Cvc liver explanation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Chronic Venous Congestion (CVC) of the Liver
CVC liver (also called passive congestion of the liver or congestive hepatopathy) is a condition caused by impaired venous outflow from the liver, most commonly due to right-sided heart failure. Blood backs up through the inferior vena cava into the hepatic veins and hepatic sinusoids, causing characteristic structural changes.
Cause
- Right-sided cardiac failure - the #1 cause. Elevated right-heart pressure is transmitted backward via the IVC into the hepatic veins.
- Other causes of outflow obstruction: constrictive pericarditis, tricuspid regurgitation, Budd-Chiari syndrome.
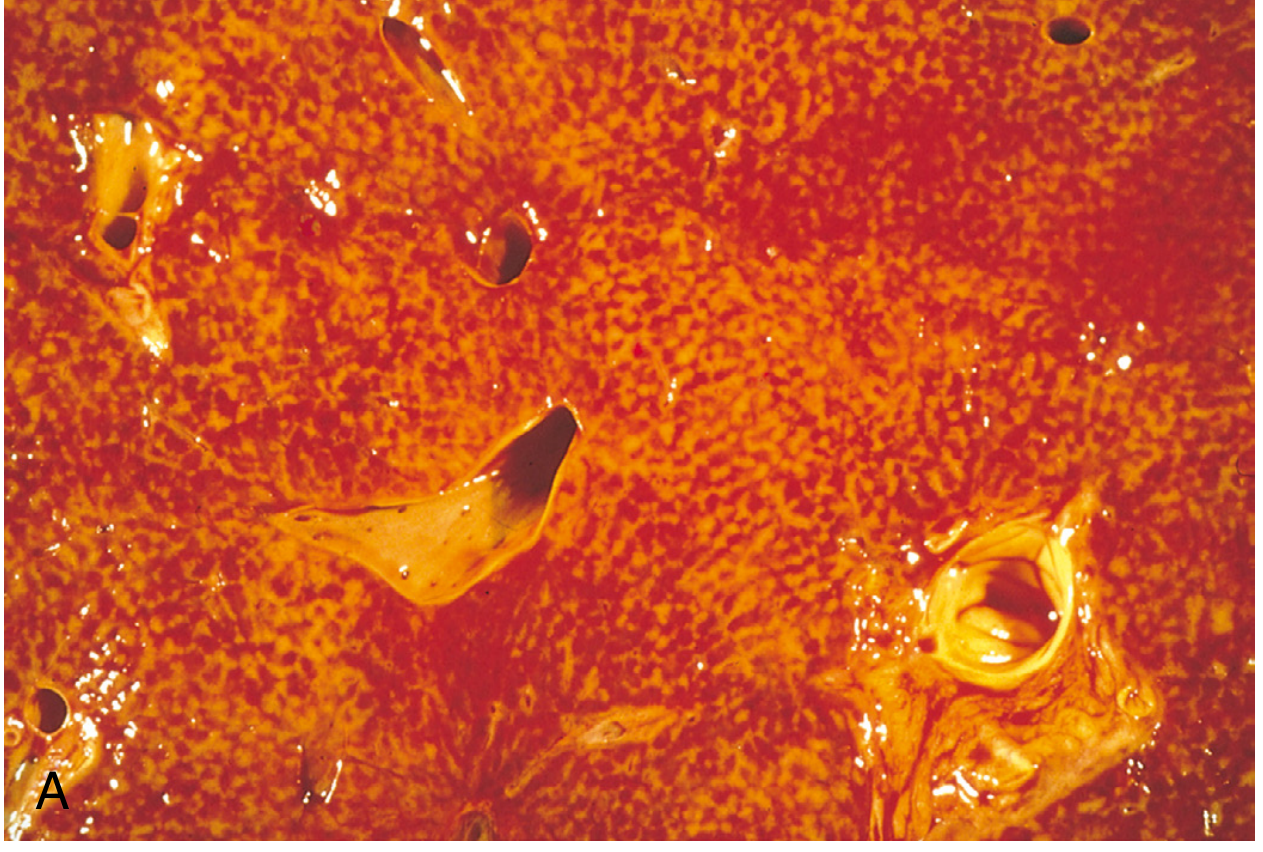
Gross Pathology - "Nutmeg Liver"
The cut surface of the liver shows a variegated, mottled red-and-tan appearance, resembling the cut surface of a nutmeg:
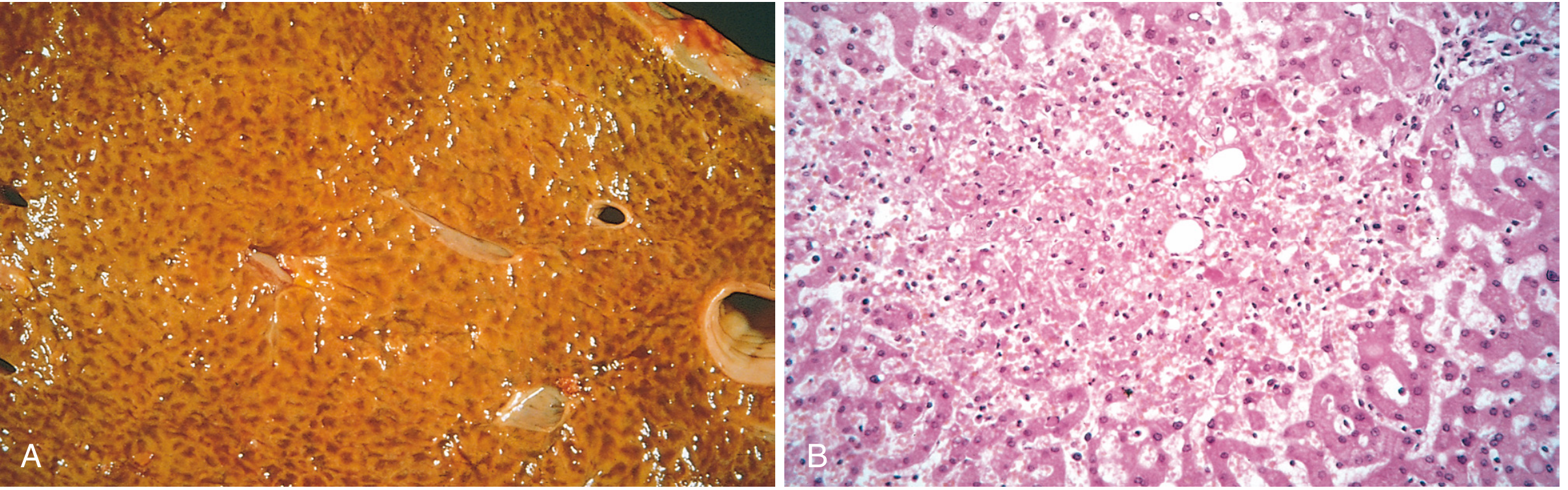
- Red-brown areas = congested, hemorrhagic centrilobular (zone 3) regions
- Tan/pale areas = relatively preserved periportal (zone 1) hepatocytes
The liver is slightly enlarged, tense, and cyanotic with rounded edges.
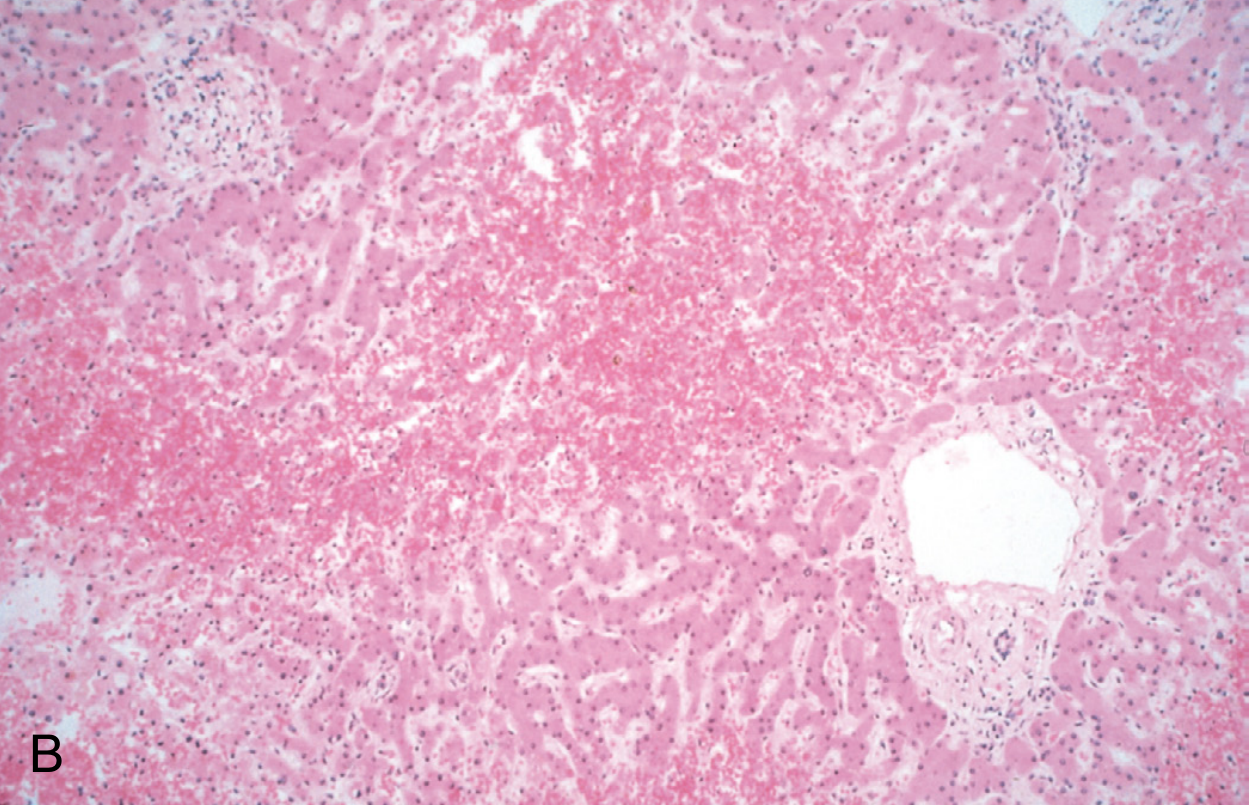
Microscopic Features
| Feature | Details |
|---|---|
| Zone affected | Zone 3 (centrilobular) - farthest from portal blood supply, most oxygen-deprived |
| Early | Dilated centrilobular sinusoids packed with red cells |
| Progressive | Centrilobular hepatocyte atrophy - attenuated hepatocyte plates |
| With left heart failure / shock added | Centrilobular hemorrhagic necrosis - combination of congestion + hypoperfusion |
| Chronic severe | Cardiac sclerosis - centrilobular pericellular fibrosis, sometimes bridging septa |
A sharp demarcation exists between:
- Viable periportal hepatocytes (zone 1)
- Necrotic/atrophic pericentral hepatocytes (zone 3)
Pathophysiology Summary
Right heart failure
↓
↑ Central venous pressure
↓
IVC → Hepatic veins → Sinusoidal congestion
↓
Zone 3 (centrilobular) hypoxia + congestion
↓
Hepatocyte atrophy / necrosis
↓
If chronic → Cardiac cirrhosis (cardiac sclerosis)
The centrilobular zone is most vulnerable because:
- It is farthest from the oxygenated portal blood supply
- It receives blood last in the hepatic lobule
- Retrograde venous pressure hits it first
Clinical Features
- Often asymptomatic or mild hepatomegaly with right upper quadrant discomfort
- Transient elevation of serum aminotransferases (ALT/AST) is the most common lab finding
- Mild to moderate jaundice if necrosis is significant
- In severe/chronic cases: signs of portal hypertension (ascites, varices) may develop
Key Terminology
| Term | Meaning |
|---|---|
| Nutmeg liver | Gross appearance - mottled red-tan pattern on cut surface |
| Cardiac sclerosis | Fibrosis around central veins in chronic CVC |
| Cardiac cirrhosis | Rare end-stage - true cirrhosis from chronic congestion |
| Centrilobular necrosis | Microscopic hallmark - zone 3 hepatocyte death |
Source: Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.