I am a BPT student
Welcome! Happy to help a BPT (Bachelor of Physiotherapy) student.
What would you like to study or get help with today? You can ask about:
- Anatomy & Physiology - muscles, joints, nerves, organ systems
- Pathology & Conditions - neurological, musculoskeletal, cardiopulmonary disorders
- Assessment & Examination - special tests, outcome measures, manual muscle testing
- Physiotherapy Techniques - electrotherapy, manual therapy, exercise therapy, hydrotherapy
- Pharmacology - drugs relevant to rehab and pain management
- Clinical Cases - case-based learning and reasoning
- Exam Prep - MCQs, revision notes, key concepts
Just ask your question and I'll get you a thorough, textbook-backed answer!
My final exams are going on
Good luck with your finals! 💪
What subject or topic do you need help with? Tell me what's on your exam and I'll help you revise it clearly and thoroughly.
For example:
- "Explain stroke rehabilitation"
- "What are the special tests for shoulder?"
- "Describe TENS and its parameters"
- "What is Parkinson's disease PT management?"
Just ask - I'm ready!
Due to long sitting hours on the chair, I started having pain over my middle traps around at the origin site near the spine
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Here's a thorough breakdown of what's happening and what you can do about it:
Why Your Middle Trapezius Hurts at the Spine
Anatomy (as a BPT student, you'll appreciate this)
The trapezius is a large, flat, triangular muscle. Its origin runs along the entire vertebral column - from the external occipital protuberance and ligamentum nuchae all the way down to the spinous processes of C7 to T12.
The middle trapezius fibers originate from roughly T2-T5 spinous processes and insert into the spine of the scapula. Their primary action is scapular retraction (adduction).
| Part | Origin | Insertion | Action |
|---|---|---|---|
| Upper | Occiput, ligamentum nuchae, C7 spine | Lateral 1/3 clavicle, acromion | Elevates scapula |
| Middle | T1-T5 spinous processes | Spine of scapula | Retracts (adducts) scapula |
| Lower | T6-T12 spinous processes | Medial scapular spine | Depresses + upwardly rotates scapula |
Source: Gray's Anatomy for Students
Why Prolonged Sitting Causes This Pain
When you sit for hours - especially hunched forward studying:
- Rounded shoulders / forward head posture - your scapulae protract (move forward), stretching the middle trapezius into a lengthened, weakened position
- The muscle is held in sustained static tension at its origin - the spinous processes - for hours
- This leads to ischemic fatigue - reduced blood flow, lactic acid buildup, and micro-trauma at the musculotendinous/origin attachments
- The result: dull, aching pain right along the spine in the mid-thoracic region, exactly where you feel it
- Over time, myofascial trigger points can develop in the middle trapezius - often referencing pain toward the neck or shoulder blade
The accessory nerve (CN XI) supplies motor function to the trapezius, while proprioception runs through C3-C4 cervical plexus branches.
What You Should Do
Immediate Relief
- Heat therapy - a warm pack on the mid-thoracic spine relaxes the muscle and improves local circulation (15-20 min)
- Gentle self-massage - use a tennis ball against a wall at the origin points along the spine
- Postural correction - sit with a lumbar roll, shoulders back, ears over shoulders
Stretches (do every 30-45 minutes of study)
- Chest opener stretch - clasp hands behind back, squeeze shoulder blades together and gently extend - holds the middle trap in its shortened position to relieve the stretch fatigue
- Thoracic extension over chair back - gently extend your thoracic spine over the backrest of your chair
- Cross-body shoulder stretch - brings the scapula into protraction to temporarily relieve the chronically retracted/over-stretched origin
Strengthening (for long-term prevention)
Since the middle trapezius is being chronically overstretched and weakened, it needs strengthening:
- Prone Y/T/W exercises - lying prone, lift arms in Y, T, and W shapes - directly targets all parts of trapezius
- Scapular retraction exercises - squeeze shoulder blades together with resistance band
- Rows - seated or standing resistance band rows
Ergonomics (most important fix)
- Raise your screen to eye level
- Keep elbows at 90 degrees
- Take a postural break every 30 minutes - stand, walk briefly, do 10 scapular retractions
- Avoid holding your phone below eye level for long periods
As a BPT Student - Key Takeaway
This is a perfect real-world example of postural syndrome / upper crossed syndrome (Janda) - where:
- Tight/overactive: upper trapezius, pectorals, SCM
- Weak/inhibited: middle & lower trapezius, deep neck flexors, serratus anterior
Your pain at the origin site near the spine is a teno-osseous stress response from sustained eccentric load on the middle trap fibers at their spinal attachments.
Take care of yourself during exams! All the best with your finals. 💪
Diurnal variation of pain: No pain for 2-3 hours after waking up. Aggravating factor: right lateral rotation of neck Relieving factor: Back rest Pain scale: 7/10 Type of pain: pin-pointed On examination, Winging of right scapula
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
This is a very rich clinical picture. Now let me put it all together for you properly.
Clinical Analysis - This is NOT Simple Muscle Strain
The combination of findings completely changes the picture. Let me walk through each clue:
Step 1: Interpreting the Clinical Features
| Feature | Clinical Meaning |
|---|---|
| No pain 2-3 hours after waking | Mechanical/postural pattern - pain builds with activity/posture, not inflammatory |
| Aggravated by right lateral rotation of neck | Nerve tension/compression - rotating the neck stretches or further compresses a neural structure on that side |
| Relieved by back rest (unloading posture) | Postural/mechanical load is driving the pain |
| Pain scale 7/10, pin-pointed | Likely nociceptive nerve irritation, not diffuse muscle ache |
| Right scapular winging | This is the KEY finding - points directly to nerve involvement |
Step 2: The Winging - The Most Important Sign
Scapular winging has a precise differential based on direction:
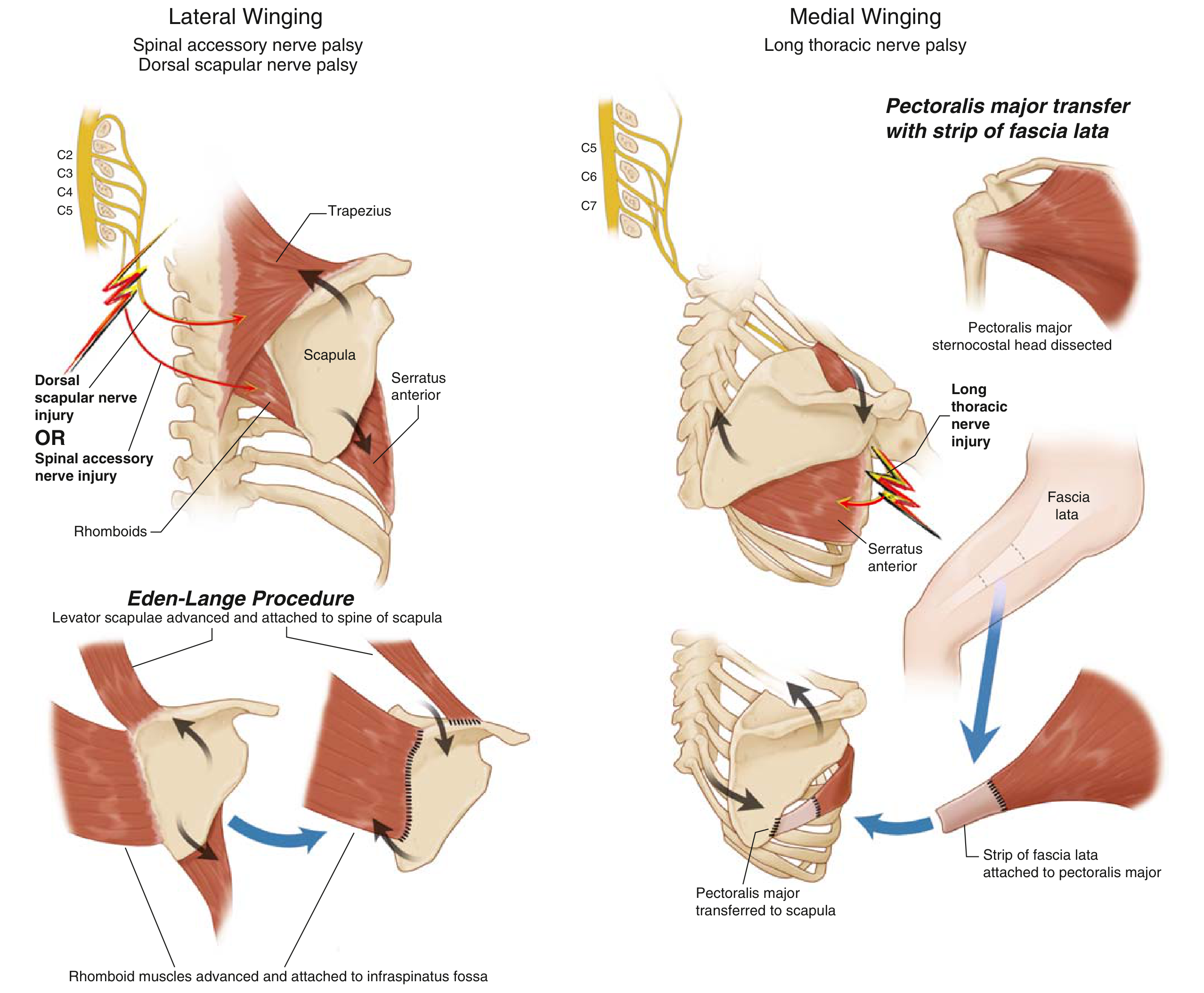
Two Types - You MUST Differentiate:
| Type | Nerve Injured | Muscle Affected | Direction of Inferior Angle |
|---|---|---|---|
| Medial winging | Long thoracic nerve (C5-C7) | Serratus anterior | Inferior angle moves medially (toward spine) |
| Lateral winging | Spinal accessory nerve (CN XI) | Trapezius | Inferior angle moves laterally (away from spine) |
| Rhomboid winging | Dorsal scapular nerve | Rhomboids | Less common |
Memory trick from Miller's: "SWIM" = Serratus Winging Inferior Medial; "TRAWL" = Trapezius and Rhomboid Are Winged Laterally
Since your pain is at the middle trapezius origin and you have right scapular winging, the leading hypothesis is:
Step 3: Working Diagnosis
Most Likely: Spinal Accessory Nerve (CN XI) Neuropathy causing Trapezius Weakness
Here's why all your features fit:
1. Pain at middle trap origin - The trapezius is being overstressed and is in spasm/pain because CN XI is injured and the muscle is neurogenically weakened. The origin fibers are being strained.
2. Right neck lateral rotation aggravates pain - When you rotate the neck to the right, you:
- Stretch the left SCM, but also
- Compress/tension the right posterior cervical triangle where CN XI travels superficially just beneath the skin from the SCM to the trapezius. This mechanical irritation aggravates the already irritated nerve.
3. Scapular winging - CN XI palsy → trapezius weakness → lateral winging
- From Harrison's: "the affected shoulder is lower at rest, scapular winging occurs, and the arm cannot abduct beyond 90°"
- From Bradley & Daroff's Neurology: "Spinal accessory nerve dysfunction results in weakness of contralateral head turning and ipsilateral shoulder elevation... pain in the neck or shoulder is common"
4. Mechanical diurnal pattern - Not an autoimmune/inflammatory process.
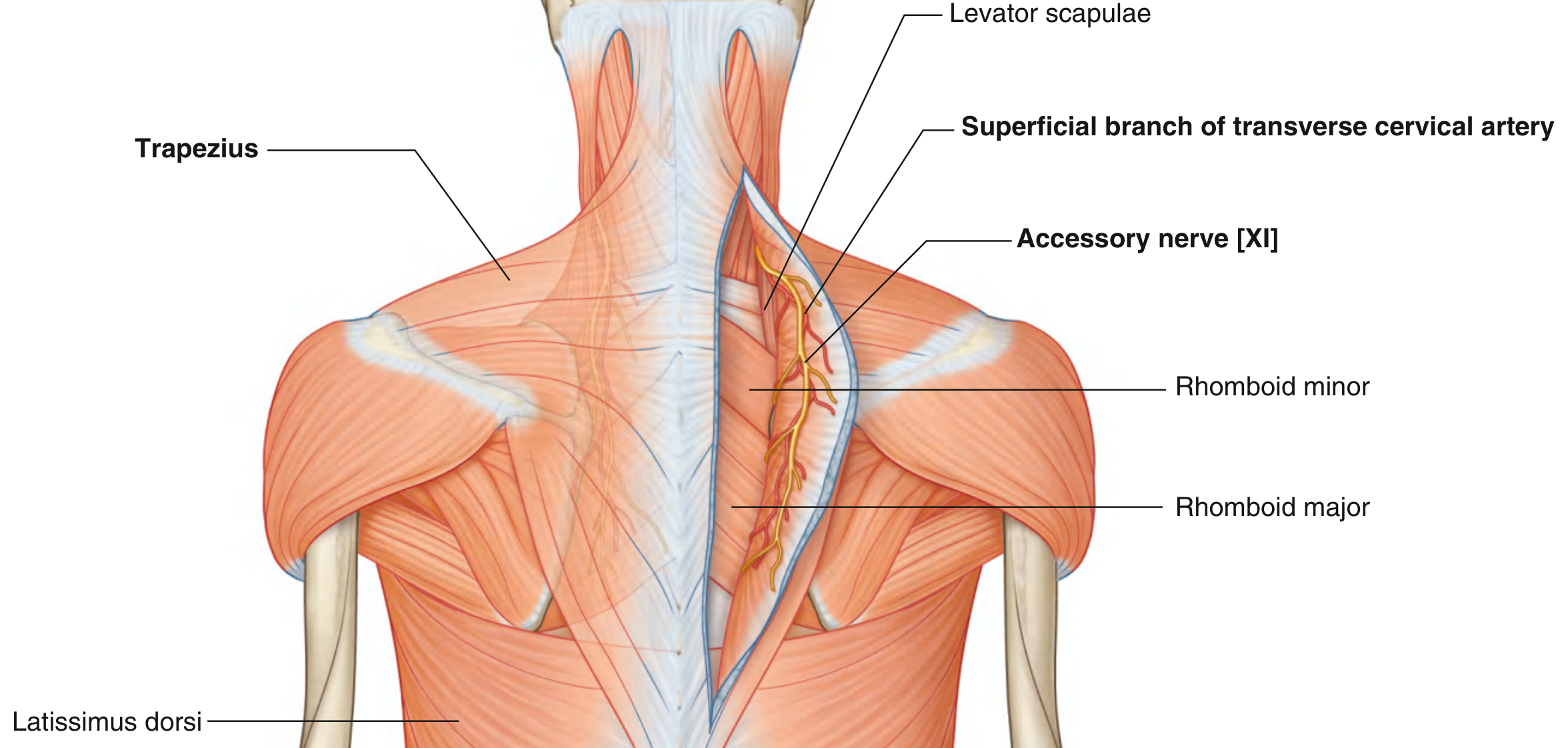
Step 4: CN XI - Anatomy You Must Know
The spinal accessory nerve (CN XI):
- Exits the jugular foramen
- Crosses the posterior triangle of the neck (very superficial - just under skin/fascia) - this is why it's so vulnerable
- Enters the deep surface of the trapezius
- Innervates SCM and trapezius
Why is it vulnerable in your case?
- Prolonged forward head posture during study hours may cause chronic traction/compression on CN XI as it traverses the posterior cervical triangle
- The nerve travels with the superficial branch of the transverse cervical artery along levator scapulae
Step 5: Other Differentials to Consider
| Diagnosis | For | Against |
|---|---|---|
| CN XI neuropathy (top pick) | Winging + trap pain + neck rotation aggravation | No lymph node biopsy/surgery history? |
| Cervical radiculopathy (C3/C4) | Neck rotation aggravates, referred pain to shoulder region | Winging not typically seen |
| Long thoracic nerve palsy | Winging | Serratus, not trapezius, affected - medial not lateral winging |
| Neuralgic amyotrophy (Parsonage-Turner) | Acute nerve pain + winging | Usually sudden onset, not postural |
| Thoracic outlet syndrome | Postural, neck movement | Usually upper limb neurovascular symptoms |
Step 6: Further Assessment You Should Do
As a BPT student, you know what to test next:
- Confirm winging type - Is it medial or lateral? Push-up against wall test (serratus) vs. arm abduction winging (trapezius)
- Shoulder elevation strength - CN XI palsy weakens ipsilateral shrug
- SCM strength test - CN XI also innervates SCM; weakness on contralateral rotation
- Cervical AROM - Document full ROM, which movements exactly reproduce pain
- Neural tension tests - Slump, upper limb tension test (ULTT)
- Neurological exam - Dermatome C3/C4 sensation testing
- Refer for EMG/NCS - To confirm nerve involvement and localize the lesion
Step 7: Management Direction
Since this appears neurogenic (not just muscular):
- Avoid further nerve compression - correct posture, avoid prolonged neck flexion/rotation to the right
- Neural mobilization - gentle cervical SNAG, neural flossing once acute phase settles
- No aggressive trapezius strengthening yet - strengthening a neurogenically weakened muscle worsens it; treat the nerve first
- Electrotherapy - TENS for pain modulation; later NMES/FES once neural recovery begins
- Scapular stabilization - taping to reduce winging while nerve recovers
- Heat, gentle soft tissue release to the posterior cervical triangle (carefully, given nerve proximity)
Bottom Line
Your pain started as "postural trap strain" but the right scapular winging is the red flag that says this is a nerve problem, not just a muscle problem. The most likely structure involved is the Spinal Accessory Nerve (CN XI) as it travels through the posterior triangle of the neck - irritated by prolonged poor posture and aggravated by neck rotation that tensions it further.
You need a proper clinical assessment by a physiotherapist or neurologist - especially an EMG to confirm. Don't push through this with heavy exercise.
Take care of yourself during finals! 🙏
This is a shared conversation. Sign in to Orris to start your own chat.