Kyphosis
Reading File
Finding Sources
Searching the Web
kyphosis types causes treatment clinical overview
Reading File
Reading File
Reading File
Reading File
Searching PubMed
kyphosis classification management
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks along with high-quality images. Here is the full answer:
Kyphosis
Kyphosis refers to an excessive forward (posterior convex) curvature of the vertebral column. The normal thoracic kyphosis measures 20-50° on a lateral radiograph; angles beyond this range are considered pathological. - Gray's Anatomy for Students
Normal Spinal Curvatures
The thoracic spine normally has a mild kyphotic curve. When this exceeds 50°, it becomes clinically significant. A sharp, angular kyphosis (gibbus deformity) is characteristic of vertebral collapse, classically from tuberculosis affecting a thoracic body. - Gray's Anatomy for Students
Classification / Types
1. Postural Kyphosis (Round Back)
- Most common type
- No structural vertebral body changes on imaging
- No sharp angulation
- Corrects with backward bending and prone hyperextension - distinguishing feature
- Treatment: hyperextension exercise program
- Miller's Review of Orthopaedics, 9th Ed
2. Scheuermann's Disease (Structural Kyphosis)
The most important structural cause of adolescent kyphosis.
Diagnostic criteria (radiological):
- Increased thoracic kyphosis >45°
- Anterior vertebral wedging of ≥5° at three consecutive vertebrae
- Disc space narrowing and end-plate irregularities
- Schmorl nodes (disc herniation through end-plates)
- Associated spondylolysis in 30-50% of cases
- Associated scoliosis in 33% of cases
Clinical features:
- More common in boys
- Affected patients are often overweight
- Kyphosis is not postural - it does NOT fully correct with hyperextension (key distinguishing point from postural kyphosis)
- Neurologic changes are rare; MRI indicated if present
- Aetiology is unknown

Treatment of Scheuermann's Disease:
| Severity | Indication | Management |
|---|---|---|
| 50-75° | Skeletally immature (Risser ≤2), progressive curve | Bracing - modified Milwaukee brace (often poorly tolerated) |
| >75° or failed PT | Severe or progressive curve with continued pain | Surgery - posterior fusion with multilevel osteotomies |
- Surgical fusion to the first lordotic disc and the vertebra touched by the posterior sacral vertical line
- Brace treatment improves deformity in ~63% of patients who comply regularly - Bailey & Love's Surgery, 28th Ed
3. Congenital Kyphosis
Uncommon but significant because neurologic deficits are frequent.
Cause: Abnormal embryological development - failure of vertebral body formation or segmentation.
Winter Classification:
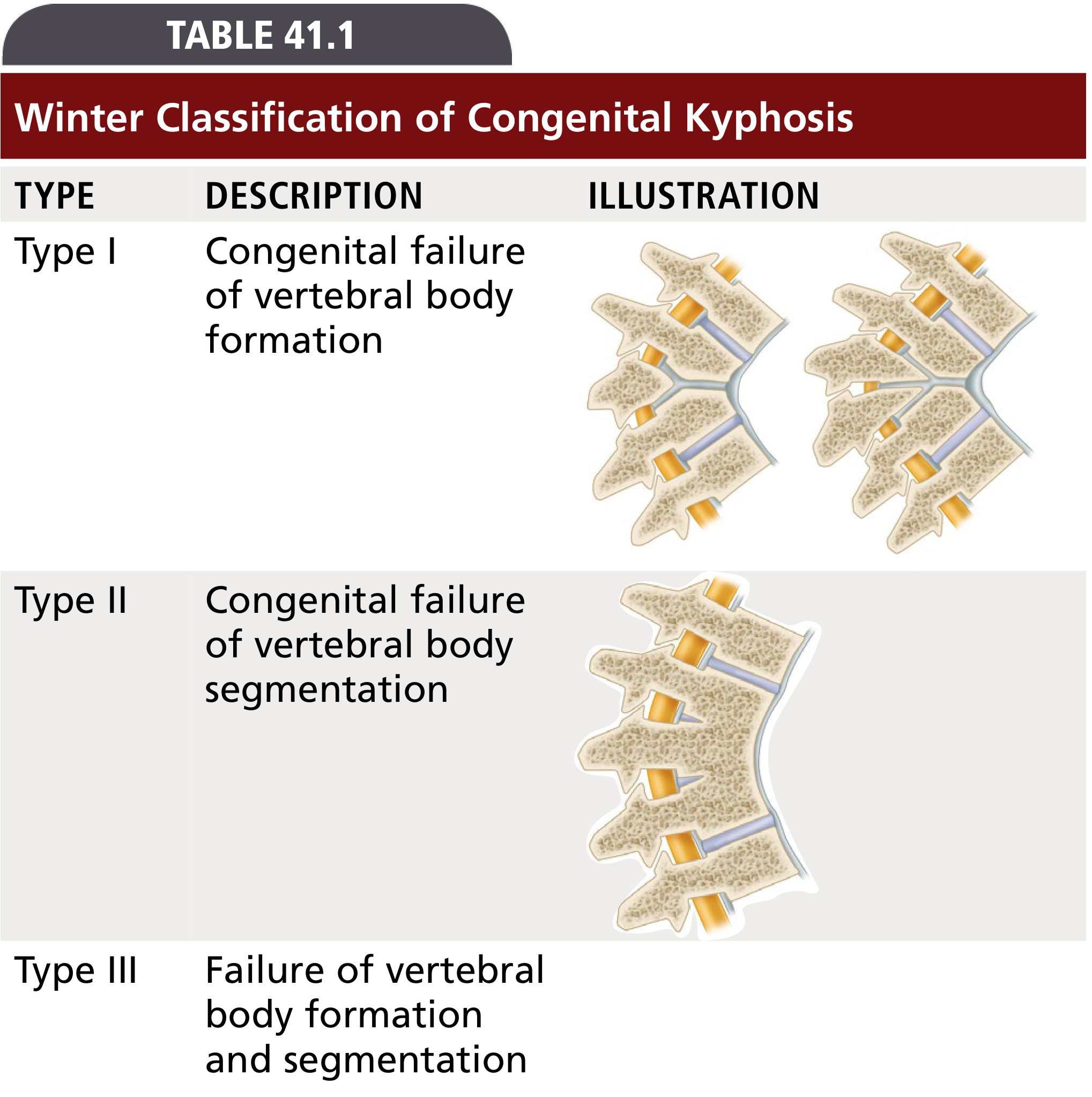
| Type | Description | Prognosis |
|---|---|---|
| Type I | Failure of vertebral body formation (hemivertebrae, wedged vertebrae) | Most severe progression; highest risk of paraplegia |
| Type II | Failure of vertebral body segmentation (anterior unsegmented bar) | Slower progression |
| Type III | Mixed - failure of both formation and segmentation | Variable |
- Deformity usually progresses with growth; severity proportional to number of vertebrae involved and growth remaining
- Type I is subdivided further into: posterolateral quadrant vertebrae, posterior hemivertebrae, butterfly vertebrae, and anterolateral wedged vertebrae
- Campbell's Operative Orthopaedics, 15th Ed 2026
4. Other Causes of Kyphosis
| Cause | Notes |
|---|---|
| Trauma | Vertebral compression/burst fractures causing kyphotic deformity |
| Infection | TB (gibbus deformity), pyogenic spondylodiscitis |
| Osteoporosis | Age-related vertebral compression fractures (most common in elderly) |
| Bone dysplasias | Mucopolysaccharidoses, Kniest syndrome, diastrophic dysplasia |
| Neoplasms | Pathological fracture leading to kyphosis |
| Postlaminectomy | Especially in skeletally immature patients; total laminectomy without stabilization is contraindicated in growing children - may require anterior + posterior fusion |
- Miller's Review of Orthopaedics, 9th Ed
Gibbus Deformity
A sharp, angulated kyphosis at a single level - classically from tuberculous spondylitis (Pott's disease) destroying a vertebral body. This was prevalent before antituberculous medication became available. - Gray's Anatomy for Students
Evaluation
- Lateral standing radiograph - measure Cobb angle (T1-T12 or from apex)
- Adams forward bend test - assesses for rotational component; may show rib hump (see scoliosis differentiation)
- MRI - indicated for neurological symptoms, congenital kyphosis (rule out intraspinal anomalies), or atypical features
- Normal thoracic kyphosis: 20-50°; Scheuermann defined as >45° with structural wedging
Summary
| Type | Age | Structural | Correctible | Treatment |
|---|---|---|---|---|
| Postural | Adolescent | No | Yes (hyperextension) | Exercises |
| Scheuermann | Adolescent | Yes | No | Brace/Surgery |
| Congenital | Any | Yes | No | Surgery (often early) |
| Osteoporotic | Elderly | Yes | No | Medical + bracing |
| Post-traumatic | Any | Yes | Partial | Surgery/conservative |
Sources: Bailey & Love's Short Practice of Surgery 28th Ed | Miller's Review of Orthopaedics 9th Ed | Campbell's Operative Orthopaedics 15th Ed 2026 | Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.