphernalia)
- Tricuspid valve most commonly involved
- Chronic course; better prognosis than left-sided valve involvement
H. Other Infections
- Meningitis/CNS: Post-neurosurgical procedures
- Osteomyelitis: Especially in IV drug abusers and diabetic foot
- Gastrointestinal infections: Rare; necrotizing enterocolitis in neonates
- Septic arthritis
Suppurative Complications
These arise from direct bacterial invasion and tissue destruction:
- Lung abscess / empyema - from severe pneumonia
- Bacteremia / septicemia - spread from primary focus
- Septic shock - from overwhelming bacteremia (endotoxin-mediated)
- Ecthyma gangrenosum - vascular invasion causing skin necrosis
- Endophthalmitis - from keratitis progression (can lead to blindness)
- Malignant otitis externa with osteomyelitis - bone destruction
- Osteomyelitis and septic arthritis - from hematogenous seeding or direct inoculation
- Endocarditis - especially tricuspid valve in IV drug users
- Meningitis / brain abscess - from neurosurgical or hematogenous spread
- Multi-organ failure - from uncontrolled sepsis
Non-Suppurative Complications
These arise from immune/inflammatory reactions rather than direct pus formation:
- Immune complex deposition: In chronic Pseudomonas infection (especially in CF lungs), antibodies form against LasA and LasB elastases → immune complexes deposit in infected tissues → chronic inflammation and tissue injury
- Reactive arthritis: Rare, following Pseudomonas bacteremia
- Chronic pulmonary destruction in CF: Progressive fibrosis and bronchiectasis driven partly by immune-mediated inflammation against persistent Pseudomonas antigens
- Systemic inflammatory response syndrome (SIRS): Cytokine storm from LPS (endotoxin) triggering TNF-α, IL-1, IL-6 cascade
Laboratory Diagnosis
1. Specimen Collection
- Based on site of infection: sputum, BAL, wound swab, urine (midstream or catheter), blood (for bacteremia), CSF, eye swab, ear swab
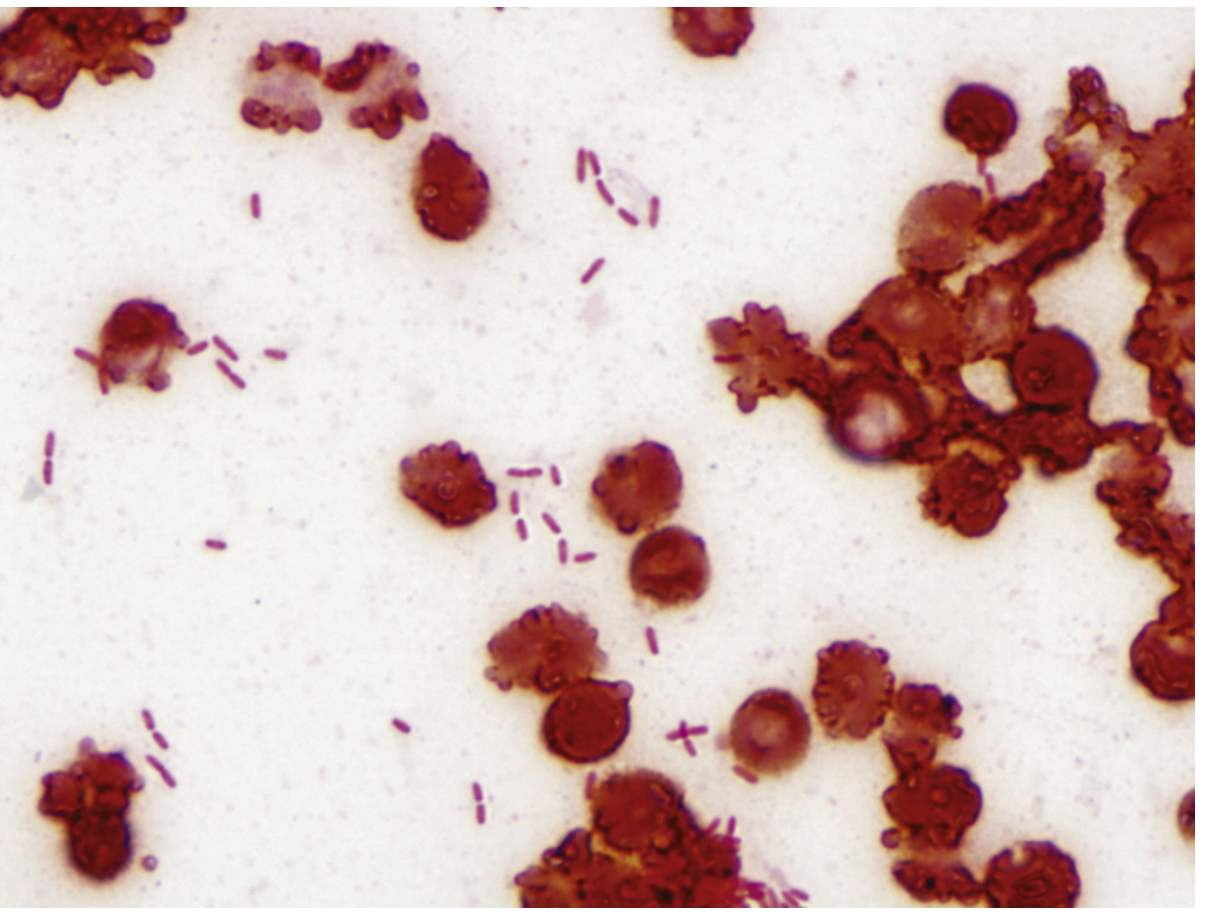
2. Direct Microscopy (Gram Stain)
- Gram-negative rods, arranged singly or in pairs
- Mucoid capsule may be visible in CF patients (slime around organisms)
- Pus cells (neutrophils) in most infections
3. Culture
Media used:
- Grows on all common media: Blood agar, MacConkey agar, nutrient agar
- Selective media: Cetrimide agar (contains cetrimide as selective agent - inhibits other organisms)
Colonial characteristics:
- Blood agar: Large, spreading, β-hemolytic colonies; metallic sheen; fringed/irregular edges; characteristic fruity/grape-like odor (due to aminoacetophenone)
- MacConkey agar: Non-lactose fermenting (pale/colorless) colonies
- Pigments: Produces diffusible pigments that color the medium
- Pyocyanin (blue) - produced ONLY by P. aeruginosa
- Pyoverdin/fluorescein (yellow-green, fluorescent under UV)
- Together they produce a characteristic blue-green color on plates
- Other pigments: pyorubin (reddish-brown), pyomelanin (brown-black)
4. Biochemical Identification
| Test | Result |
|---|---|
| Oxidase test | Positive (key differentiator from Enterobacteriaceae) |
| Catalase | Positive |
| Indole | Negative |
| Citrate | Positive |
| Urease | Variable |
| Nitrate reduction | Positive |
| Glucose fermentation | Oxidative (not fermentative) |
| Growth at 42°C | Positive (distinguishes from other Pseudomonas species) |
| Lactose fermentation | Negative (non-fermenter) |
5. Antibiotic Sensitivity Testing
- Essential due to multiple resistance patterns
- Methods: Kirby-Bauer disc diffusion, MIC determination (broth microdilution)
- Test against: piperacillin-tazobactam, ceftazidime, cefepime, carbapenems (imipenem/meropenem), aminoglycosides (amikacin/gentamicin/tobramycin), fluoroquinolones (ciprofloxacin), colistin
6. Serology
- Not routinely used for diagnosis
- Anti-elastase (anti-LasA, anti-LasB) antibodies may be detected in chronic CF infections
- Useful for monitoring chronic pulmonary infection in CF patients
Treatment
General Principles
- Pseudomonas is intrinsically resistant to many antibiotics (due to restricted outer membrane permeability, efflux pumps)
- Monotherapy is generally ineffective and can rapidly select resistant mutants
- Combination therapy (aminoglycoside + anti-pseudomonal β-lactam) is the standard approach for serious infections
Drug Classes Active Against Pseudomonas
| Class | Drug(s) |
|---|---|
| Anti-pseudomonal penicillins | Piperacillin-tazobactam, ticarcillin-clavulanate |
| Anti-pseudomonal cephalosporins | Ceftazidime, cefepime |
| Carbapenems | Imipenem, meropenem (NOT ertapenem) |
| Monobactams | Aztreonam |
| Aminoglycosides | Gentamicin, tobramycin, amikacin |
| Fluoroquinolones | Ciprofloxacin (most active), levofloxacin |
| Polymyxins | Colistin (polymyxin E) - last resort for MDR strains |
Recommended Regimens by Infection Type
| Infection | Preferred Regimen |
|---|---|
| Bacteremia/Severe infection | Anti-pseudomonal β-lactam + aminoglycoside (combination) |
| Pneumonia/VAP | Piperacillin-tazobactam or cefepime or meropenem ± aminoglycoside |
| UTI (uncomplicated) | Ciprofloxacin oral |
| Burn wound infection | Topical: silver sulfadiazine; systemic if invasive |
| Malignant otitis externa | IV ceftazidime or ciprofloxacin; prolonged course 6-8 weeks |
| Keratitis | Topical ciprofloxacin or tobramycin eye drops (intensive) |
| CF exacerbation | Tobramycin (inhaled) + IV anti-pseudomonal β-lactam |
| MDR/XDR strains | Colistin ± rifampicin or fosfomycin |
Why Monotherapy Fails
- Intrinsic resistance: restricted porin permeability blocks antibiotic entry
- Efflux pumps (MexAB-OprM, MexXY-OprM) actively export antibiotics
- β-lactamase production (AmpC, OXA, MBL types)
- Biofilm formation reduces antibiotic penetration by 100-1000x
Prevention and Control
- Strict infection-control measures in hospitals: prevent contamination of sterile equipment
- Avoid unnecessary broad-spectrum antibiotic use (prevents selection of resistant strains)
- Adequate hand hygiene, sterilization of respiratory therapy equipment
- Maintain sterility of IV lines, urinary catheters
- For CF: inhaled tobramycin (TOBI) prophylaxis to slow respiratory deterioration
Summary Table (Quick Recall for Exams)
| Feature | Key Point |
|---|---|
| Type | Gram-negative, non-fermenting rod, opportunistic pathogen |
| Key pigment | Pyocyanin (blue) - ONLY P. aeruginosa |
| Key test | Oxidase +ve; grows at 42°C |
| Selective media | Cetrimide agar |
| Key toxin | Exotoxin A (same mechanism as diphtheria toxin - ADP ribosylation of EF-2) |
| Unique skin lesion | Ecthyma gangrenosum (bacteremia) |
| Key complication in CF | Chronic mucoid colonization → irreversible lung destruction |
| Key complication in diabetics | Malignant otitis externa |
| Key complication in IV drug users | Tricuspid valve endocarditis |
| Treatment rule | Never monotherapy - always combination |
| Last resort drug | Colistin (for MDR strains) |
Sources: Medical Microbiology 9e (Murray et al.), Sherris & Ryan's Medical Microbiology 8th Edition - content aligned with Apurba Sastri Microbiology syllabus for 2nd year MBBS.
This is a shared conversation. Sign in to Orris to start your own chat.